Purpose: Prone positioning (PP) was advocated more than 40 years ago as a means of improving the oxygenation status in patients exhibiting acute respiratory failure (ARF) and acute respiratory distress syndrome (ARDS). The purpose of this meta-analysis is to determine if prone positioning (PP) is a more effective way of treating ARDS patients than supine positioning (SP) in patients that are refractory to conventional mechanical ventilation.
Design methods: Relevant electronic databases were searched for studies that met appropriate inclusion criteria. Key Medical Subject Headings (MeSH) terms were utilized such as: ARDS, prone positioning, supine positioning, mortality, and ventilator-associated-pneumonia (VAP). The meta-analysis was performed using Review Manager (RevMan) Version 5.4.1 and Microsoft Excel. Any studies relating to COVID-19 were excluded at this time.
Results/Expected results: There was no statistically significant difference between PP and SP in terms of mean intensive care unit (ICU) days. PP showed a statistically significant difference over SP for the secondary outcome of mortality. This study indicated that PP had no statistically significant positive effect on VAP cases.
Discussion/conclusions: A glaring limitation of this study is the number of cases as only 4 studies were uncovered that met the criteria for acceptance. Lack of study subjects was another limitation and this can be explained partly by the mindset of practitioners. The use PP is a novel approach to treating ARDS. Practitioner education is vital in expediting the change, with COVID-19 seeming to have become a catalyst. As the amount of research, studies, and education increases, this will allow for creation/modification of policies and procedures that will include PP as a first-line treatment in certain cases.
Acute respiratory distress syndrome (ARDS) has gone by many names in the past such as capillary leak syndrome, non-cardiac hemorrhagic pulmonary edema, and stiff lung syndrome [1]. ARDS has a host of causative factors including infections, drug overdose, oxygen toxicity, shock, aspiration, and pulmonary ischemia [1]. Regardless of the cause, the lungs of patients affected by ARDS undergo similar anatomic changes.
The pulmonary capillaries become engorged with a concurrent increase in the permeability of the alveolar capillary membrane [1]. Interstitial and intra-alveolar edema follows next, as well as dispersed areas of hemorrhagic alveolar consolidation [1]. All of these anatomic changes results in a marked decrease in alveolar surfactant and leads to atelectasis [1].
Progression of the disease leads to rippled hyaline membrane formation along the intra-alveolar walls and leads to intra-alveolar fibrosis [1]. Gross appearance of lungs affected by ARDS are likened to looking heavy and "red", "beefy", or "liver-like" [1].
Due to the anatomic alterations previously listed, ARDS is classified as a restrictive disorder and severe hypoxemia normally develops. Treatment protocols normally call for oxygen therapy, lung expansion measures (e.g., positive end-expiratory pressure (PEEP)), and mechanical ventilation utilizing high rates and low tidal volumes for lung protection purposes [1]. Depending on the severity of the ARDS, a patient being treated with these modalities alone might not be enough and the patient can stay or enter into a state of refractory hypoxemia. Today ARDS is still associated with significant mortality [2].
Prone positioning (PP) was advocated more than 40 years ago as a means of improving the oxygenation status in patients exhibiting acute respiratory failure (ARF) and ARDS [3]. PP is the positioning of the patient in the bed in a facedown orientation [4]. For ARDS patients, PP provides a more homogenous, rather than heterogeneous, distribution of inspired gas [5].
PP also allows for improvement in ventilation-perfusion matching, an increase in end-expiratory lung volume, and helps in limiting ventilator associated lung injury by more uniform distribution of tidal volume through alveolar recruitment and alterations in chest wall mechanics [6]. This provides an increase in oxygenation measurements such the partial pressure of arterial oxygen (PaO2) and the saturation of arterial oxygen (SaO2) [4].
