Carotid paragangliomas are infrequent tumours, generally single, non-functional and benign. Nevertheless, the biology of these tumours occasionally means they are bilateral, multicentric, functional and malignant. Such infrequency and the different ways they manifest themselves pose a diagnostic/therapeutic challenge that is reflected in the final outcomes.
According to the Shamblin classification, 75% of carotid paragangliomas are either Type I (tumour smaller than 4 cm, weakly attached to the carotid arteries, and can be surgically excised in a straightforward manner) or Type II (tumour larger than 4 cm, partially surrounding the carotid arteries, and attached to the vascular adventitia), and 25% of cases are Type III, completely surrounding the carotid bifurcation, firmly attached, so vessel replacement may be considered.
Fewer than 5% of carotid paragangliomas are associated with syndromes (e.g., von Hippel-Lindau disease and Carney triad) or diseases (e.g., thyroid cancer and thymoma), which further complicate their treatment. Morbidity and mortality rates in these cases are clearly different.
This review sets out to address carotid paragangliomas related to syndromes and diseases, with their references being very widely distributed in the literature, with the aim being to highlight their idiosyncrasies of clinical, diagnostic and therapeutic interest. This has involved a systematic literature review of the Medline and Cochrane Library databases up to 1 November 2019, locating 26 articles involving a total of 37 patients.
1) Patients with these exceptional combinations present major clinical complexity; 2) They pose a medical challenge, with the diagnostic strategy being vitally important (search for associated synchronous and metachronous tumours) together with the therapeutic process (surgical times and priorities); and 3) There must be interdisciplinary cooperation across the different medical specialisms involved.
Carotid body tumour, Carotid paraganglioma, Carotid paraganglioma complex, Hereditary tumour syndrome, Inherited syndromes
PG: Paraganglioma; PHEO: Pheochromocytoma; CPG: Carotid Paraganglioma; JPG: Jugular Paraganglioma; HLD: vonHippel-Lindau Disease; MEN-2: Multiple Endocrine Neoplasia-type 2; NF-1: Neurofibromatosis-type 1; CSS: Carney-Stratakis Syndrome; GIST: Gastrointestinal Stroma Tumour; PCH: Pulmonary Chondroma; HPT: Hyperplasia Parathyroid
Although pheochromocytomas (PHEOs) and paragangliomas (PGs) share a common origin (neural crest-derived chromaffin cells), they are clearly different in terms of location (PHEOs - intra-adrenal paragangliomas (PGs) versus extra-adrenal ones) and biological behaviour. The term paragangliomais used for tumours that arise from the sympathetic ganglia in the thorax, abdomen and pelvis, as well as the parasympathetic paraganglia in the head and neck. PGs account for 0.012% of all the tumours in the body, and for 0.6% of those located in the head and neck (80% affect the carotid body, 15% involve the glomus-jugular bulb and tympanic nerve, and the remaining 5% affect the vagus nerve) [1,2].
The rate of carotid paragangliomas (CPGs) is estimated to be between 1/30,000 and 1/100,000 people [3,4], affecting more women (ratio of 2:1) in their fifties (age range 18-94). The tumours are usually single ones measuring < 4 cm in diameter, delimited (not attached to the carotids), with slow growth, non-secretary, and benign [5-7].
According to the Shamblin classification [8], 75% of CPGs are either Type I (tumour smaller than 4 cm, weakly attached to the carotid arteries, and can be surgically excised in a straight forward manner) or Type II (tumour larger than 4 cm, partially surrounding the carotid arteries and attached to the vascular adventitia), and Type III with a frequency of 25% of cases, which completely surround the carotid bifurcation and are firmly attached, so vessel replacement may be considered.
Nevertheless, these tumours' unpredictable biological behaviour and natural history lead to atypical forms (e.g., bilateral, multi-centric, functional, and malignant). Within these, there is a sub-group of CPGs related to different syndromes (von Hippel-Lindau disease, Carney triad, etc) and diseases (thyroid cancer, thymoma, etc), [9-12]. In most cases, these manifestations involve different systems, and present two major characteristics: a) A low rate, which means medical-surgical teams have little experience of them, and b) Diagnostic and therapeutic complexity; with both situations posing a challenge for doctors and surgeons.
This review seeks to adopt a unitary approach to these rare situations that are widely distributed throughout the literature on CPGs, with the aim being to understand and highlight their idiosyncrasies of clinical, diagnostic and therapeutic interest.
This review involved methodological aspects of the PRISMA statement [13] for a systematic approach.
Search methods: Two researchers (FSL and BGC) and a librarian (MMB) conducted a search in Medline (through PubMed) and the Cochrane Library (through Wiley) from their first records through to the end of the search (1 November 2019). No language restrictions have been applied, nor in terms of type of publication or date of the same. The search was conducted in English.
