Constipation is one of the common problems in childhood. Recently, Polyethylene Glycol (PEG 3350) has been suggested as a good alternative laxative to Lactulose as a treatment option in pediatric constipation. The current study aimed to compare the efficacy of two laxatives (PEG 3350 and Lactulose) in the management of functional constipation and evaluate the side effects.
In an open-label clinical trial, 1-13 year-old children with functional constipation according to ROME IV criteria and the presence of RAIR based on anorectal manometry were studied. The patients were randomized to receive either PEG3350 (0.8 g/kg/d) or Lactulose (2 ml/kg/d). Both groups received the medication orally in two divided doses for 12 weeks. They were evaluated clinically at the end of 4, 8, and 12 weeks of therapy, and the end of 16 and 20 weeks from enrolment. At the end of the 12th week, Success was defined as a defecation frequency ≥ 3/week and improvement in stool consistency without painful defecation, as well as encopresis ≤ 1 every two weeks.
We enrolled 43 patients (M20, F23) aged 4.16 ± 2.3 years. At the end of the 12th week, good clinical outcomes were achieved in 95% (PEG) and 77.3% (Lactulose). The PEG group had a significant increase in defecations in a week compared with the Lactulose group (6.26 ± 0.5 vs. 4.94 ± 0.8, p = 0.0001) and a significant decrease in encopresis (35% vs. 10, p = 0.01). PEG achieved defecation without pain (0% vs. 22.7%) and less hard stools (5% vs. 18.2%, p = 0.1). Patients reported less abdominal pain and bloating than children using Lactulose (25% and 0% vs. 68.2% and 27.3%, respectively). We reported a significant relapse because of sudden ceasession of treatment in the Lactulose group (13.6% vs. 5%, p = 0.04) compared with the PEG group.
PEG3350 compared with Lactulose provided a higher success rate, less relapse rate, and fewer side effects in the treatment of constipated children.
Functional constipation, PEG3350, Lactulose, Laxatives
Chronic constipation is a serious common gastrointestinal disorder in children [1]. It is very important to exclude organic causes before making the diagnosis of functional constipation, which is defined by fulfillment of at least 2 items of the ROME IV criteria [2]. Treatment includes a fiber-rich diet, parent's education, toilet training, and pharmacotherapy [3-5]. Osmotic laxatives are recommended to use as the first-choice therapy for functional constipation in children [6,7] Polyethylene Glycol (PEG) is a water-soluble, non-absorbed polymer. It has an osmotic effect on the intestinal membrane due to its high water-binding capacity [8] which leads to fluid retention and softening of stools, so it does not need to metabolize by the colonic flora [9]. It is used to clean colons before diagnostic gastrointestinal procedures in children. Lactulose is a synthetic disaccharide that is fermented by colonic bacteria, which leads to decrease colonic PH, an increase in fecal volume, in addition to, increase colonic transit time. When it is used for a long period, it leads to a change in bacterial colonic flora which reduces its efficacy [10]. There have been recommendations to use low doses of PEG as a choice in the treatment of functional constipated children [11,12]. The current study aimed to compare the clinical efficacy and safety of PEG 3350 and Lactulose in the treatment of childhood functional constipation.
An open-label clinical trial was performed between March 2020 and September 2021, in Tishreen University Hospital in Lattakia. We enrolled children between 1 and 13-years-old who had functional constipation according to ROME IV criteria, newly diagnosed as well as children who were previously treated ineffectively. Exclusion criteria were organic causes of constipation as Hirschprungʹs disease, hypothyroidism, celiac disease, neuromuscular disorders, structural gastrointestinal tract anomaly, and previous surgery of digestive tract.
During the first visit, we recorded the patient's data and did a physical examination with an evaluation of stool retention. Then many tests were performed in addition to anorectal manometry. 19 patients were excluded, 9 patients whose RAIR was absent, 3 patients had neurologic disorders, 4 patients had anal anomalies, 2 patients had celiac disease and one patient had hypothyroidism. The Parents were asked to sign an acceptance for participation in the study. After fecal disimpaction, 43 patients were randomized to receive either PEG 3350 (0.8 g/kg/d) or Lactulose (2 ml/kg/d), orally in two divided doses for 12 weeks, and then we reduced the medication gradually to avoid sudden stopping. We evaluated the patients clinically at the end of the 4th, 8th, 12th weeks of therapy and followed-up at the end of the 16th and 20th weeks of enrolment. Success was defined at the end of the 12th week by a defecation frequency ≥ 3/week and improvement in stool consistency without painful defecation, as well as encopresis ≤ 1 every two weeks.