A recent large international epidemiological study showed that roughly 16% of severe ARDS patients are turned prone [7]. There is a component of underutilization of PP in relation to ARDS treatment but the rate of application of the prone position has been increasing throughout the years [8]. The clinical practice of PP is still widely considered a rescue or "last ditch effort" maneuver although its practice should be considered in moderate to severe cases of ARDS regardless of the level of hypoxemia [8].
Prone positioning is a novel approach to treating ARDS patients that are refractory to conventional mechanical ventilation. The proposed question is:
Is prone positioning a more effective way of treating ARDS patients than supine positioning (SP) in patients that are refractory to conventional mechanical ventilation?
The use of PP is a more effective way of treating ARDS patients that are refractory to conventional mechanical ventilation when compared to supine positioning in terms of lessening patient's intensive care unit (ICU) stay, mortality, and cases of ventilator-associated-pneumonia (VAP).
A specific aim is to thoroughly answer the proposed question above. Another aim would be to gain a more detailed understanding of PP and its role in oxygenation and ventilation of patients. Other specific aims are to compare the amount of time spent in the ICU, the number of deaths, and the number of cases of VAP for each modality. The amount of time spent in the ICU is the primary outcome while mortality and VAP cases are the secondary outcomes.
Due to the conducting an actual experiment would be impractical and unethical; the chosen study design to test the hypothesis was a meta-analysis [9]. This allowed for the combining of several quantitative studies into one summary statistic that allowed for a better understanding of PP's effectiveness compared to supine positioning. The electronic databases CINAHL, BioMedCentral, PubMed, The Cochrane Library, and MEDLINE were searched from 1990 through 2021 for pertinent randomized controlled trials (RCTs) and peer reviewed articles. Studies relating to coronavirus disease 2019 (COVID-19) were excluded. The following medical subject headings (MeSH) and key terms were used: ARDS, adults, prone positioning, hypoxemia, oxygenation, ventilator-associated-pneumonia, supine positioning, refractory, respiratory failure, and mortality. The meta-analysis was performed utilizing Review Manager (RevMan) Version 5.4.1 and Microsoft Excel (Table 1).
Table 1: Study characteristics. View Table 1
The studies selected for inclusion were required to meet the eligibility criteria below:
1. The Articles were published studies.
2. The articles measured the effectiveness of PP versus SP in the adult population.
3. The articles measured included effectiveness measures of PP in terms of time spent in the ICU, mortality, and VAP.
4. The patients in the studies suffered from a disease process that caused refractory respiratory failure.
5. The articles performed that appropriate statistical analysis.
6. The articles shall be in English.
7. The date range shall be from 1990 until the present.
8. The subjects are required to have met the Berlin criteria for ARDS.
The Berlin criteria for ARDS are as follows: Timing of onset Within 1 week of a known risk factor, the formal exclusion of hydrostatic pulmonary edema, a PaO2/FiO2 (P/F ratio) of 300 mmhg or less on a PEEP ≥ 5 cmH2O, and bilateral infiltrates not explained by effusions, collapse, or nodules [10].
Studies were excluded if the criteria below were met:
1. Subjects that were not Intubated/tracheotomized and mechanically ventilated were not included.
2. Studies that were not RCTs were not considered for inclusion.
3. Any studies Qualitative in nature were excluded.
4. Any studies relating to COVID-19 were excluded at this time.
5. No studies will be considered that are industry-sponsored and/or industry led.
6. Studies were excluded that were not written/translated into English.
The primary outcome of mean ICU days (Table 2) was 74.2 total for PP and 78 total for SP, showing slight favorability for towards PP. The averages of the mean ICU days follow the same favorability. Table 3 shows a total mortality of the four studies that favors PP versus SP with total mortality of 91 patients compared to 134 patients. The amount of VAP for prone patients slightly favors SP at 20 patients versus 22 for prone (Table 4).
