Title: Risk Factors of Nosocomial Transmission of Tuberculosis among Healthcare Workers in Kaduna State, North-Western, Nigeria.
Setting: Healthcare facilities providing tuberculosis care service through Directly Observed Treatment Short Course (DOTs) in Kaduna State.
Objective: To identify risk factors of Nosocomial Transmission of Tuberculosis among Healthcare Workers.
Design: A cross-sectional cohort study was used to identify risk factors of Nosocomial transmission of tuberculosis among healthcare workers in Kaduna State.
Result: Involving in providing tuberculosis care services and medical conditions like HIV and cancer is the risk factors to developing tuberculosis among healthcare workers.
Conclusion: Prolong exposure to pulmonary tuberculosis patients, poor provision and effective implementations of tuberculosis infection prevention and control as well medical conditions like cancer and HIV are the risks factors of nosocomial transmission of tuberculosis among healthcare workers.
Recommendation: Implementations of tuberculosis infection prevention and control guidelines as well as pre-placement and periodic screening of tuberculosis should be conducted among healthcare workers providing tuberculosis.
Tuberculosis (TB) is an infectious disease leading to high morbidity and mortality from single germ until the emergence of Covid-19 in 2019 [1]. The disease is caused by the bacillus Mycobacterium tuberculosis (MTB), which affects the lungs, pulmonary tuberculosis (PTB) and other part of the body extra pulmonary tuberculosis (EPTB), the disease spread when an effected person sneeze or cough. One infected pulmonary TB patient can infect on average of 10-20 people every year [2]. It’s confirmed that 85% of all people who developed active TB can be successfully treated with approved TB drugs [1]. TB is curable and preventable infectious disease provided all measured are put in place to adhere to the WHO END-TB strategy [3]. Health care workers are health professionals providing TB care services among TB patient who are 7.5-60% more vulnerable to develop active TB than the general population [4]. It’s confirmed that an estimated 4000 people die from TB every day and nearly 30,000 people develop tuberculosis respectively [1]. Globally south East Asia contributed to (44%) of the global TB burden while African and western medeterinian pacific contributed to (25%) and (18%) respectively [5]. Nigerian alone has contributed to 4.4% of the global TB burden but the actual burden among these cohorts remains undocumented [6]. The burden of TB is higher among low and middle income countries like Nigeria, this is because of their in ability to provide and implement effective TB infection control. Nigerian alone has an estimated annual new TB cases of 590,000 [5]. TB is one of the higher killer infectious diseases from single germs. The disease was confirmed as an occupational disease since 1950s more especially among health care workers with poor infectious control in the facilities [4]. The disease was discover as the disease of poverty, but with the emergence of Human immune deficiency virus HIV, diabetes, unhealthy life styles like alcoholism and cancer the risks of developing the disease is beyond poverty as a single determinant [7]. Infected health care worker stand more chance of infecting other people than the general population due to prolong faced to faced exposure to patients than the general population while discharging professional responsibility. It was reported that one infected pediatrician has infected an average of 15 adult and 09 children age 0-5 within 9 months of infection in Italy [8]. The associated risks factors to nosocomial transmission include but not limited to poverty, poor provision and implementations of TBIC, unhealthy life style like alcoholism, medical conditions like HIV, diabetes and prolong exposure to pulmonary TB patient, despite the WHO ability to developed guideline on TBIC [9]. The identification of vulnerable group to infectious TB is an important strategy to effective TB control, but the science among health care workers is seems to be neglected [10]. The likelihood of nosocomial transmission of TB depends majorly on the patient population, duration of exposure, availability of medical facility and efficiency of TB infected control [11].
Kaduna State is located at the north-western geopolitical zone in Nigeria, with a total coverage area of 46,053 square kilometers. The state has a projected population of 8,397,541 across the 23 LGA in 2017 with an increased to 3.0% of 6,113,503 of 2006 National projection (NBS, 2017). Agricultural activities are the major source of income in the state. A cross-sectional study was conducted to assess the implementation level of WHO guidelines on tuberculosis infection prevention measures in healthcare facilities providing tuberculosis care services through DOTs in Kaduna State, Nigeria.
