Hemophagocytic Lymphohistiocytosis (HLH) describes a clinical syndrome of hyperinflammation resulting in uncontrolled and ineffective immune response. It may be primary or secondary HLH. Primary HLH is better defined as "genetic" encompassing both the familial hemophagocytic lymphohistiocytosis (FHL) and also HLH occurring in association with Chediak-Higashi syndrome, Griscelli syndrome type 2 and X-linked lymphoproliferative disorder [1]. FHL is inherited as an autosomal recessive manner. The incidence is of 0.12 cases/100,000 children/year. The incidence is higher in areas where parental consanguinity is common [2]. About 80% of the cases present before one year of age but only 10% are symptomatic in the neonatal period [3]. Five mutations leading to FHL have been identified and the underlying genetic defect described in four of these. Secondary HLH is seen in infection, malignancy, autoinflammatory and metabolic conditions [4].
Secondary HLH can present at any age. It has more variability in severity and outcome, although the clinical picture may be identical to primary HLH. It is seen in the context of infection, underlying autoimmune disorders (where it is often termed Macrophage Activation Syndrome, MAS), some metabolic disorders and malignancy. HLH is reported to occur with a wide variety of infections, including bacterial, viral, protozoal and fungal infections [5,6].
The clinical presentation of HLH in children can be varied and mimic the clinical features of sepsis, malignancy and autoinflammatory disorders. In order to improve the diagnosis of HLH, the Histiocyte Society published diagnostic guidelines in 1991, which were expanded in 2004 [7]. As per the revised criteria, five of the eight criteria are required to fulfil a clinical diagnosis of HLH, although patients with a molecular diagnosis, that is, one of the known FHL mutations, do not necessarily need to fulfil the diagnostic criteria (Table 1) [8].
Table 1: The diagnosis of HLH is established by fulfilling one of the following two criteria. View Table 1
Fever, hepatosplenomegaly and cytopenias are the cardinal features that should raise a doubt of this condition in the pediatricians mind. In addition to this, continued deterioration inspite of maximal care will almost confirm the diagnosis. The presentation could be acute or insidious. Hyperferritenemia, raised transaminases, hypofibrinogenemia and hypertriglyceridemia are suggestive laboratory features. In upto 30% of cases, neurological symptoms and signs like ataxia, encephalopathy, irritability, cranial nerve palsies and seizures are seen at presentation [9]. Fever may be absent in the neonatal period [10].
A 16-months-old male child presented with a history of fever, cough of 1-week duration associated with hurried breathing and refusal of feeds noticed 1 day prior to the admission to the hospital. The child was brought to the hospital in status epilepticus requiring 1st line anti epileptics (midazolam and fosphenytoin). Initial clinical examination suggested septicemia with bronchopneumonia and meningitis with radiological features showing bilateral upper zone consolidation. Child was started on broad spectrum antibiotics (amoxycyllin-clavulinic acid) Initial blood cultures and routine viral markers were sent which were negative (HBsAg, HIV). A possibility of bacterial sepsis was entertained all along and so tests for EBV, herpes virus, CMV were not ordered initially. Lumbar puncture was done which was normal. Initial blood counts revealed haemoglobin of 9.6 gm/gl, total count of 10,500 cells/cu.mm and platelet count of 2.6 lac/cu.mm.