Patient data were analyzed by IBM SSPS statistics version 20. A p-value of 0.05 was considered statistically significant.
In the current study, there were Forty-three patients (M20, F23) mean aged 4.16 ± 2.3 years. The mean duration of constipation was 11.02 ± 7.8 months. The mean number of bowel movements per week was 2.09 ± 0.6. 81.1% had hard stools and 95.3% had painful defecations and 23.3% had encopresis. 21 patients received PEG and 22 children received Lactulose. One patient dropped out from the study from the PEG group in the 8th week. The efficacy of the treatments at weeks 4 and 8 are shown in Table 1.
Table 1: The efficacy of the treatments at 4 and 8 weeks. View Table 1
At the end of the 12th week, we noted good clinical outcomes in 95% (PEG) and 77.3% (Lactulose) which was statistically significant (p-value 0.03). The PEG group had a significant increase in stool number per week compared with the Lactulose group, (6.26 ± 0.5 vs. 4.94 ± 0.8, p = 0.0001) and a significant decrease in encopresis (35% vs. 10%, p = 0.01). PEG achieved less hard stools (5% vs. 18.2%, p = 0.1) and defecation without pain (0% vs. 22.7%). Follow-up at 16 weeks and 20 weeks were as in Table 2.
Table 2: Follow-up at 16 and 20 weeks. View Table 2
We noted a more relapse in the Lactulose group in patients who stopped receiving the medication without gradually reducing the dose compared with the PEG group (5% vs. 13.6%, p = 0.04) (Figure 1).
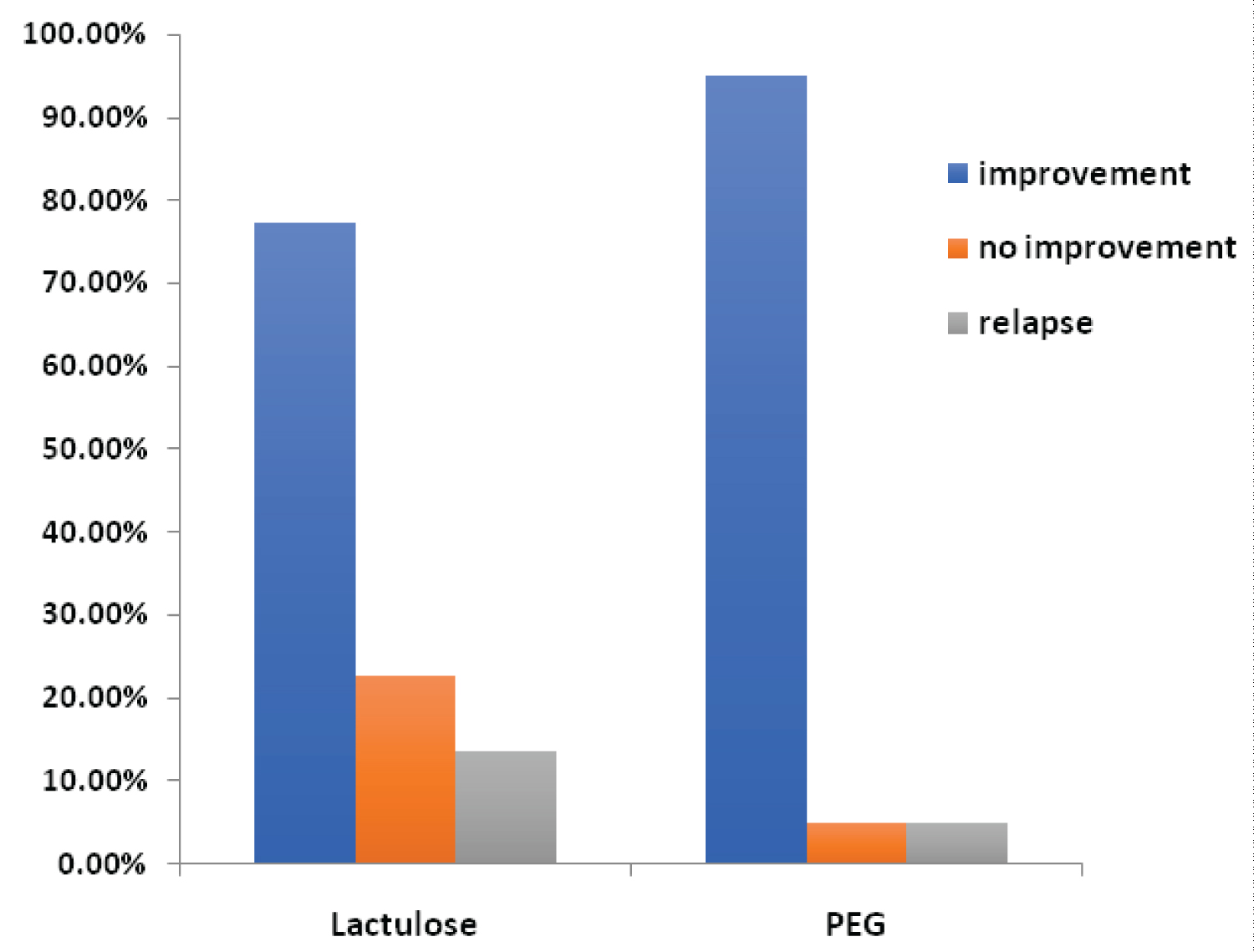 Figure 1: Treatments efficacy and relapse.