A Multistage convenient sampling procedure was used to select the study participants. At the first stage, all Local Government Area (LGAs) providing TB care services through directly observed treatment short course (DOTs) were selected. The second stage stratified the local government according to the three geo political zones. The third stage selected 2 LGAs from each of the geological zones considering urban and rural characteristics, and 36 facilities were selected across all the LGAs using a convenient sampling procedure due to insecurity. Healthcare workers providing TB care services in both the public and private health facilities from the selected facilities were recruited.
Data was collected using a questionnaire on the risk factors of tuberculosis among healthcare workers. All data collected was validated through data triangulations method and analyzed using Statistical Package for Social Sciences (SPSS version 23.0) Software. All information was presented in Table 1.
Table 1: Risks Factors of Nosocomial Transmission of Tuberculosis among Healthcare Workers. View Table 1
Ethical clearance was obtained from Lead City University research ethical committee, Kaduna State Ministry of Health Research Ethics Committee and Health Research Ethics Committee of the National Tuberculosis and Leprosy Training Center (HREC, NTBLTC). All data collected was managed under high level of confidentiality and strictly used for the purpose of this study.
A total of 325 respondents were interviewed out of which 171(52.6%) were males, 175(53.8%) are between the ages of 25-34 with mean age of 31.51 ± 8.24. Among these health workers 220(67.7%) are married, 158(48.6%) had NCE/OND degrees, 136(41.1%) had higher degree and only 31(9.5%) has secondary school certificate and below. More than 50% of the respondents were either laboratory personnel 93(28.7%) or community healthcare workers 87(26.8%). The result of this analysis also shows that majority of the respondents 87(26.8%) while only 21(6.5%) were doctors respectively. About 36.6% of the respondents were from the general outpatient’s department, while 46(14.2%) where from the DOTS centre.
The result of this analysis shows that 96.9% involved in providing TB care services, majority has 5 years of training see Figure 1 84.6% knows their HIV status with 5.1% reactive. See Figure 2 17.2% has related medical conditions like HIV and cancer. 36.9 are trained on TBIC, 32.8% were trained in 2012 see Figure 3 91.1% do afford good nutrition, 88.3% do have adequate ventilation, 14.5% do smoke or drink alcohol, 74.2% do use PPE while on duty and 59.4 do screen themselves for TB.