Table 2: Mean ICU days. View Table 2
Table 3: Mortality. View Table 3
Table 4: Ventilator-associated-pneumonia cases. View Table 4
Viewing the forest plot in Figure 1 shows no statistically significant difference between PP and SP in terms of mean ICU days. This conclusion comes with a p-value of 0.98. The I-squared statistic in Figure 1 of 0.000 indicates that there is no heterogeneity and studies used are homogenous [9]. Due to the level of homogeny, the fixed effects model was used instead of the random effects model [9]. Examination of the funnel plot in Figure 2 shows no observed publication bias. The study by Guérin, et al. had the most weight at 61.50% and had the greatest effect on the meta-analysis results for mean ICU days (Table 5).
Table 5: Study weights for mean ICU days. View Table 5
 Figure 1: Forrest plot mean ICU days. View Figure 1
Figure 1: Forrest plot mean ICU days. View Figure 1
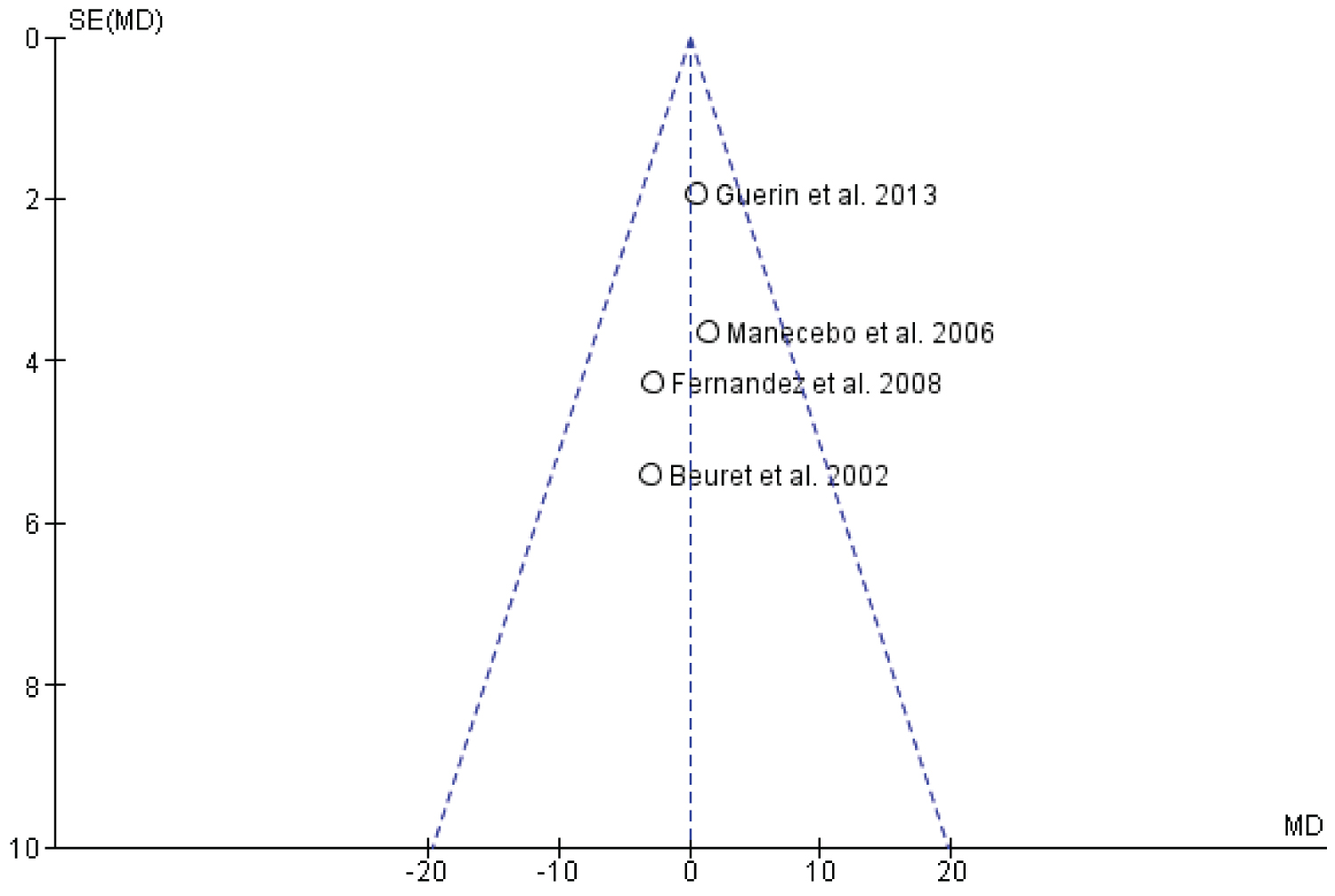 Figure 2: Funnel plot of mean ICU days. View Figure 2
Figure 2: Funnel plot of mean ICU days. View Figure 2
Figure 3 shows that patients had less mortality when PP was utilized. The corresponding p-value of less than 0.05 indicated the results in Figure 3 are statically significant. The study by Guérin, et al. accounted for the most weight in the figure due to the number of patients included in the study. Overall, Figure 4 shows there is no statistically significant difference in VAP between PP and SP patients. The study by Guérin, et al. was not included in these results due to its lack of monitoring VAP cases.
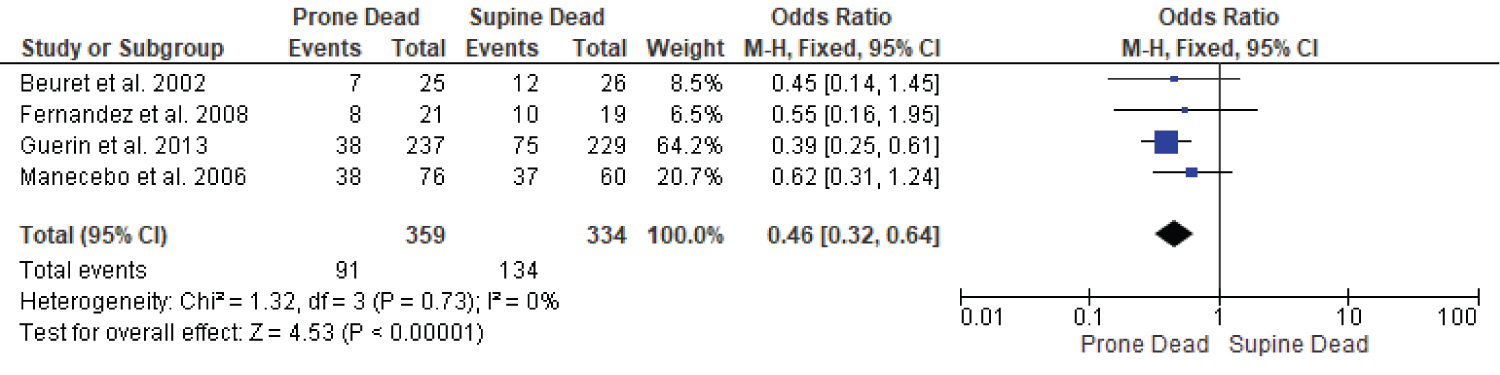 Figure 3: Forrest plot mortality. View Figure 3