View Figure 1
Figure 1: Treatments efficacy and relapse.
View Figure 1
We reported significantly more side effects in patients who received Lactulose compared with the patients who received PEG. The most common adverse effects were abdominal pain and bloating (68.2% and 27.3% vs. 25% and 0% respectively). No serious adverse effects were recorded (Figure 2).
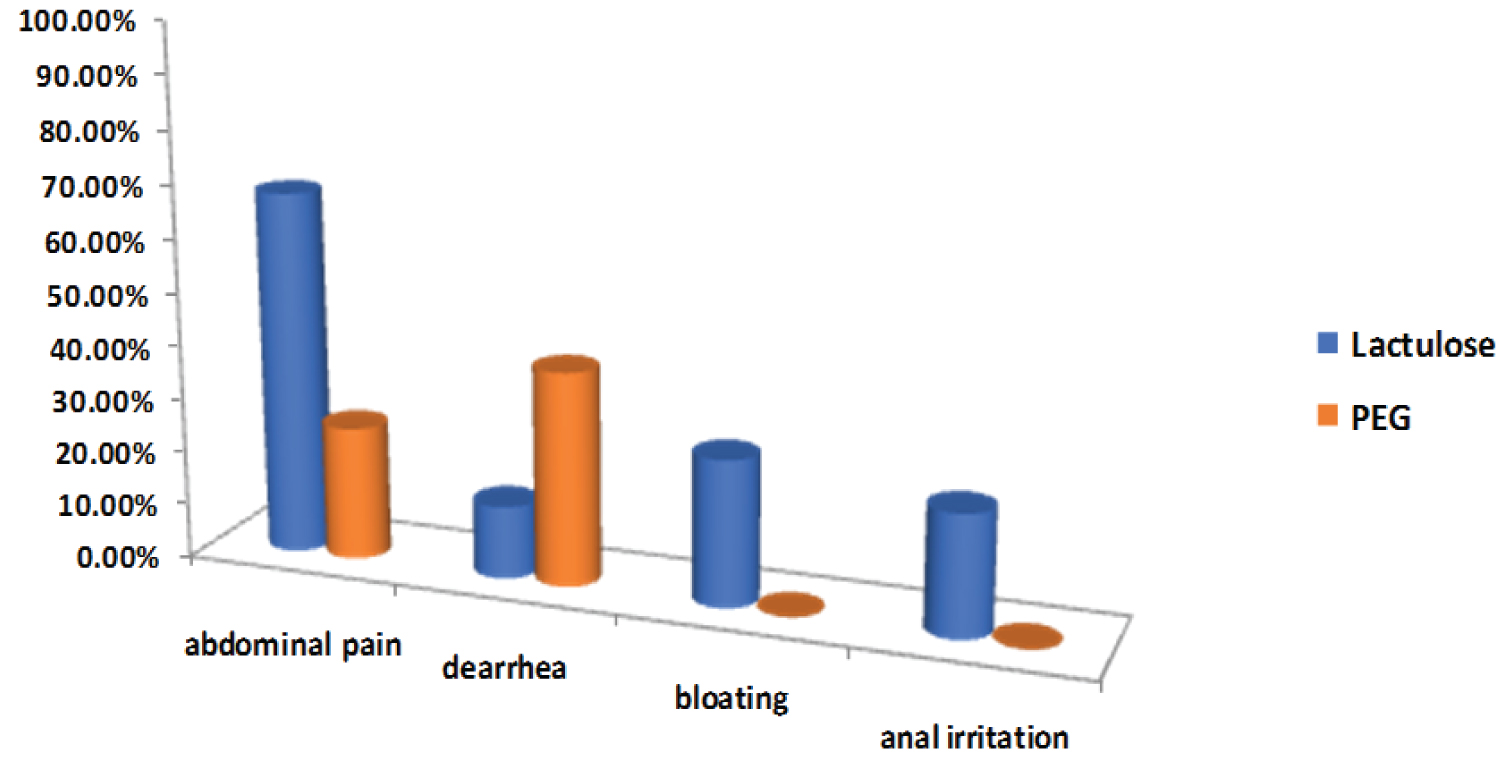 Figure 2: Side effects of the treatments during the study.
