Background: The TMPRSS2 protein is an entry pathway for SARS-CoV-2, its expression is up-regulated by testosterone. Men have 7 to 8 times higher serum testosterone than women. We propose that patients hospitalized with COVID-19, with higher levels of testosterone, have worse outcomes than those with lower levels.
Methods: A prospective, observational analysis of patients over 18-years-old with COVID-19 admitted to the internal medicine department in Mexicali's General Hospital from January to April 2021.
Results: 49 patients included, 32 men with a mean free testosterone of 2.95 pg/ml; 17 women with a mean of 1.08 pg/ml (p = 0.0002). 16 patients survived, with a mean of 3.21 pg/ml while 33 patients died with a mean of 1.82 pg/ml (p = 0.007). In the male subgroup, the mean of survivors was 3.95 pg/m, in non-survivors was 2.43 pg/ml (p = 0.017). In women, the survivors mean was 1.85 pg/ml while in non-survivors it was 0.66 pg/ml (p = 0.01).
Conclusions: Our study showed that hospitalized patients with COVID-19, with lower levels of free testosterone have worse outcomes than those with higher levels.
Free testosterone, Gender, Mortality, TMPRSS2, SARS-CoV-2
In recent months, humanity has been marked by the pandemic that originated in Wuhan [1], and our community has not been exempt from this health crisis. The infection from SARS-CoV-2 can present itself has a minor, moderate or severe disease, including acute respiratory distress syndrome (ARDS), septic shock, multi-organ failure and even death. The virus entry point is through the mucosa, then the alveolar epithelium where it binds to the receptors of the angiotensin converting enzyme II (ACE-2) and the union protein TMPRSS2 [2].
Respiratory infections always have a worse outcome in men, this has been observed since SARS (2003) which had a fatality rate of 21.9% in men versus 13.2% in women [3]; more recently, MERS (2012) had a mortality of 53% in men compared to 23% in women [4]. Nasir, et al. has observed that generally speaking, men have worse outcomes in any infection [5].
Worldwide, one of the main risk factors for severe COVID disease was the male gender, with different publications even reporting the estimated risk related to gender; Jin, et al. claim that men with COVID-19 had 2.4 times more chance of dying compared to women (P value = 0.035) [6].
One meta-analysis including 3,111,714 patients observed that the proportion of infections between men and women is equal, however, men's risk of being admitted to the intensive care unit (ICU) due to the severity of disease was almost 3 times higher while the risk of a fatal outcome had an odds ratio (OR) of 1.38 compared to the group of infected women [7].
Different hypotheses have been proposed about this, some considering the influence of specific risk factors such as older age in the men group, multi-morbidities and tobacco index. However, the immunologic response differs between these two genders, with mediation by specific sex hormones such as testosterone and estrogens.
We know that testosterone has a suppressing role in the immune system, contrary to estrogens [8]. It has been demonstrated that SARS-CoV2 enters the cell through the mediation of the ACE2 and the cell protease receptor TMPRSS2 [2]. This TMPRSS2 receptor is also a biomarker in prostate cancer, and its expression is mediated by testosterone [9,10].
Sexual hormones then have a fundamental role in the immunologic responses, as estrogens are closely related to T-cell proliferation, the X chromosome is also related to genes that have an important role in the development of autoimmune diseases that are more common in women. Testosterone on the other hand, has a down-regulation effect in natural killer cells and TNF-α [11]. In the course of infection women have a better, more efficient and faster immunological response.
In clinical observations, it was found that patients with androgenic alopecia had a worse outcome that those that did not have alopecia, including women that had this same condition; this resulted in the description of Gabrin's sign, that consists in androgenic alopecia in COVID-19 patients, apparently associated with a worse prognosis that those who do not have it. This clinical sign gets its name from Dr. Frank Gabrin, who had androgenic alopecia and was the first physician from the United States to pass away from COVID-19; he was also a testicular cancer survivor.
In one study from Spain by Wambier, et al. 175 patients with COVID-19 severity criteria were studied, of which 122 were men and the rest were women. 67% had androgenic alopecia, 79% of men and 42% of women; said results support the previous hypothesis [12].
Similarly, the result of a cohort of 44 men with severe COVID-19 supported this same hypothesis, since androgenic alopecia was present in all of these patients. One important observation is the fact that prostate cancer patients that are being treated with testosterone blockers have shown a decreased risk of COVID-19, compared with cancer patients without the hormone-depriving treatment [13].