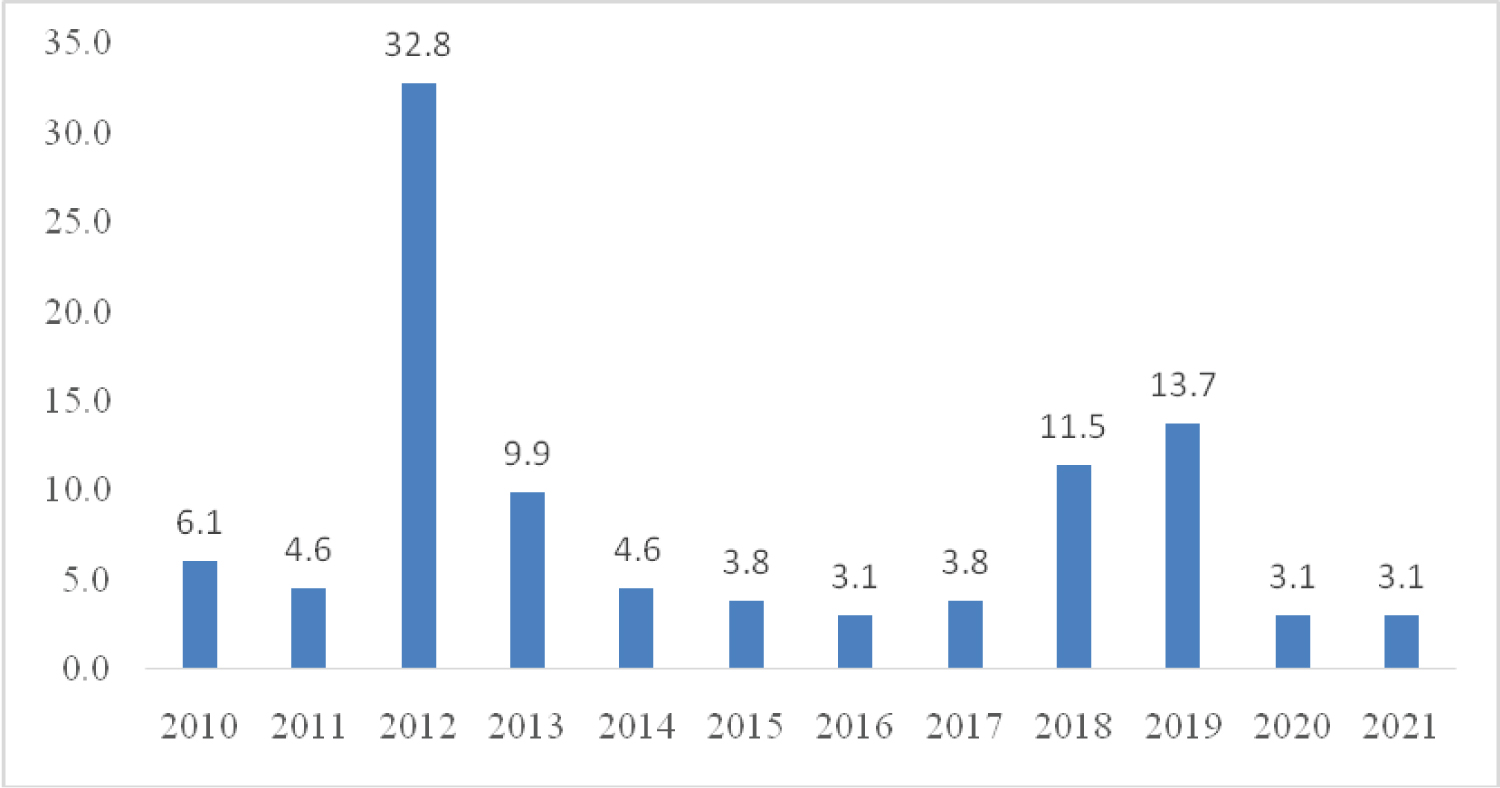 Figure 1: Last time trained on TBIC.
Figure 1: Last time trained on TBIC.
Source: Researcher's Survey (2022).
This shows that among HCWs that knows their HIV status, 5.1% were reactive.
View Figure 1
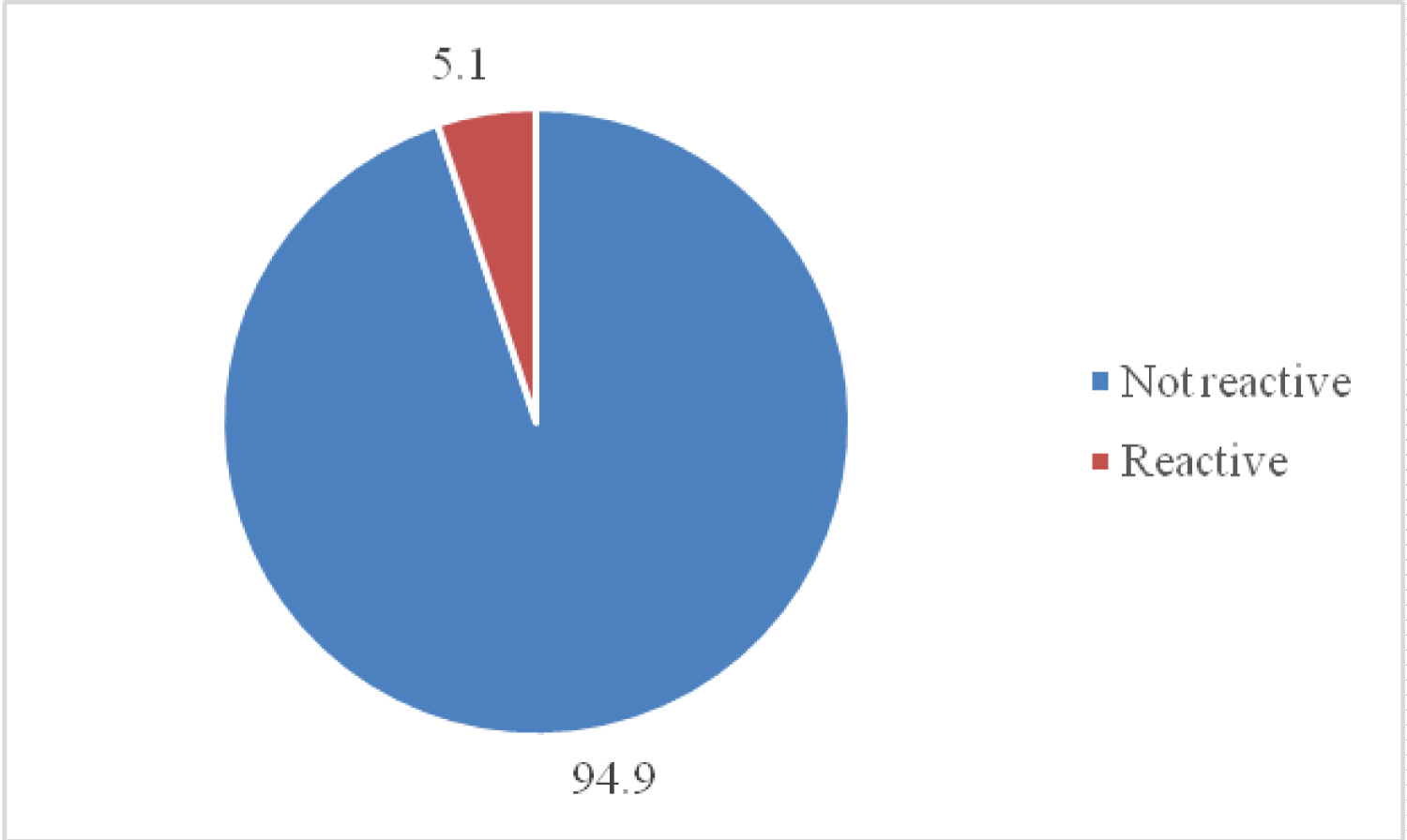 Figure 2: HIV Status among HCWs Positive for TB Years of work experience.
Figure 2: HIV Status among HCWs Positive for TB Years of work experience.
Source: Researcher's Survey (2022).
This shows that of the HCWs involved in providing TB care services majority 17.2% have five years of experience.
View Figure 2
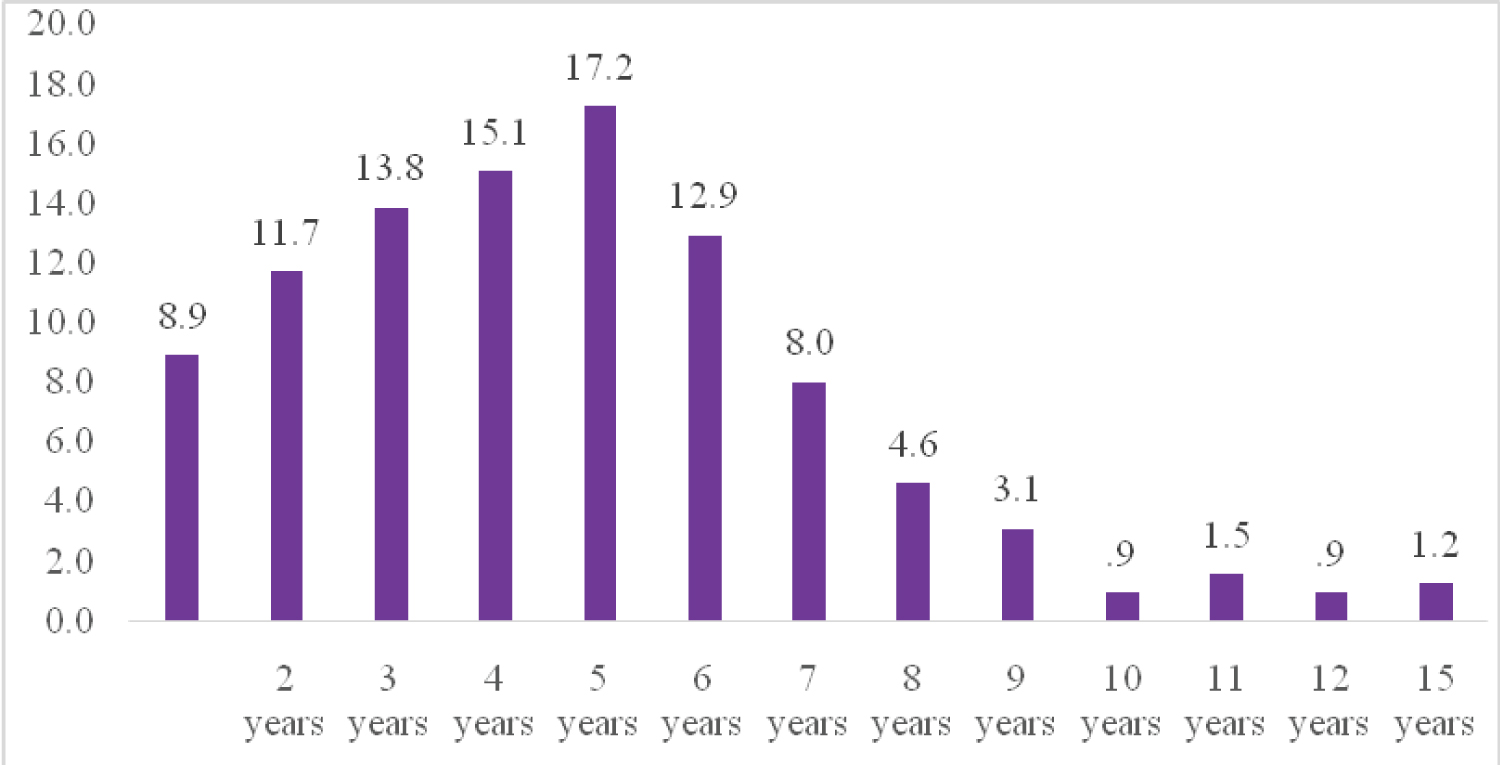 Figure 3: Years of working experience.
Figure 3: Years of working experience.
Source: Researcher's Survey (2022).
View Figure 3
This shows that out of the HCWs that were trained on TBIC 32.8% were trained last in 2012.
The finding of this study is lower than a study that reported 31(16.3%) of administrative staff in Nepal [12]. This result is similar to a study that reported 54(28.4%) of 1-4 years duration of employment in Nepal [12]. This finding is contrary to a study that reported 222(72%) unknown HIV status among HCWs in South Africa [13]. This finding is different to a study that reported 29(10%) HIV infection among HCWs in South Africa [12], this finding is higher than a study that reported 7(4.27%) of training/orientation on TBIC in Nepal [14]. Another study in Nigeria has also reported 2(10 > 0.0%) staff training on TBIC [13]. This findings is higher than a study that reported 69(67.0%) ventilation in Gabon [14]. another study in Nigeria also reported 20(100%) provision of natural and artificial ventilation in South west Lagos Nigeria [15]. This finding is similar to a study that reported 40(86.96%) nonsmokers among HCWs in Indonesia [16]. Another study has also reported 201(96.2%) not smoking among HCWs in Mozambique [16]. This finding is similar to a study that reported 73(70.9%) wearing a mask when with a TB patient in Gabon [14]. This finding is similar to a study that reported 180(55.9%) of skin smear test history in AkwaIbom State, South-West Nigeria [17].
Prolong exposure to pulmonary tuberculosis patients, poor provision and effective implementations of tuberculosis infection prevention and control as well medical conditions like cancer and HIV are the risks factors of nosocomial transmission of tuberculosis among healthcare workers.
Implementations of tuberculosis infection prevention and control guidelines as well as pre-placement and periodic screening of tuberculosis should be conducted among healthcare workers providing tuberculosis.