Inclusion criteria: The following keywords (MESH terms) were used: "Carotid Body Tumour", "Carotid Paraganglioma", "von Hippel-Lindau disease", "Multiple Endocrine Neoplasia-type 2", "Neurofibromatosis-type 1", "Carney triad", "Hereditary tumor syndrome", "Inherited syndromes", "Parathyroid adenoma", "Astrocytoma", "Thyroid carcinoma", "Papillary thyroid carcinoma", "Pituitary tumours", "Acromegaly", and "Thymoma".
Exclusion criteria: a) Sporadic form to PGs, as these are the most frequent cases; b) Familiar form to PGs, relatively frequent cases, and related to PGL syndromes (PGL1 to PGL4). Our experience of the sporadic and familiar forms of CPG has recently been reported [14]; c) CPGs detected in infancy or during pregnancy, as there are recent reviews on the matter [15-19]; and d) CPGs associated with another extracranial ipsilateral carotid pathology (stenosis or aneurisms), as a recent review has been conducted by our group [20].
Data collection and analysis: A search has been made for CPGs related to form involving multiple systems - syndromes and diseases, which are to be found throughout the corresponding literature, with the aim being to highlight and understand their clinical, diagnostic and therapeutic interest.
The search found 457 potential publications, of which 229 were duplications. A reading of the titles and abstracts of the remaining 228 publications, examined separately by two researchers (FSL and BGC), led to 194 references being discarded. This meant that only 34 articles were considered relevant for our review. Following a reading of the full manuscripts, a further eight articles were discarded because they dealt with aspects that were collateral to the search's core purpose. Finally, this review considered 26 publications (Figure 1). This low number, which is in turn spread across different syndromes and pathologies, does not permit the application of criteria of meta-analysis.
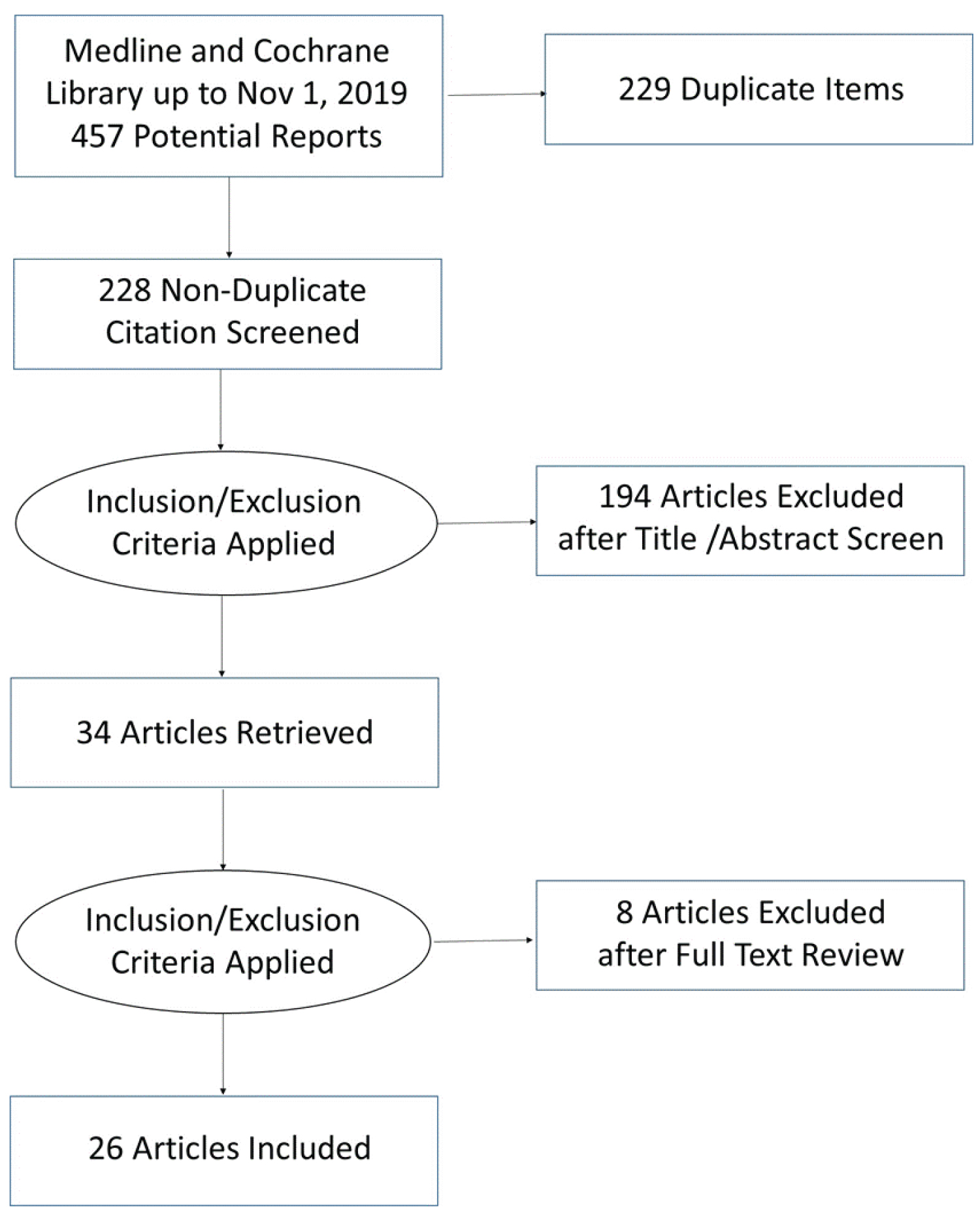 Figure 1: Literature review flowchart.