In an orchitis-like syndrome reported in men with COVID-19, a reduction in testosterone production was observed, reflecting directly in lower levels of this hormone and a worse outcome [14]. A lesser expression of ACE2 in men predisposes a higher risk of fatal pulmonary disease compared to women [15]. Observations by Soro-Paavonen, et al. support this theory, since they found that circulating levels of ACE2 are higher in men and patients with comorbidities like diabetes and cardiovascular disease [16].
Logic up until this moment pointed to lower levels of testosterone being present in those patients gravely affected by COVID-19, resulting in irregularities in expression ACE2 and TMPRSS2 receptors. Also affected are the endothelial cells, increasing production of reactive oxygen species, leading to cellular dysfunction through oxidative stress and inflammation. And thus, the cytokine theory proposes that low levels of testosterone in male COVID-19 patients of advanced age, predisposes a more severe cytokine storm, often requiring mechanical ventilation, increased pulmonary damage and catabolism of respiratory muscles [17].
Considering that men usually have 7 to 8 times more testosterone than women, it would be expected that this would not play an important role in the pathophysiology in the female gender, however, in a retrospective analysis done in the ICU at the Hamburg-Eppendorf University, among patients admitted between March 8th through April the 29th , it was found that testosterone levels have a specific effect by gender: Most men with elevated testosterone levels, had a lower expression of inflammatory cytokines such as VEGF, Il-2 and INF-y, all of which are involved in angiogenesis and cellular endothelial function. On the contrary, in women, levels of IL-6, GM-CSF, IL-12, IL-1B and IL-15 were elevated in those con lower levels of testosterone, and were consistent with 60% of patients admitted to the ICU for severe COVID-19 [18].
Testosterone could act as a protective factor, reducing the risk of cytokine storm, on the contrary, lower levels of testosterone have been associated with higher levels of IL-1 beta, IL-6 and TNF-alpha; this is why defining the role of this hormone in the infection of SARS-CoV2 and progression of COVID-19 could point to new forms of treatment and prevention.
Of note, is the proposal of hormonal substitution therapy as a helper in treatment, backed by studies such as that published by the Journal of Sexual Medicine, where it was found that despite having comorbidities, a group of men going through hormonal substitution therapy with testosterone had on average a smaller number of admittances to the ICU, even though this was not statistically significant [19].
The use of inhibitors of TMPRSS2, which are currently used in the treatment of prostate cancer, has also been proposed, since this molecule is also expressed in the lungs, as a means to treat pneumonia secondary to COVID-19 [20].
Finally, the knowledge of the role of androgens during the COVID-19 pandemic could offer treatment directed at this physiological route. There are also hypotheses, such as the one by Wambier, et al. were the phenotype of hyperandrogenism is related to an increase in viral dissemination and severity of COVID-19 [21]. On the contrary, Giagulli, et al. propose that men with lower testosterone are prone to develop worse systemic inflammation and a worse respiratory outcome [22]. Creating a debate about the real role of androgens in COVID-19, we could state that more investigation for therapeutic and diagnostic purposes is needed, which is why we decided to do this study in the population on Mexicali, with the intention of improving the management and prognosis of this disease.
This was an observational, prospective study, made in Hospital General de Mexicali (Mexicali's General Hospital, a government sponsored popular hospital).
Our study was made in the period between January 1st 2021 to April 30th of that same year. Data from patients admitted to the internal medicine service with a COVID-19 diagnosis was taken from the hospital's electronic health record. The inclusion criteria were: Patients over the age of 18, both men and women and an operational diagnosis of COVID-19 (Either a positive PCR test, or clinical diagnostic with a confirmatory chest tomography).
Relevant data such as age, biological sex, smoking status, disease comorbidities, (diabetes, hypertension, dyslipidemia, chronic kidney disease, thyroid disease) and previous medication, date of onset of COVID-19 symptoms, date of hospital admittance, tomography severity index and result of diagnostic COVID-19 tests such as PCR, chest CT scan, antigen or antibody test. Clinical data was taken from admittance records such as heart rate, respiratory rate, mean blood pressure, ventilatory status, and whether the patients had need of vasoactive amines (dopamine or norepinephrine). The risk of death was calculated with both the APACHE and SOFA scales both at admittance and at 48 hours. Relevant laboratory test data during the hospital stay was also included. Finally, we also looked at whether the patient developed ARDS (according to the 2018 Berlin definition) and the patient's condition at discharge or death. For this study, a blood sample was taken for each patient at admittance for measurement of free testosterone serum levels using an ELISA method.
The sample size was estimated according to an alpha error of 0.05, with an estimated power of 80, resulting in a minimum sample size of 49 patients.