Figure 3: Forrest plot mortality. View Figure 3
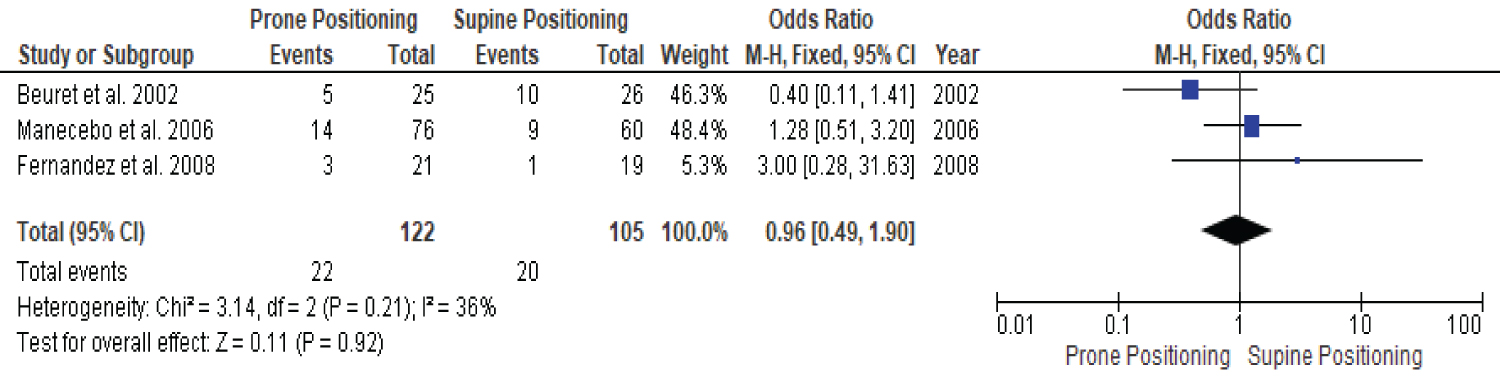 Figure 4: Forrest plot VAP. View Figure 4
Figure 4: Forrest plot VAP. View Figure 4
A meta-analysis done by Sud, et al. showed that PP reduced mortality especially in patients where lung protective strategies were mandated, which corresponds with this study's findings [11]. A comprehensive review by Kallet, et al. showed that PP provided a decrease in mortality of 34% when used with lung protective strategies and no benefit when used without lung protective strategies [12].
The meta-analysis conducted by this study indicates that PP had no statistically significant positive effect on mean ICU days or VAP cases. Mortality was the only outcome conducted by this study that determined that PP has a statistically significant positive effect on ARDS patients that are refractory to conventional mechanical ventilation. This effect appears to be a function of anatomy as putting patients prone allows for more uniform ventilation-perfusion matching, an increase in end-expiratory lung volume, and a more homogenous distribution of inspired gas [6].
A glaring limitation of the study is the number of cases as only 4 studies were found that met the criteria for acceptance. Lack of study subjects is another limitation and this can be explained by the mindset of practitioners. Prone positioning has been classically used a rescue therapy and is not considered as a first-line treatment for ARDS [8]. Changing the mindset of practitioners would allow for a more robust amount of studies and sample sizes. A brief glimpse of COVID-19 studies with regard to PP hints that this change in mindset is possibly occurring. The study by Guérin, et al. lacked VAP information but was included due its sample size, the measuring of the primary outcome of mean ICU days, and the secondary outcome of mortality. Out of all studies it possessed the highest weight at 61.50% for mean ICU days.
There are some inherent challenges that must be accounted for and overcome in the use of meta-analysis. Challenges that have been identified are an assessing the quality and comparability of each study to be included and extracting all statistical results from each of the studies that meets all of the inclusion criteria [9]. Other challenges include publication bias, heterogeneity, and small-study effect [13].
To alleviate the challenges of meta-analysis one can make sure that literature search is conducted in a systematic order to identify all relevant studies, using more explicit and elaborate descriptions and discussions of underlying assumptions [14]. Efforts should also be made to avoid bias by making use of adequate statistical methodology and interpreting results based on context and available evidence [13].
The use PP is a novel approach to treating ARDS that is refractory that (from the meta-analysis) has the potential to be used as a first-line treatment. More studies and research are needed to allow for this change to occur. Practitioner education is also vital in expediting the change, with COVID-19 seeming to have become a catalyst. As the amount of research, studies, and education increases, this will for policies and procedures to be created that will include PP as a first-line treatment depending on factors such as PEEP, FIO2, PaO2, and time on a mechanical ventilator.