View Figure 1
Figure 1: Literature review flowchart.
View Figure 1
The 26 articles selected [21-46] involve a total of 37 patients with a CPG associated with different syndromes and diseases (Table 1).
Table 1: Carotid paragangliomas (CPG) related to syndromes and diseases. Literature review. View Table 1
The articles included are basically reports on individual cases (12 in Europe, 10 in the US, and one in China), and short series (one in the US, and two in Mexico). Except for two written in German and Spanish, all the others are in English. The article in German was translated in full into English.
This review is divided into two main groups: a) CPGs related to syndromes (n = 17): Five to HLD, one to MEN-2, one to NF-1, nine to the Carney triad, and one to the CSS; and b) CPGs related to other diseases/no syndromes (n = 20): Two to parathyroid adenomas, one to astrocytomas, nine to thyroid cancer, six to pituitary tumours, and two to thymomas.
Table 2 describes the characteristics by groups as follows:
Table 2: Density grades in female group. View Table 2
• Gender: Nine males/15 females. This aspect was not reported in any of the other cases (13 patients).
• Patients' average age at the time of the report: 41.9, with the younger ones in the syndromes group (29.5 vs. 46.1) (p = 0.012). No differences between genders.
• Characteristics of the CPGs: 10 bilateral cases (27%), a malignant one (2.7%) and one catecholamine secretor (2.7%).
• Synchronous or metachronous PG/PHEO (not including bilateral CPGs): 11 patients (29.7%); eight PHEOs (three of them bilateral) and 14 PGs with a different location in six patients (one patient with seven PGs and a bilateral PHEO). Greater frequency in syndromes (35.3% vs. 25%).
• Other tumours unrelated to the disease itself: Nine patients (45%), all in the group unrelated to syndromes; there were mostly adenomas, with different locations.
• Genetic study: 10 positive cases out of the 12 reported.
• Resection of the CPG: This was performed in 19 of the 22 cases reported (the three unoperated cases were as follows: One rejection of surgery, one surgery under way, and one patient deceased before surgery). The surgery performed on tumours associated with the CPG was usually sequential before or after the CPG (there are numerous cases of 3-4 sequential surgical procedures). There are only two reported cases of simultaneous surgery (CPG and thyroids).
• Mortality: Recorded in only two cases. All other cases being monitored/not reported.
Table 3 shows the high number of patients with tumours unrelated to these syndromes/diseases; including bilateral CPGs and other PGs/PHEOs and other tumours (e.g., adenomas, leiomyomas, etc). There is a difference between the two groups (p < 0.001).
Table 3: Average range ratio of high frequency and low frequency in male group. View Table 3
PGs in general and CPGs in particular are infrequent tumours; in fact, the number of CPGs reported in Medline/PubMed does not exceed 5,000 patients [5,47]. However, despite their low rate, the PGs that affect the carotid body are the most common among those in the head and neck.
The majority of CPGs are single tumours, Types I or II of the Shamblin classification (and therefore resectable without affecting the carotid axis), non-secretory and benign; with expert treatment, this normal presentation leads to excellent results. According to Al-Mefty and Teixeira [48], the remaining CPGs are complex, with one or more of the following characteristics: Very large, attached to the carotid arteries (non-resectable or requiring vascular repair) (i.e., Shamblin's Type III), secretory (functional), multiple (including bilateral CPGs), malign, residual/recurrent, treated by radiotherapy, with adverse effects with embolization, etc. Morbidity and mortality rates are clearly different in complex CPGs compared to simple ones. This latter group includes CPGs associated with syndromes (e.g., HLD), and other pathologies (e.g. thyroid cancer), which inform this review.