For the statistical analysis the software Minitab version 18 was used. We determined the correlation between serum levels of free testosterone and both the SOFA and APACHE scores using a lineal regression and Pearson correlation methods. The difference between testosterone levels between men and women, as well as the difference in testosterone between survivors and non-survivors was made using the Student's T test. A statistically significant difference was considered when the P value was < 0.05. This work was approved by the Comité de Etica del Hospital General de Mexicali ethics committee.
49 patients met the inclusion criteria, of which 33 died representing 67% of our sample. 32 of the total 49 were male (65.4%), out of these 32 males, 21 did not survive. Out of the 17 women included (which represented 34.6% of the total sample) 11 died, representing close to 65% fatality rate on both the men and women subgroups.
The mean free testosterone for the survivor group was 3.21 pg/ml (SD ± 2.0) compared to a mean free testosterone of 1.82 pg/m in non-survivors (SD ± 1.46; p = 0.007).
The male gender had a mean free testosterone of 2.95 pg/ml (DE ± 1.77). Surviving males had a mean free testosterone of 3.95 pg/ml (SD ± 1.95). Non-surviving males had a mean free testosterone of 2.43 pg/ml (CI 95%; SD ± 1.46; p = 0.017). In the female subgroup, the mean free testosterone was 1.08 (SD ± 1.01), with female survivors having a mean free testosterone of 1.85 pg/ml (SD ± 1.37) and a mean of 0.66 pg/ml in the non-survivors (CI 95%, SD ± 0.41; p = 0.01).
Pearson's correlation was used to measure correlation between free testosterone levels and different patient characteristics, where a moderate and negative correlation was found between free testosterone levels and the score in the APACHE II score at admittance (r = -0.407 p = 0.015), as well as a weak and negative correlation between age and free testosterone levels (r = -0.288; p = 0.04). For the rest of the analyzed parameters, a negative, but statistically insignificant correlation was found (Table 1, Table 2 and Figure 1).
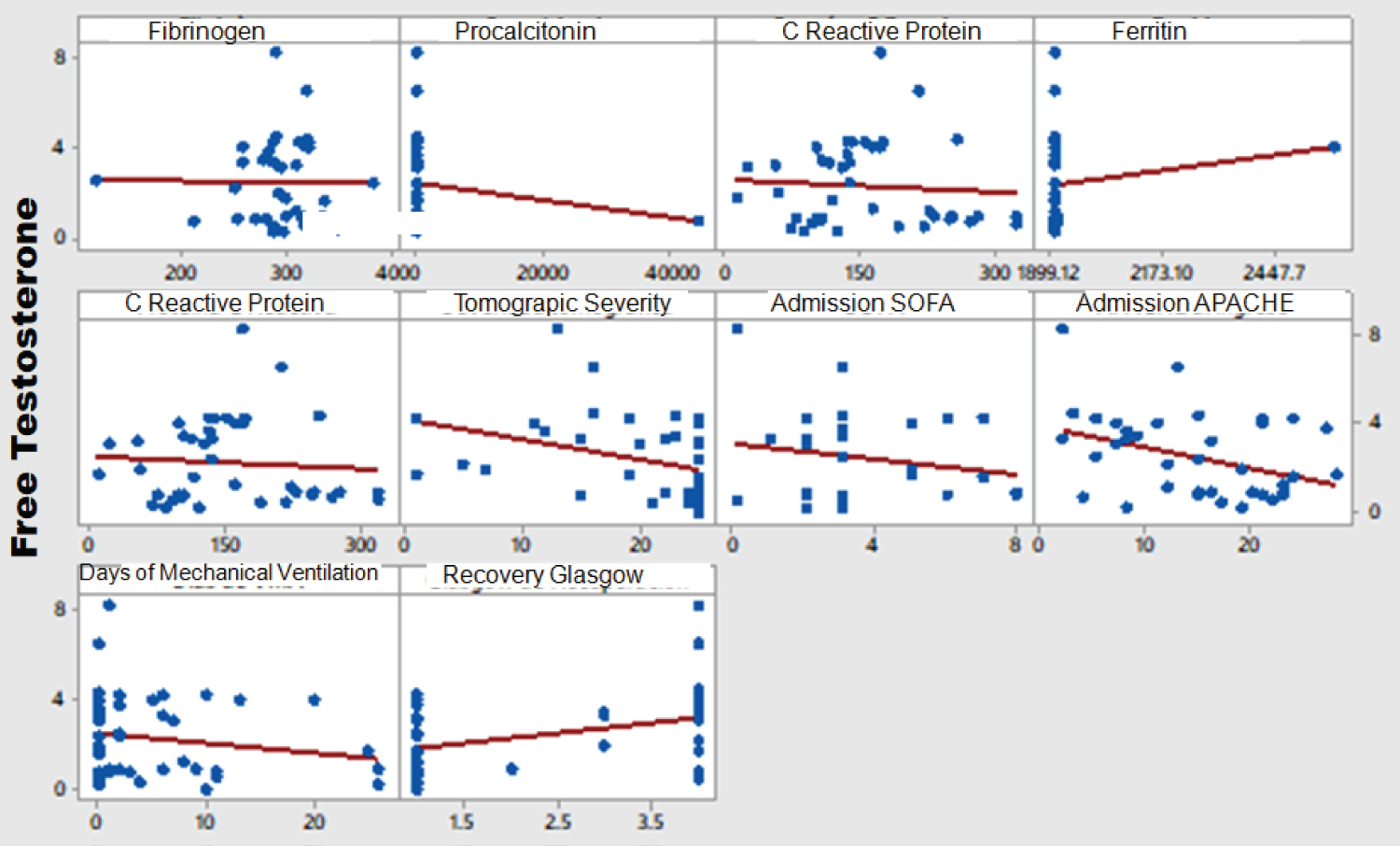 Figure 1: Free testosterone and severity markers correlation. View Figure 1
Figure 1: Free testosterone and severity markers correlation. View Figure 1
Table 1: Free testosterone means by gender and outcome. View Table 1
Table 2: Correlation between free testosterone and inflammatory biomarkers. View Table 2
A number of studies have found an association between the male gender and a worse prognosis in COVID-19, which has led researchers to find a possible association between sex hormones, SARS-CoV-2 and its receptors. Likewise, a correlation has been found between the androgen TMPRSS2 receptor and the SARS-CoV-2, similar to other virus such as the influenza virus [20]. This androgen receptor is found in different organs such as the prostate, testicles, and lung tissue; thus allowing the SARS-CoV-2 virus to more easily access these tissues, this being a possible explanation of why men tend to have worse outcomes in COVID-19.
