Background: Sepsis is a leading cause of morbidity, mortality and health care utilization for children worldwide. Mortality for children with sepsis ranges from 4% to as high as 50%, depending on the severity of illness, risk factors and geographic location. The majority of the children who died from sepsis suffer from refractory shock and/or multiple organ dysfunction syndromes, with many deaths occurring within an initial 48 to 72 hours of treatment.
Materials and methods: The study is designed as a prospective observational study and was conducted in the pediatric intensive care unit of a tertiary care teaching hospital of west India from Jan 2021 to Jan 2022 for the period of 1 year.
Results: Out of 570 PICU admissions, 25 cases fulfilled the inclusion criteria of septic shock. The mean age of presentation was 24 months. The most common presenting symptom was fever in 18 (72%) followed by vomiting (60%) and breathlessness (60%). Culture-positive sepsis was seen in only four patients (16%), from which three patients had blood culture-positive sepsis and one had urine culture positive. MODS was seen in 15 (60%) of the patients. Patients requiring more than one inotrope, mechanical ventilation, and those who progressed to MODS were significantly associated with mortality.
Conclusion: Septic shock has very high mortality rate due to rapid progression of the disease leading to multi organ dysfunction syndrome and death. Hence early diagnosis and detection of sepsis can reduce the mortality rate.
Historically, the term sepsis was "sepsin" from Greek, meaning "rot, make putrid". It has been used to characterize life-threatening infections usually caused by bacterial pathogens if untreated progress to shock and death [1]. Pediatric sepsis and septic shock still remain major causes of morbidity and mortality worldwide, especially in developing countries. It is a distinct entity from adults and neonatal sepsis, given the unique characteristics of children. The global burden of sepsis study provided global estimates of pediatric sepsis and highlighted the significant burden in Lower and middle-income countries [2]. In 2017, there were an estimated 20 million cases of sepsis worldwide and an estimated 2.9 million global deaths among children younger than 5 years of age. The three most common causes of sepsis-related deaths among children were infections related to neonatal disorders, lower respiratory tract infections, and diarrheal diseases [2].
It is estimated that infection accounts for more than 60% of mortality under-five children. Estimates of the incidence of sepsis suggest that there are more than 42,000 cases annually in the United States and millions worldwide and 5-30% of total sepsis patients develop septic shock [3]. The mortality rate varies in patients from 4% to as high as 50% [4]. Patients presenting with sepsis or septic shock progress rapidly, if left untreated, may rapidly progress to death. It is estimated that it is the 4thleading cause of hospital admission [5]. The severity and high mortality highlight a major challenge in front of the health care system. Early identification and appropriate resuscitation and management are therefore critical to optimizing outcomes for children with sepsis.
Very little data on sepsis epidemiology are available from the scientific literature, particularly in Lower- and middle-income countries where the burden seems to be higher. Hence it is therefore important to address gaps in data availability and research globally [2].
This study was done to analyze the clinical and etiological profile and significance of associated comorbid conditions and the effect of treatment and outcome of children admitted to PICU with septic shock.
A hospital-based prospective observational study was conducted over a period of 1- year after the approval of the ethics committee.
The aim of the study was to analyze the clinical-etiological profile and outcome of the patients admitted in PICU with septic shock. Out of 300 admissions in PICU 25 patients fulfilling the criteria of septic shock were included in our study.
International consensus guidelines 2005 were used to define septic shock as given following [6].