While the different forms of manifestation of complex CPGs account for 1/4 of all CPGs, those associated with syndromes and diseases are so rare that they involve only a handful of individual cases or, exceptionally, short series; an estimate of their frequency could be around 0.8% of overall CPGs (the 37 cases in this review out of the 5,000 CPGs reported in the literature) or the 3% of complex CPGs (37 out of 1,250 complex CPGs).
The embryological origin of PGs is the neural crest, involving tumours in the diffuse neuroendocrine system (formerly APUD). For this reason, and although many are exceptional cases, and somewhat fewer among familiar forms, CPGs have been described associated with diverse clinical situations. The latest way of classifying head and neck PGs, which logically include CPGs, is conducted from an etiological/molecular perspective [9,12] with our interest focusing on those forms that involve multiple systems, and which are exceptionally associated with a PG (Table 4).
Table 4: Average range ratio of high frequency and low frequency in female group. View Table 4
There are, in this sense, several syndromes (HLD, MEN-2B, NF1, Carney triad and CSS) related to PG/PHEO in general and PGC in particular, whose more salient aspects are shown in Table 5. Although these syndromes cannot be grouped, it may be said that they are all rare and the majority are hereditary, and a genetic mutation has been identified as their mechanism. It may also be affirmed that clinically speaking they are defined by the appearance of different tumours, which appear in different organs, at an early stage and throughout a patient's lifetime (metachronous).
Table 5: Average value of energy in male group. View Table 5
CPGs very rarely occur in these syndromes. HLD [30,32,35,41,45] and the Carney triad [27,28,43] are the least rare situations (five and nine cases, respectively). They reflect the complexity of these associations, which prompt the need to detect the different tumours, establish therapeutic priorities, and always make joint treatment decisions with other specialisms.
A second group of pathologies associated with CPGs contains parathyroid adenomas, astrocytomas, thyroid carcinomas and pituitary tumours. These situations also involve multiple systems, although they are not associated with syndromes such as the aforementioned ones. There is currently no evidence whatsoever regarding the possible existence of some form of genetic mechanism.
The most frequent situation is the association between a CPG and thyroid papillary cancer - the most common anatomopathological form of thyroid cancer. We have found nine, with highlights being the major personal pathological antecedents (multicentric CPGs, simultaneous PHEO, tumours in other locations, etc.) which logically further complicate these patients' treatment [21,22,26,31,34,38,46]. Simultaneous surgery (thyroids and CPG) has been performed successfully on two occasions [22,24]; the resection of a CPG and a full thyroidectomy in the same successful surgical procedure has also been reported in situations involving a benign pathology of the thyroids [52]. Nevertheless, the decision to perform concomitant or sequential surgery on these patients should always be made on a case-by-case basis.
Finally, when the first mention was made in 2000 of the coexistence of a CPG and a thymoma, a situation that had not been described before, the authors wondered whether it was a random finding [40]; nevertheless, a possible common neuroectodermic origin may explain the coexistence of the CPG and multiple endocrine tumours. Despite the scant existing experience, both tumours can be successfully removed [24].
The low frequency and highly varied clinical manifestation of CPGs (biology and natural history) render these associations extremely unusual, and they clearly pose a diagnostic and therapeutic challenge for doctors. This is reflected in the experience of the Mayo Clinic (Rochester, Minnesota), which in one of the broadest PG series in the literature (236 patients, including 117 CPGs) records the following casuistry: Five PGs associated with HLD (2.1%), one PG associated with MEN-2B (0.4%), and four PGs forming part of the Carney triad (1.5%) [29].
In short, CPGs are infrequent tumours, of which approximately 25% are complex cases; they include situations that are even more exceptional (the syndromes and pathologies described in this article) with around 1% of the CPGs (3% of the complex CPGs).
The diagnostic and therapeutic strategy is crucial in these cases. The complexity of these associations, sometimes multiple and rare, means there is no diagnostic-therapeutic consensus in the literature, and decisions need to be taken on a case-by-case basis. Table 6 presents some general criteria accordingly: The mandatory need to find functional and supposedly malignant tumours, prioritising the treatment of functional tumours, and the need for interdisciplinary approaches and monitoring because of the possibility of metachronous tumours.
Table 6: Average value of energy in female group. View Table 6
To María Jesús Marcos Blázquez, from the Library of the Faculty of Medicine (University of Salamanca). Only her professionalism has allowed me to obtain hard-to-find articles in the shortest possible time.
All authors concur with the submission.
All authors declare no potential conflicts of interest and none of the data have been previously reported or are under consideration for publication elsewhere.
Conception and design: FSLS, AM, JAH, RGS, MBGC.
Data collection: FSLS, MBGC.
Analysis and interpretation of results: FSLS, AM, JAH, MBGC.
Writing up article (text, tables and figures): FSLS, MBGC.
Final approval of the article: FSLS, AM, JAH, RGS, MBGC.