COVID-19 is a relatively new and rapidly emerging disease. Given current knowledge of the disease process, it is of the utmost importance to gain further insight into its different clinical manifestations. In this report we describe three cases involving Hispanic males with COVID-19 all of whom developed pneumomediastinum during their hospital course. We want to emphasize the importance of this adverse event despite their non-smoking history and the exclusion of positive pressure ventilation. We also question as to whether this may be an underappreciated contributor to worse clinical outcomes especially in the more severely ill patient population. Early detection of pneumomediastinum is important as this could lead to worse morbidity and possibly mortality if left unrecognized despite its usually benign nature.
COVID-19 is an ever-evolving disease that the medical community continues to learn more about daily. It is important to highlight important clinical courses that are not common so that adverse events can be better predicted and treated appropriately. In a retrospective study done in a hospital out of Wuhan, China in February 2020 showed that out of its 99 patients, only one patient had pneumothorax [1]. Later, in March 2020, a literature review published in the American Journal of Roentgenology of more than 900 patients described the incidence of pneumothorax as uncommon or rare [2]. Pneumomediastinum is far less appreciated. A literature search of PubMed reveals only five case reports of pneumomediastinum to the best our knowledge, mostly originating from China, in the absence of positive pressure ventilation [3-7]. Presented below is a case series from a county hospital in Long Island, New York on three patients diagnosed with pneumomediastinum in the absence of positive pressure ventilation. These cases are significant because they all involve non-smokers with no underlying pulmonary disease, the absence of positive pressure ventilation, and delayed presentation (two weeks or more) after hospital admission.
A 51-year-old obese Hispanic male, never smoker with no significant medical history was admitted with three days of cough, chills and dyspnea. On admission, his temperature was 103 degrees Fahrenheit and oxygen saturation was 88% on 100% non-rebreather mask (NRB). He was found to have severe Acute Respiratory Distress Syndrome secondary to SARS-CoV-2 viral pneumonia, with a PaO2:FiO2 ratio of 68. Admission labs revealed normal WBC count, CRP elevated at 10.1 mg/dL, LDH elevated at 439 U/L, D-dimer elevated at 0.40 ug/mL and ferritin elevated at 489 ng/mL. His chest X-ray showed bilateral diffuse infiltrates. He was treated with a course of hydroxychloroquine, azithromycin, and methylprednisolone. He received tocilizumab and convalescent plasma. He continued to require 100% NRB mask to maintain his oxygenation. On day 15 of his hospitalization, he developed sudden chest pain and worsening hypoxemia. Chest X-ray revealed right sided apical pneumothorax and pneumomediastinum (Figure 1). He had a chest tube placed with improvement in his oxygenation. His pneumothorax and pneumomediastinum resolved after which chest tube was removed. He was discharged to rehabilitation facility on oxygen therapy 3 liters per minute nasal cannula. He had a CT thorax done eight weeks later which showed peripheral ground glass opacities with bronchiectasis. No significant underlying bullous lung disease noted. There was also no evidence of residual pneumomediastinum.
