Background and objective: Hypersensitivity pneumonitis (HP) or extrinsic allergic alveolitis (EAA) is a diffuse parenchymal lung disease due to an inflammation of air spaces and airways secondary to an exposure to organic dust, bioaerosols, microorganisms (fungi, bacteria, protozoa) or certain reactive chemical species. Previous studies done in Sri Lanka recognized that it accounts for about one forth of ILD cases in total. Though the previous studied done in Sri Lanka looked into ILD patients in overall, no single study has looked into the hypersensitivity pneumonitis in details to identify its characteristics and impact on the community. This study was aimed at filling that gap.
Methods: This was an observational descriptive study. To avoid selection bias consecutive patients presenting with clinical radiological and pathological, characteristics consistent with the diagnosis of hypersensitivity pneumonitis were recruited to the study after their diagnosis being reviewed by the ILD MDT, over a period of 12 months from 2019 to 2020. Forty patients had been enrolled to the study by end of this period. Demographic, clinical, radiological and aetiological data were collected with a random identification code for each patient in view of maintaining the confidentiality during data collection. Data was analysed by a separate person who didn't involve with the data collection using SPSS (26 version). Population characteristics studied were described using descriptive statistics such as mean, median and standard deviation and frequency.
Results: Out of Forty patients (N = 40) there were 27 (67.5%) females and 13 (32.5%) males. Mean age of the population was 62.975 years (SD = 11.346 years). Twenty three (57.5%) patients were less than 65 years of which twenty one were aged between 45 to 65 years while two (5%) were aged 35-45 years. Rest of the patients were above 65 years. Shortness of breath (72.5%) and Cough (67.5%) were the most common symptoms on presentation. Mean duration of symptoms was 6 months (SD = 2.4 months). 18 (45%) patients had severe restrictive (FVC less than 50% of predicted) lung disease by presentation, while another 18 (45%) had moderate restriction (FVC of 50% to 80% of predicted). Moderate to severe fibrosis were evident in almost 36 (90%) patients while only 4 (10%) having mild or no fibrosis. Exposure to poultry was identified in 12 cases (30%), while six (15%) had been exposed to paddy. There were 4 (10%) carpentry workers, 4 (10%) textile workers and two (5%) welders in the studied population. In 10 (25%) cases the aetiology was unknown.
Discussion: The majority of patients were in the working age range and were females. There had been a substantial patient delay in seeking medical help for their condition. Most of the affected were having moderate to severe disease clinically and radiologically by presentation. Majority had moderate to severe fibrosis established on presentation. Poultry and paddy were the most common offending agents while occupations like Carpentry, garment industry and welding were associated with the disease occurrence.
Conclusion: Preponderance in females and people of working age, Delayed presentation, established advanced fibrosis and advanced disease on presentation could have potentially influenced the outcome of hypersensitivity pneumonitis in the studied population. Large scale studies are warranted on this regard. Public awareness regarding the disease is essential in terms of minimizing its burden on the community.
ILD: Interstitial Lung Disease; FVC: Forced Vital Capacity; EAA: Extrinsic Allergic Alveolitis
Hypersensitivity pneumonitis (HP) or extrinsic allergic alveolitis (EAA) is a diffuse parenchymal lung disease due to an inflammation of air spaces and airways secondary to an exposure to organic dust, bioaerosols, microorganisms (fungi, bacteria, protozoa) or certain reactive chemical species [1]. The disease can be categorized as acute, subacute and chronic according to the chronicity of the disease [2]. There are no definite estimates regarding its global prevalence or incidence in the current literature and the prevalence and incidence seems to be highly variable on multiple factors [3]. Over 300 aetiologies have been so far identified having potential to cause hypersensitivity pneumonitis in humans [4]. There is no data regarding any gender preference for the disease globally however the prevalence rates increase with age [3]. The exposure might be evident in the history of patients at first instance but at the same time may go unnoticed for unless specifically looked into [4]. The peoples' exposure could be during their occupation or while being engaged in their hobbies [5]. Even though the diagnosis may be straightforward given the right clinical and radiological evidence, the management would be challenging at times in the absence of overt evidence for underlying aetiology [4,6]. Outcome and Prognosis of the disease dependant on causal antigen, the duration of exposure and host response [7]. HRCT evidence of fibrosis, honeycombing and traction bronchiectasis are associated with worse outcomes [8,9]. Previous studies done in Sri Lanka recognized that it accounts for about one forth of ILD cases in total [10,11]. Though the previous studies done in Sri Lanka looked into ILD cases in overall, no single study has looked into hypersensitive pneumonitis in details in order to get an understanding of its characteristics and impact on the community. This study was aimed at filling that gap.