|
Term |
Definition |
|
Systemic Inflammatory response syndrome |
The presence of at least two of the of the following 4 criteria, one of which must be abnormal temperature or leucocyte count:
Or Otherwise explained persistent elevation over a 0.5 to 4 hr. time period OR In children < 1-yr-old, persistent bradycardia over 0.5 hr (mean heart rate < 10th percentile for age in absence of vagal stimuli, Beta blockers drugs, or congenital heart disease)
|
|
Sepsis |
SIRS in the presence of, or as a result of suspected or proven infection. |
|
Severe sepsis
|
It is sepsis plus one of the following- 1. Cardiovascular dysfunction, defined as: Despite > 40 ml/kg of isotonic intravenous Fluid in 1 hour; Hypotension < 5th percentile for age or systolic blood pressure < 2 SD below normal for age Or Need for vasoactive drug to maintain blood pressure Or Two of the following: · Unexplained metabolic acidosis: base deficit > 5 mEq/L · Increased arterial lactate: > 2 times upper limit of normal · Oliguria: Urine output < 0.5 ml/kg/hr. · Prolonged capillary refill time > 5 sec · Core to peripheral temperature gap: > 3 C 2. Acute respiratory distress syndrome, as defined by the presence of a PaO2/Fio2 ratio < = 300 mmHg, bilateral infiltrates on chest radiograph, and no evidence of left sided heart failure. Or Sepsis Plus > = 2 organ dysfunctions |
|
Septic shock |
Sepsis Plus cardiovascular dysfunction as defined above. |