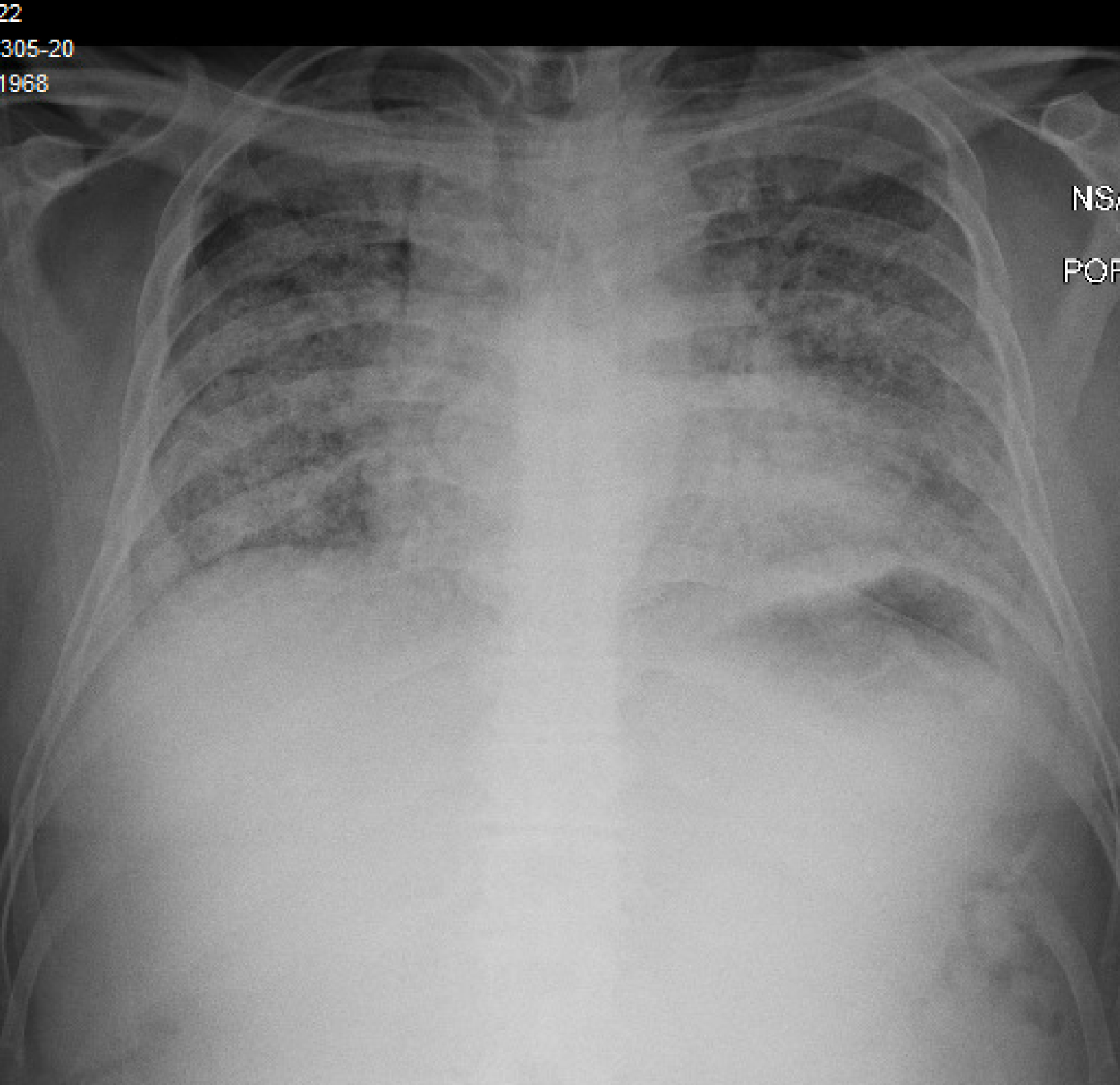 Figure 1: Pneumomediastinum with small right apical pneumothorax.
View Figure 1
Figure 1: Pneumomediastinum with small right apical pneumothorax.