This was an observational descriptive study. To avoid selection bias consecutive patients presenting with clinical radiological and pathological, characteristics consistent with the diagnosis of hypersensitivity pneumonitis were recruited to the study after their diagnosis being reviewed by the ILD MDT over a period of 12 months from 2019 to 2020. Forty patients had been enrolled to the study by end of this period. Demographic, clinical, radiological and aetiological data were collected with a random identification code for each patient in view of maintaining the confidentiality during data collection. Ethical approval for the study was obtained from Ethical Review Committee, Faculty of Medicine, University of Kelaniya, Sri Lanka (P/214/12/2018). Data was analysed by a separate person who didn't involve with the data collection using SPSS (26 version). Population characteristics studied were described using descriptive statistics such as mean, median and standard deviation and frequency.
Out of Forty patients (N = 40) there were 27 (67.5%) females and 13 (32.5%) males. Mean age of the population was 62.975 years (SD = 11.346) years. Twenty three (57.5%) patients were less than 65 years of which twenty one were aged between 45 to 65 years while two (5%) were aged 35-45 years. Rest of the patients were above 65 years. Shortness of breath (72.5%) and Cough (67.5%) were the most common symptoms on presentation. Mean duration of symptoms was 6 months (SD = 2.4 months). 18 (45%) patients had severe restrictive (FVC less than 50% of predicted) lung disease by presentation, while another 18 (45%) had moderate restriction (FVC of 50% to 80% of predicted). Moderate to Severe fibrosis were evident in almost 36 (90%) patients while only 4 (10%) having mild or no fibrosis. Exposure to poultry was identified in 12 cases (30%), while six (15%) had been exposed to paddy. There were 4 (10%) carpentry workers, 4 (10%) textile workers and two (5%) welders in the studied population. In 10 (25%) cases the aetiology was unknown (Figure 1, Figure 2 and Figure 3).
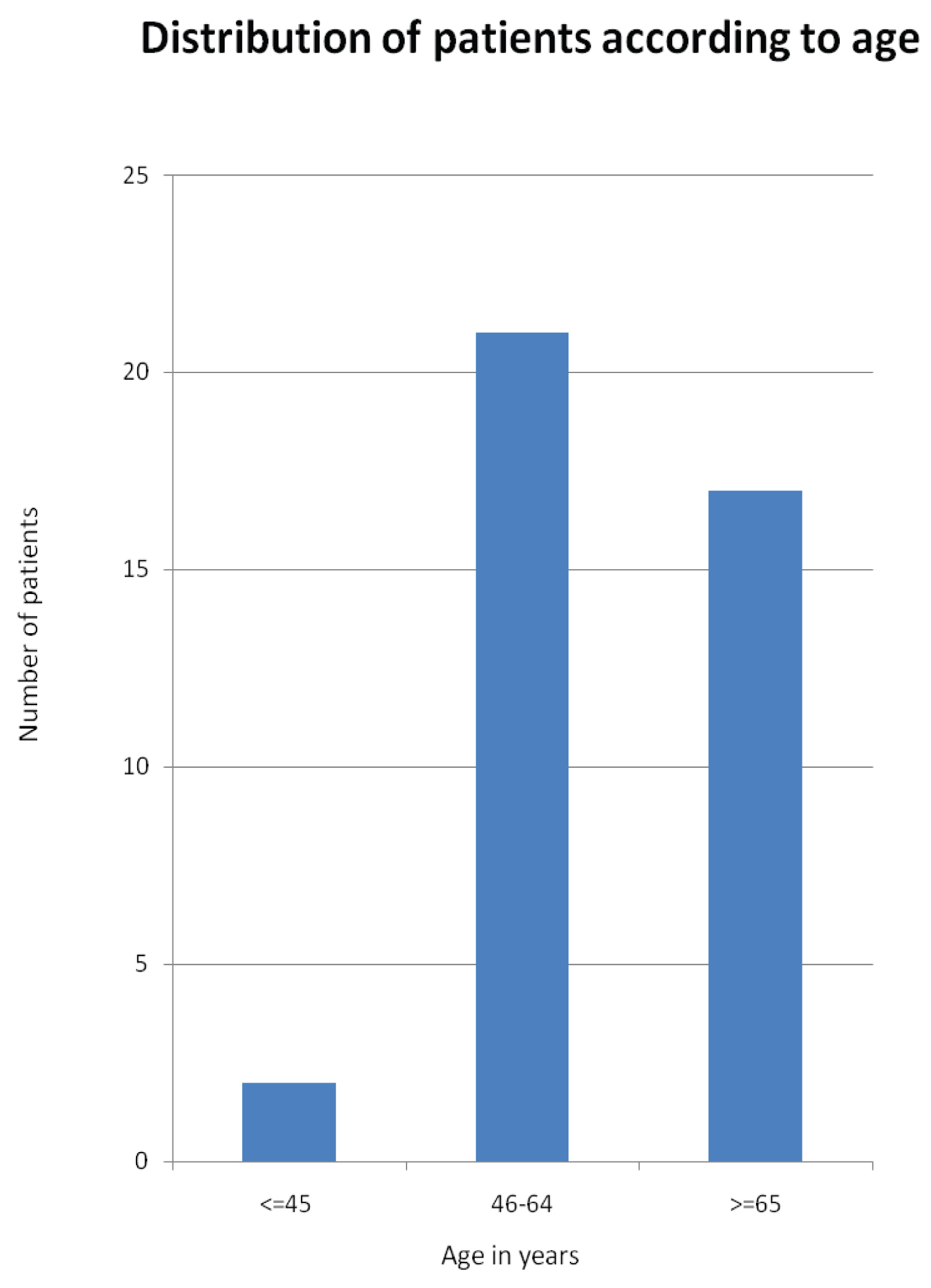 Figure 1: Distribution of patients according to age.
View Figure 1
Figure 1: Distribution of patients according to age.
View Figure 1
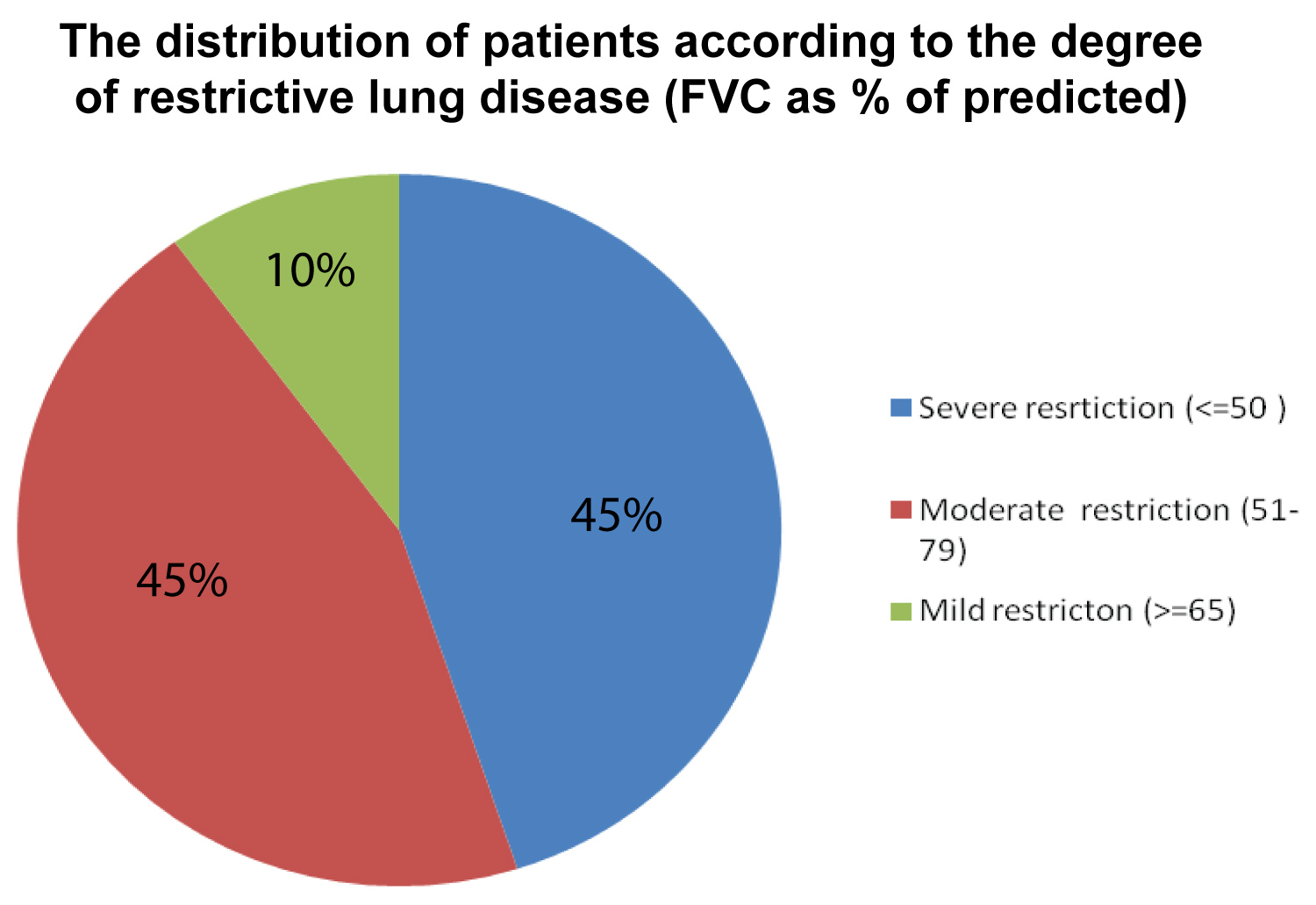 Figure 2: Degree of restrictive lung disease in the study population in view of FVC (% of predicted).
View Figure 2