The clinical profile and detailed history of these patients were documented. The Demographic profile, laboratory parameters treatment given records, and the outcome was documented and analyzed.
Data were entered in a master chart using an excel sheet. A Chi-square test was used to determine the association between various variables in survivors and nonsurvivors.
A p-value less than 0.05 were considered to be significant.
Out of 576 patients in PICU during the period of study 25 (4%) cases were diagnosed with septic shock. The mean age was 24.2 months (range from 1 month to 12 years). Most of the children were falling in the age group between 2 months to 24 months. Sixty percent of patients were males. Seventy-two percent of patients were below five years of age. Seventeen patients were from the lower middle class while thirty-two patients were from the upper middle class (Table 1).
Table 1: Demographic details (n = 25). View Table 1
The most common presenting symptom was fever in 18 (72%) followed by vomiting (60%) and breathlessness (60%). Other presenting features were oliguria in urinary complaints and altered mental status (Table 2 and Figure 1).
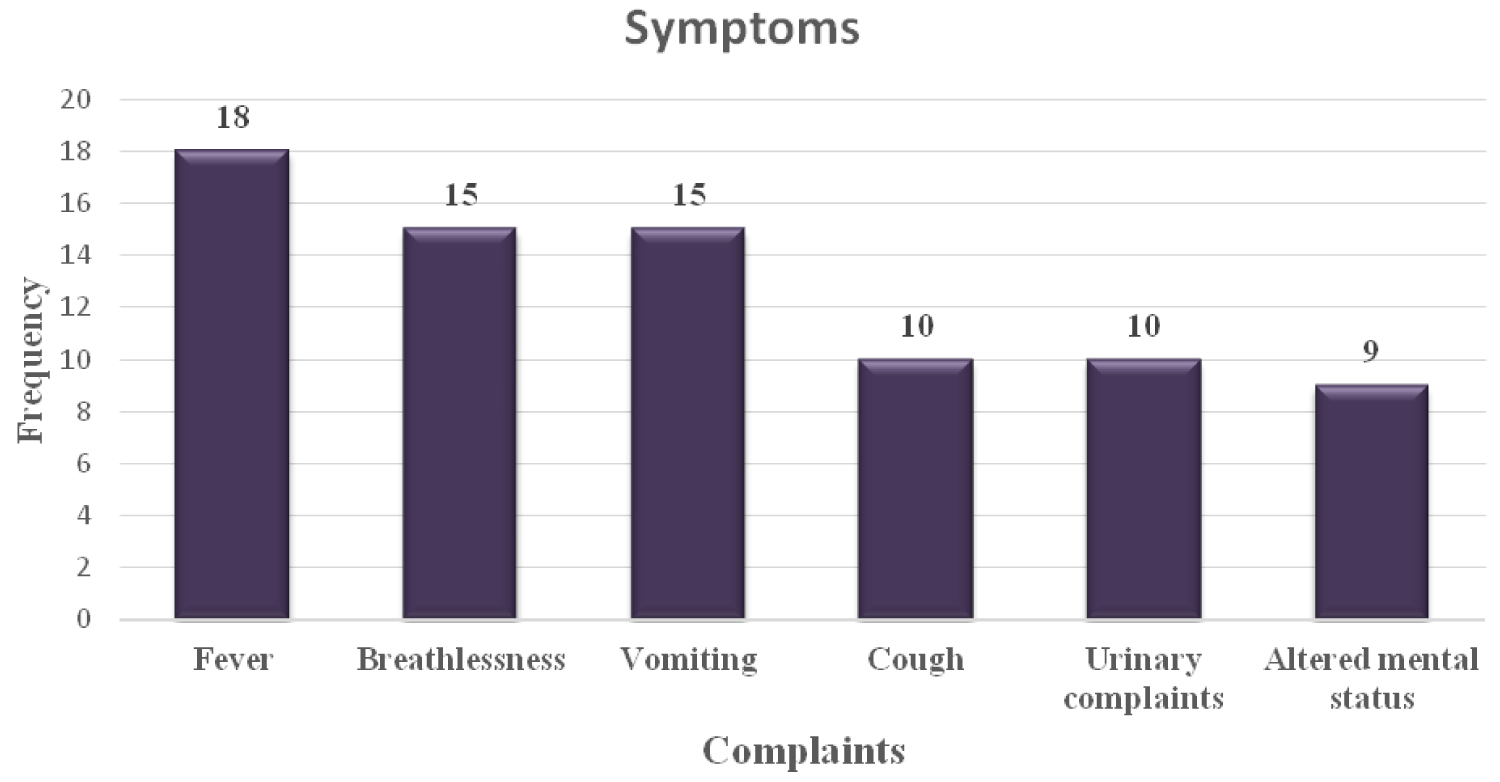 Figure 1: Symptoms.
View Figure 1
Figure 1: Symptoms.
View Figure 1
Table 2: Presenting symptoms. View Table 2
According to lab investigations, anemia was found in twenty (85%) of patients, followed by abnormal leucocyte count and thrombocytopenia. Anemia was defined according to IAP guidelines according to age (Table 3 and Figure 2).
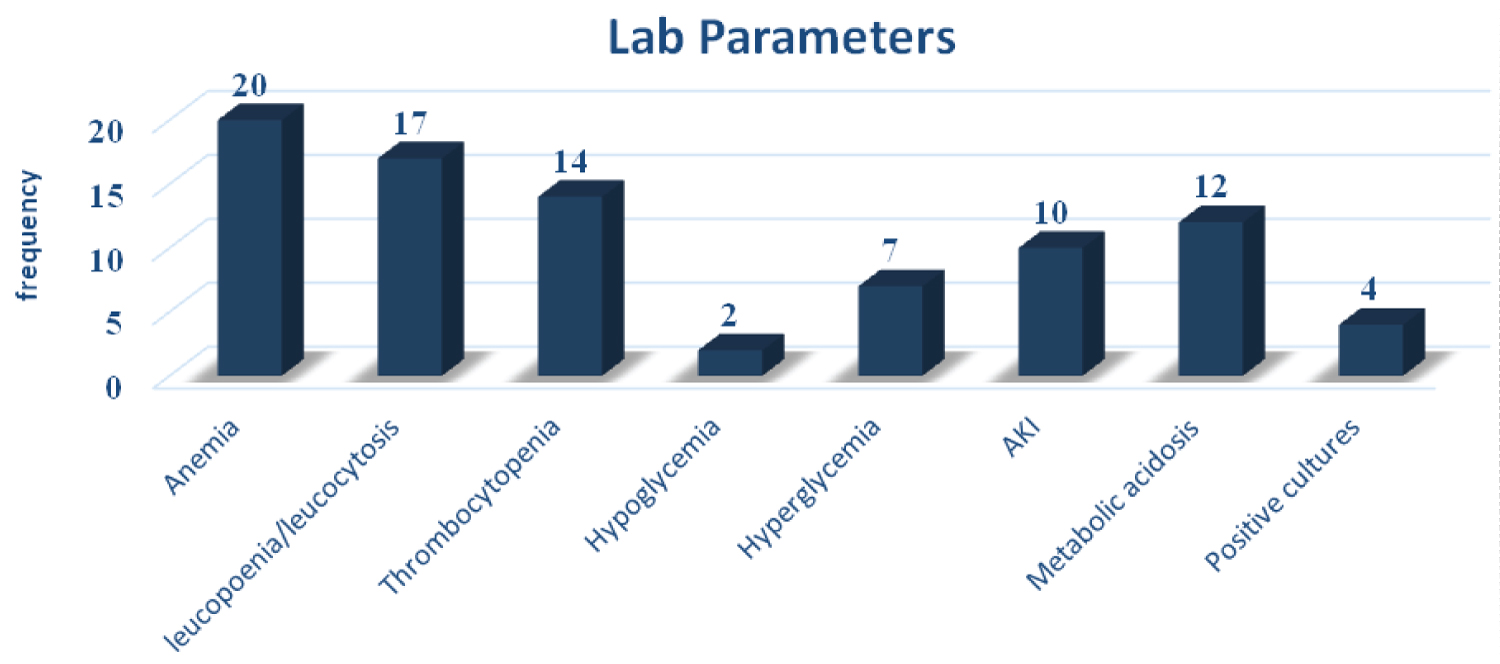 Figure 2: Lab parameters.