View Figure 1
A 37-year-old obese, Hispanic male, never smoker with no significant medical history was admitted with five days of cough, fever, and dyspnea. On admission, he was afebrile, tachycardic with a heart rate of 108 beats per minute, tachypneic with a respiratory rate of 31 breaths per minute and oxygen saturation was 92% on 100% NRB. He was found to have severe Acute Respiratory Distress Syndrome secondary to SARS-CoV-2 viral pneumonia, with a PaO2:FiO2 ratio of 80. Admission labs revealed normal WBC count, acute kidney injury with creatinine 1.7 mg/dL. CRP elevated at 5.5 mg/dL, LDH elevated at 738 U/L, D-dimer elevated at 1.29 ug/mL and ferritin elevated at 489 ng/mL. His chest X-ray showed bilateral diffuse infiltrates. He was treated with a course of hydroxychloroquine, azithromycin, and methylprednisolone. He received tocilizumab and convalescent plasma. He continued to require 100% NRB mask to maintain his oxygenation. On day 14 of his hospitalization, he had persistent hypoxemia requiring 100% NRB and 6 liters per minute nasal cannula used in tandem. Chest X-ray showed pneumomediastinum (Figure 2). He had CT thorax done which showed complete ground glass opacification of bilateral lungs, diffuse pneumomediastinum, and small amount of pneumopericardium. No significant underlying bullous lung disease was noted. He was managed conservatively, and was noted to have slowly decreasing oxygen requirements. He was discharged home after a 27-day hospitalization on 2 liters per minute nasal cannula oxygen. He was followed up in pulmonary clinic with continued improvement in his symptoms. A repeat chest X-ray done three weeks after discharge showed improved pneumomediastinum and significant improvement in bilateral consolidations.
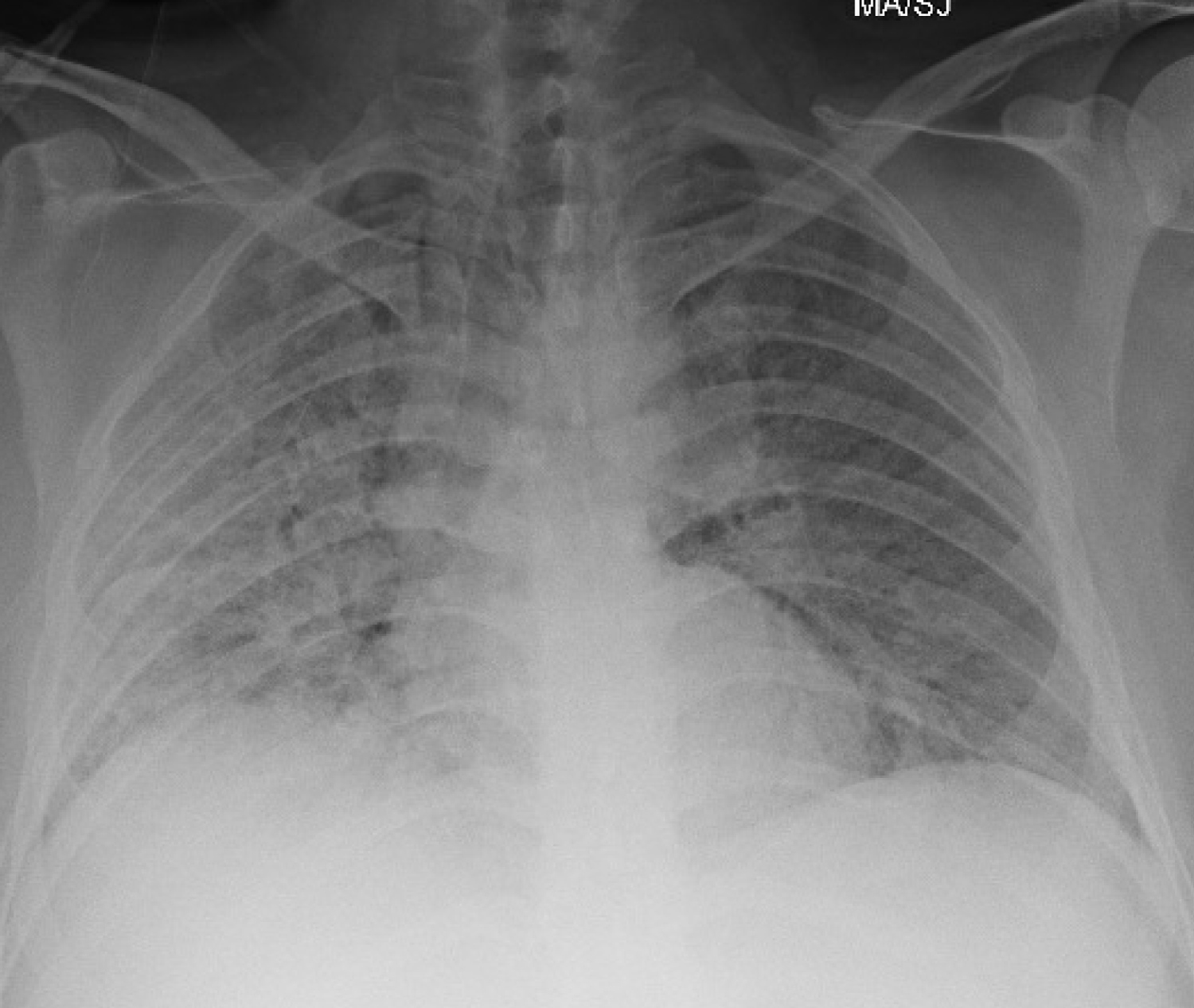 Figure 2: Pneumomediastinum.