Child on admission to the hospital was ventilated in view of hypoxic respiratory failure. Child on day 3 of illness was noted to have poor response to treatment with bleeding manifestations in the form of melena, worsening pneumonia. Antibiotics were hiked up in view of deteriorating child's condition and repeat blood cultures were done along with extended viral panel consisting of blood cultures for CMV, EBV, Human herpes 6 virus which did not show any positive results. However, repeat blood counts were done which showed a fall in all the three cell lines (HB-6.3 mg/dl, TC-4300 cells/cu.mm, Platelet Count-1.4 lakh/cu.mm). HLH was suspected in view of critically ill condition, splenomegaly and pancytopenia. Serum ferritin levels (1100 ng/ml) and triglyceride levels (380 mg/dl) were estimated which was elevated meeting the revised diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Histopathological confirmation was done using bone marrow examination which showed macrophages engulfing the blood cells suggestive of HLH. In view of rapid progress of pneumonia and an epidemic of H1N1, nasopharyngeal swab was sent on day 3 of admission and in the meantime child was started on prophylactic antiviral therapy (osaltamivir). Child was noted to have positive cultures for H1N1 which was confirmed by the regional H1N1 laboratory. Guarded prognosis was explained to the parents. Child was started on a trial of chemotherapy with etoposide on day 4 of admission after seeking opinion of pediatric haematooncologist. However, on day 5 of admission child's clinical condition deteriorated and child succumbed to the illness (Figure 1).
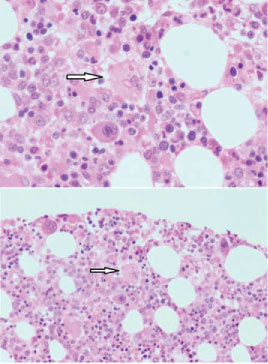 Figure 1: Bone marrow smear showing Hemophagocytosis. Arrow showing Macrophage engulfing blood cells.
View Figure 1
Figure 1: Bone marrow smear showing Hemophagocytosis. Arrow showing Macrophage engulfing blood cells.
View Figure 1
This case fulfilled 6 out of 8 criteria for the diagnosis of HLH. Fever, splenomegaly, cytopenias, hyperferritinemia, hypertriglyceridemia and hemophagocytos is in the bone marrow were the six criteria which were positive in this child. There has been criticism of the HLH diagnostic criteria as being too nonspecific and encompassing many patients on the pediatric intensive care unit with systemic inflammatory response syndrome (SIRS) and multiorgan dysfunction (MODS) [11]. This child had all features consistent with a diagnosis of sepsis and so he was started on antibacterial therapy. Since he did not respond to the best of antibiotics and supportive care, the suspicion of HLH was raised. This is the most important feature of any patient with HLH that has been highlighted by all the authors. Patients presenting in acute state to the general pediatrician or pediatric intensive visit with a clinical picture of likely sepsis (fever, laboratory evidence of inflammatory response, coagulopathy and thrombocytopenia) should be appropriately investigated and managed for sepsis, but the possible diagnosis of HLH should be borne in mind, particularly in the child who deteriorates despite maximal therapy. In addition upto 30% of cases can present with neurological symptoms and signs. This child did have encephalopathy which was a marked clinical feature during his stay in the hospital. Nasal swab suggested H1N1 infection in the regional testing centre. The possibility of meningitis was also thought of and an Lumbar puncture (LP) performed which was normal.
HLH has been described in association with a wide variety of infections. Though a bacterial infection was suspected in this child, all blood culture reports were negative. In this case, a possibility of a bacterial sepsis was entertained all along and so tests for EBV or herpes virus were not ordered initially. However, extended viral panel was sent in the second attempt in view of the downhill course.
Other authors have commented that Herpes viruses, and in particular, Epstein Barr Virus are among the most common infections associated with HLH in children and young adults. Ferritin is a commonly available investigation in most of the laboratories and so this could be done in our laboratory as well, which helped us to pursue the diagnosis of HLH more intensively. In conclusion, a possibility of HLH has to be taken into accounting any child who does not show the expected response to the therapy that has been initiated. Unless there is increased awareness of this condition, many cases may go undetected. Further research into the immunology and molecular diagnostics of HLH may help to identify children at risk, thus allowing for early detection and treatment and hopefully in the future for possible prevention of this condition.
HLH is an acute, rapidly progressive, potentially life-threatening syndrome. Prompt recognition and initiation of therapy is warranted.
HLH secondary to H1N1 is a rare entity and should be kept as a possibility when treating critically ill children especially at the time of epidemic of H1N1.