View Figure 2
Figure 2: Lab parameters.
View Figure 2
Table 3: Lab parameters. View Table 3
Culture-positive sepsis was seen in only four patients (16%), from which three patients had blood culture-positive sepsis and one had urine culture positive. Interventional procedures like peritoneal dialysis were required in two patients. MODS was seen in 15 (60%) of the patients.
SIRS criteria were fulfilled by sixteen patients (61%) with septic shock. Tachycardia and tachypnoea were common among these patients followed by abnormal leucocyte count (Table 4 and Figure 3).
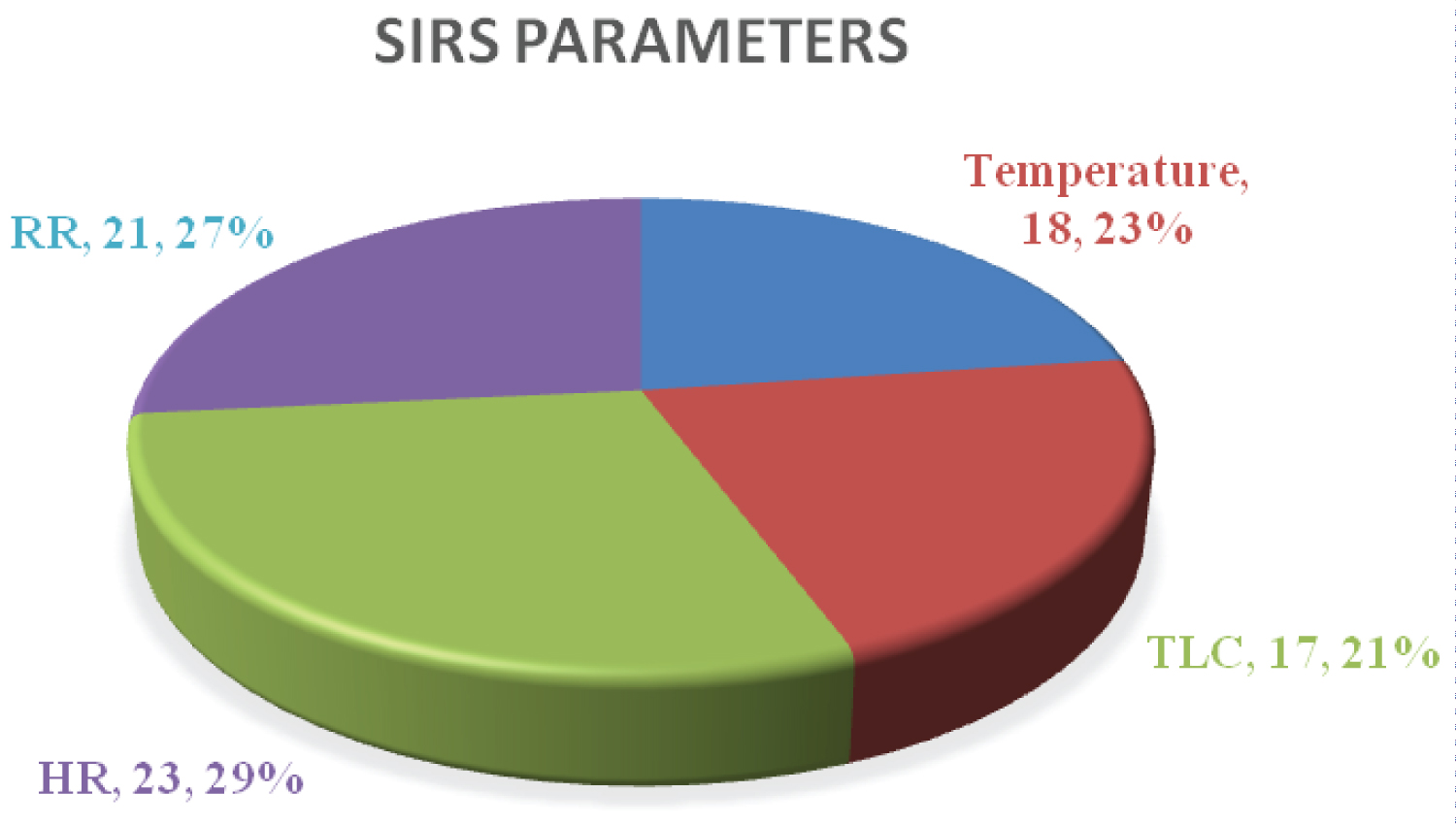 Figure 3: SIRS parameters.
View Figure 3
Figure 3: SIRS parameters.
View Figure 3
Table 4: SIRS parameters. View Table 4
The incidence of septic shock was found to be 4.3% in our study (Table 5). Carvalho, et al. in Brazil reported a prevalence of 9.8% [7]. Age distribution showed that more than 50% of patients were below 5 years of age, consistent to the previous study [8]. There was no major gender-related difference in the occurrence of septic shock, while Bindl, et al. showed male gender has high mortality with sepsis [9].
Table 5: Significance of demographic and lab parameters in outcome of patients. View Table 5
The most common presenting symptom in our study was fever followed by vomiting and breathlessness which was similar to the previous study in India. A study done in Libya reported that most children presented with fever followed by diarrhea and vomiting [7]. A study done from Romania also reported that most children presented with changes in core temperature followed by significant changes in heart rate and respiratory rate [5].
Nearly half of the patients (n = 12) presented with decompensated shock, out of which only two patients survived.
Fourteen patients (58%) amongst nonsurvivors required more than one inotrope, which was statistically found to be significant in our study. Han YY, et al. reported that nonsurvivors were found to be treated more with ionotropic support than survivors [10].