View Figure 2
Figure 2: Pneumomediastinum.
View Figure 2
A 34-year-old Hispanic male, never smoker with no significant medical history was admitted with two-week history of non-productive cough, diarrhea, non-bloody, non-bilious emesis and subjective fevers. On admission, he was afebrile, tachycardic with a heart rate of 140 beats per minute, and oxygen saturation 90% on room air and 99% on 4 liters per minute nasal cannula. He was found to have severe Acute Respiratory Distress Syndrome secondary to SARS-CoV-2 viral pneumonia, with a PaO2:FiO2 ratio of 59. Admission labs revealed normal WBC count, lymphocytopenia of 6% and an absolute count of 640/mm3. CRP elevated at 26.9 mg/dL, LDH elevated at 353 U/L, D-dimer elevated at 0.66 ug/mL and ferritin elevated at 478 ng/mL. His chest x-ray revealed bilateral diffuse infiltrates. A CTPE study done by the emergency department to rule out pulmonary embolism revealed patchy bilateral pulmonary consolidation and no evidence of filling defects. There was also no evidence of bullous lung disease. He was treated with a course of hydroxychloroquine, azithromycin, and methylprednisolone. He received tocilizumab and convalescent plasma. His hypoxia worsened during the hospital course, eventually requiring 100% NRB mask and 6 liters per minute nasal cannula in tandem to maintain his oxygenation. On day 18 of his hospitalization, he had persistent hypoxemia with worsening respiratory distress. Patient refused intubation. During the hospital course, he was managed conservatively, and was noted to have slowly decreasing oxygen requirements. On hospital day 36, he developed pneumomediastinum (Figure 3) likely secondary to violent coughing, which eventually improved with conservative management. Chest X-ray done prior to discharge revealed significant improvement in bilateral consolidations and resolution of pneumomediastinum. After six weeks since hospital admission, the patient was discharged home on 2 liters per minute nasal cannula.