Figure 2: Degree of restrictive lung disease in the study population in view of FVC (% of predicted).
View Figure 2
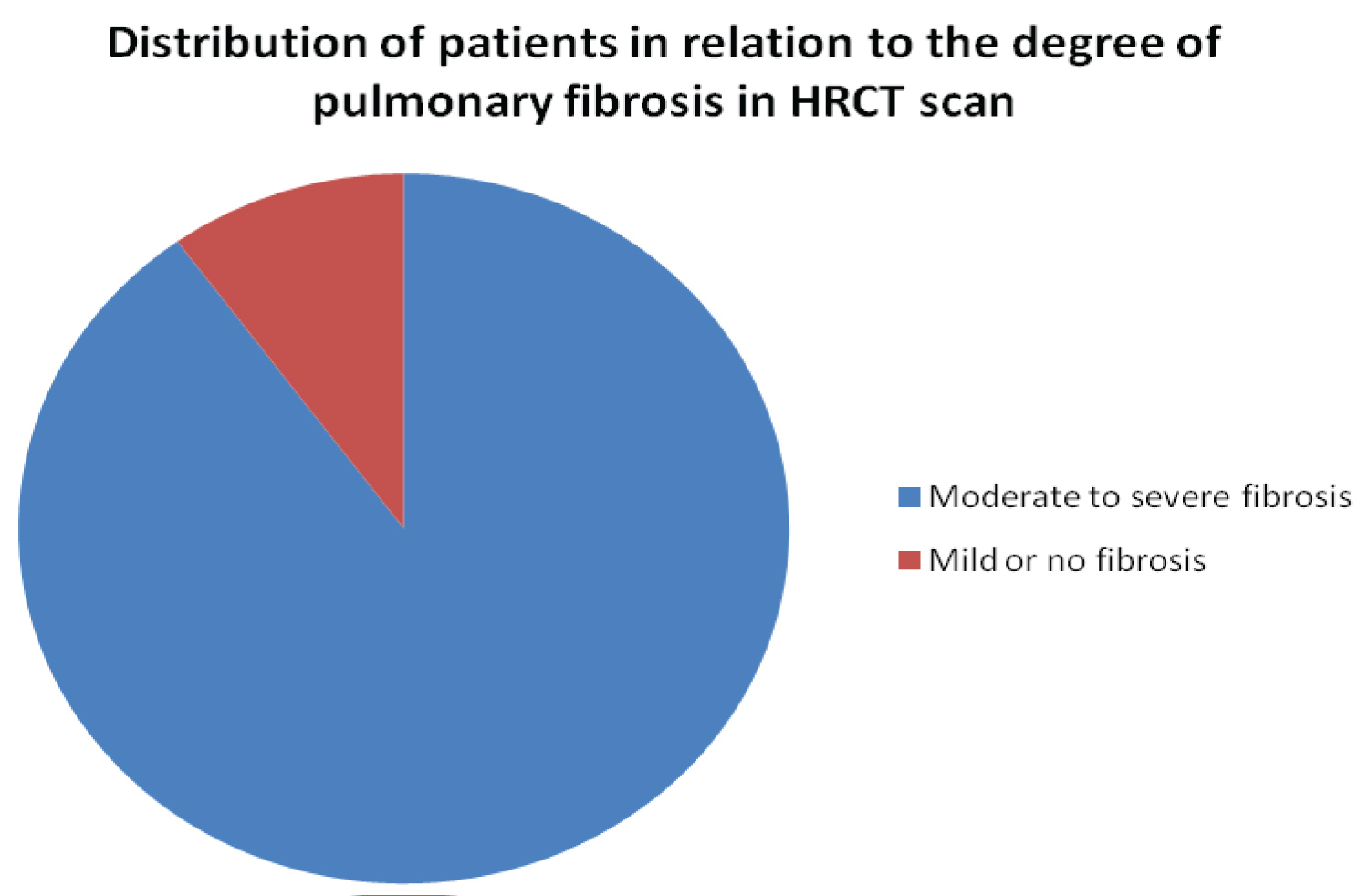 Figure 3: Distribution of patients in relation to the degree of pulmonary fibrosis in HRCT scan.
View Figure 3
Figure 3: Distribution of patients in relation to the degree of pulmonary fibrosis in HRCT scan.
View Figure 3
The majority of patients were in the working age range and were females. Female preponderance has been observed in previous similar studies [12-14].
There had been a substantial patient delay in seeking medical help for their condition in the studied population. This has been observed in another similar study done recently in India [12,13] which shared more or less similar socioeconomic background to Sri Lanka as its closest neighbour. This could have been partly related to lack of awareness regarding the disease condition among the studied population which needs further evaluation.
Most of the affected were having moderate to severe disease by presentation both clinically and radiologically. This could have been partly accounted by the substantial delay in their presentation to the medical service. Previous studies have shown that repeated exposure to the offending agent long term leads to progressive decline in lung function [15].
Majority had fibrosis established on presentation accounting for more cases of chronic HP subtype over the other two subtypes (acute and sub acute). This has been the case in another recent study done in India [16].
Poultry was the most common offending agent identified in the study. Avian precipitant has been one of the most common aetiological agents behind hypersensitivity pneumonitis cases in previous studies of this nature [17].
Preponderance in females and people of working age, delayed presentation, established fibrosis and advanced disease on presentation could have potentially influenced the outcome of hypersensitive pneumonitis in the studied population. Large scale studies are warranted on this regard. Public awareness regarding the disease is essential in terms of minimizing its burden on the community.
The study could have enrolled more cases to increase the power of the study. The exposures of the patients could have analysed in view of occupational vs. non occupational to get a more understating regarding the disease correlation with various exposures.
None.