View Figure 2
Figure 2: Side effects of the treatments during the study.
View Figure 2
In the current study, 43 constipated patients were treated. Despite both medications resulting in improving the symptoms, the number of patients who were treated successfully was higher in the PEG group, which had a significantly better effect in increasing defecation frequency in a week and decreasing encopresis, in addition, to, decrease hard stools and painful defecation. A relapse was reported in patients who had stopped receiving the medication without reducing the dose, significantly higher in the Lactulose group.
1-7.5% of visits to pediatric clinics and up to 25% of referrals to pediatric gastroenterologist clinics are affected with constipation [7]. The management of functional constipation depends on clinical experience and a half to two-thirds of children with functional constipation has a successful outcome with laxative therapy for approximately 6-12 months [13].
Early and rapid stopping of medication has an important role in recurrence [13]. PEG is used routinely in the long-term treatment of constipated adults. It is shown to be more effective than placebo or Lactulose with fewer side effects [14,15]. Recently, the ESPGHAN and NASPGHAN guidelines recommend PEG 3350 as primary therapy in children who suffer from constipation, and Lactulose can be used if PEG is unavailable [7]. Many trials compared the efficacy of PEG 3350 and Lactulose in pediatric constipation. Jarzebicka, et al. showed that PEG had more defecation per week (7.9 ± 0.6 vs. 5.7 ± 0.5) and fewer hard stools (7% vs. 13%) but it did not evaluate its effect on encopresis, because there were doubts whether parents properly reported in the child’s diary [16]. Saneian, et al. reported that PEG had more than three defecations per week, after one month when compared with Lactulose and Magnesium Hydroxide [17]. Candy, et al. showed that PEG is more effective than Lactulose in increasing the number of defecations per week (9.4 ± 4.56 vs. 5.9 ± 4.29) and in preventing the recurrence of fecal impaction [18].
Voskuijl, et al. compared PEG with Lactulose in the treatment of childhood constipation. Successful treatment was achieved in 56% compared with 29% in the Lactulose group. It achieved a significant increase in defecation frequency and a decrease in encopresis [19]. Gremse DA study found that the stool frequency and form were similar for each laxative [20].
The current study showed that side effects were higher in the Lactulose group. Abdominal pain and bloating were the most common compared with PEG. Mechanisms of colonic fermentation, production of flatus, as well as osmotic effect, and increase in colonic motility account for adverse events when using Lactulose [10,21]. We reported more diarrhea in the PEG group, we think that the additional osmotic effect due to electrolytes especially sodium sulfate played a role in increase diarrhea. Our work confirms the results of the previous studies.
PEG 3350 is more effective than Lactulose. It has a higher success rate and less relapse rate, in addition to its fewer side effects in the treatment of constipated children.
We wish to thank Leen Doya, a doctor in the pediatric department, Aras Abdo, and Victor Al-Khoury, doctors in the pediatric surgery department for their contribution and technical assistance in the research.
None declared.
We can't share patient data due to our hospital's privacy policy, which is concerned with maintaining patient confidentiality and refuses to publish or share data. Also, the informed consent signed by the parents to participate in the study prevents the sharing of information with the non-study researchers.
All parents whose children were studied gave informed consent for the sharing of this research. Ethical clearance for this study was obtained from the Ethical Committee of the University of Tishreen Hospital.
None.
The Authors developed and carried out a sample collection. Literature review, the data analysis and read of the final data were done by authors.