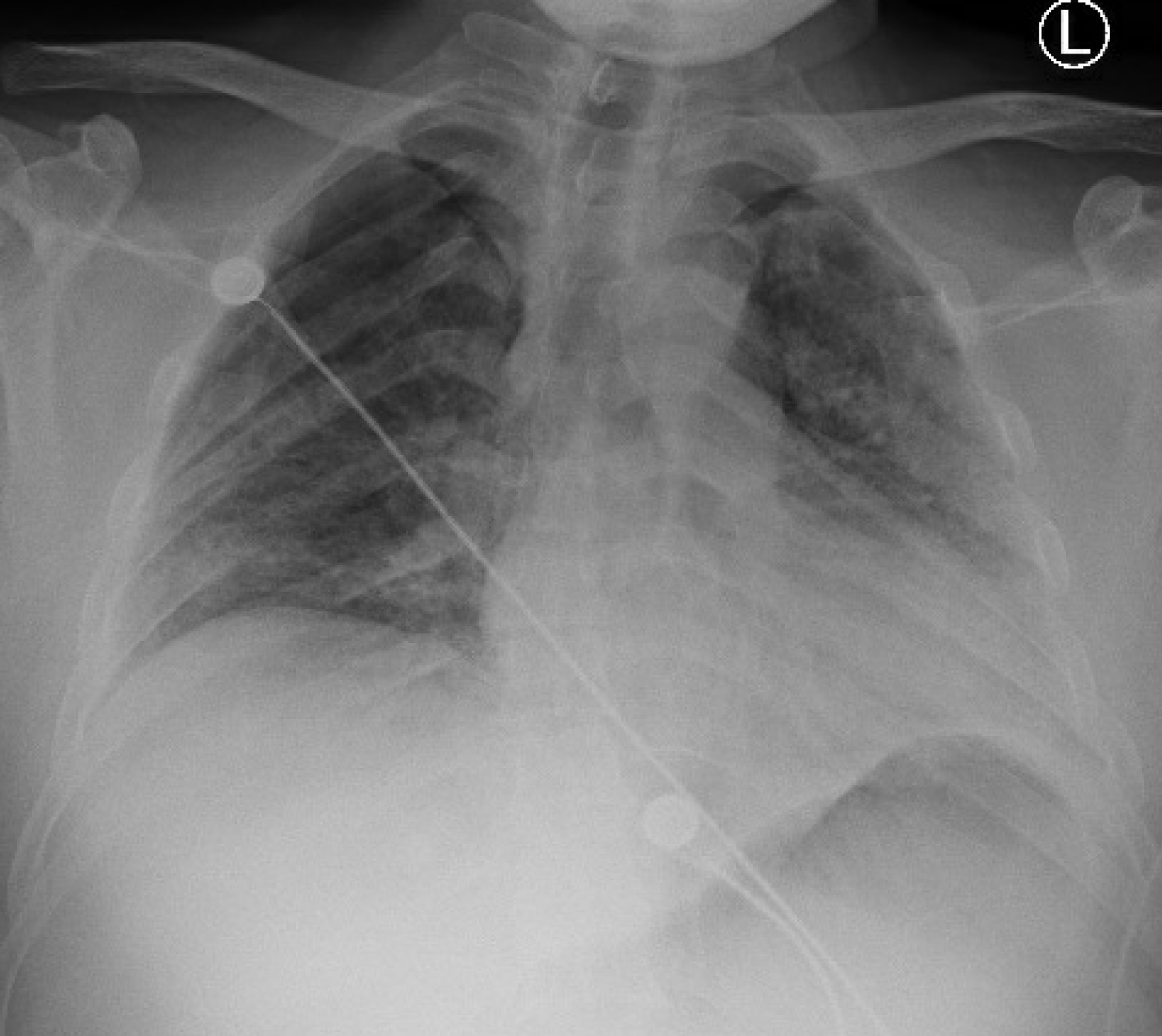 Figure 3: Pneumomediastinum.
View Figure 3
Figure 3: Pneumomediastinum.
View Figure 3
COVID-19 is a complex disease and due to its recent emergence, continued research is being done to fully understand the pathophysiology behind it. Current research shows that pneumomediastinum is a rare complication of COVID-19. With this case series we hope to further educate the medical community about the possibility of this complication. Although usually benign, this can potentially lead to further problems including tension pneumothorax, cardiac tamponade, significant subcutaneous emphysema, or pneumorrhachis [8]. Therefore, the finding of pneumomediastinum in patients with SARS-CoV-2 infection should prompt the physician to closely monitor the patients for possible rapid deterioration. All three of our patients also had sustained sinus tachycardia. We hypothesize that this can be due to either the newly developed pneumomediastinum or due to SARS-CoV-2 infection itself. We also question as to whether pneumomediastinum may be a contributor to worse clinical outcomes seen in more severe cases that may be underrecognized. The exact mechanism for which pneumomediastinum occurs in COVID-19 patients still remains unclear. Further research in this area needs to be conducted as it may be a significant contributor to morbidity and mortality that is unrecognized.
None.
None.
All authors played a significant role in the production of this manuscript.