Children with septic shock were found to have highly abnormal laboratory parameters.
Most common hematological abnormality was found to be anemia which was seen in 85 % of the patients, followed by Leucocytosis (65%) and then thrombocytopenia (56%). All three hematological abnormalities were not found to be statistically significant in our study. A study done form Libya, Beamer, et al. observed that Leucocytosis was more common than anemia followed by leucopenia, Thrombocytosis was more common in their study [11].
Forty percent of the patients had deranged renal function tests with raised creatinine and urea. Liver function tests were not done in all patients and hence could not be included in the analysis.
Out of 26 patients, thirteen patients were found to have co-morbid conditions like severe acute malnutrition, spastic cerebral palsy and underlying congenital heart disease. However, it was not found to be significantly associated among the non survivors. Mechanical ventilation was seen as significantly high in non-survivors than survivors who were similar to a study done in Sangli [8].
Three blood cultures and one urine culture was positive (Klebsiella pneumonia was most common), while staphylococcus was found the most common in a similar study in India [8]. The mortality rate in our study was 72% which was similar to previous studies. An Indian study from PGI Chandigarh has also reported 65.8% of mortality [12] due to fluid refractory septic shock. Other Indian studies, from AIIMS Delhi have reported 50% [13], Punjab 47% [14], and Rohtak Haryana 58% [15].
Septic shock has a very high mortality rate due to the rapid progression of the disease leading to multi-organ dysfunction syndrome and death. It has highest mortality among the under five children. Early diagnosis and detection and with standardized protocols, will reduce the mortality.