Our study demonstrates that those patients hospitalized with COVID-19 pneumonia and lower levels of testosterone had a higher chance of worse outcomes and death, compared to those patients with higher free testosterone levels. This held true for both biological sexes.
Our findings are similar to those of Rastrelli, et al. who observed in a study involving 31 male patients hospitalized with pneumonia due to COVID-19 that a low testosterone level was a predictor for a worse outcome [11]. Unlike the previously mentioned study, out study includes both men and women; but like the work of Rastrelli, et al. the correlation between testosterone levels and inflammatory biomarkers was negative but not statistically significant. Similarly, Dhindsa, et al. published a study involving 152 patients with a PCR-confirmed diagnosis of COVID-19, including 143 hospitalized patients, of whom 90 were male. They took blood samples on admittance and during the following days, finding that surviving patients had almost 3 times as much serum testosterone than those who did not live, independent of other risk factors associated with COVID-19 severity, with a p value of p = 0.007 [21]. It's worth mentioning however, that this study did not find relevant data on testosterone levels and the female sex.
In Our study, a negative, statistically significant correlation was found between the levels of free testosterone, age and the APACHE II score; which contrasts with the findings of Salciccia, et al. who found no statistically significant correlation between testosterone levels and the age of the studied men [22].
The relationship between low levels of testosterone and an increase in all-cause mortality has been described previously, as explained by Araujo, et al. who analyzed 21 studies in men, concluding that lower levels of testosterone are correlated to an increase in all-cause mortality, as well as an increase in cardiovascular disease. However, the heterogeneity between the included studies was high [23].
One of the weaknesses of our study was not considering a possible association between obesity and testosterone levels, as this condition has been associated with hypogonadism, which is considered by some as a risk factor for severity and death in patients with COVID-19 [24,25]. Likewise, a meta-analysis by Aghlili, et al. supports the theory of obesity as a risk factor [26], which implies a weakness in our work, as only free serum testosterone was measured in the included patients, instead of also measuring total testosterone, FH and LH among other possible biomarkers.
It's important to note that our sample of patients includes only those who were hospitalized in the internal medicine service with COVID-19 pneumonia, meaning that only moderate to severe patients were studied. We can't negate the possibility that the testosterone levels in our sample are lower than that of the general population, as our sample was made up of mostly middle-aged to older hospitalized and gravely sick patients.
The authors declare that there were no conflicts of interest related to any aspect of our study. The studied blood samples were analyzed through "Laboratorio Lozano" a private laboratory, unrelated to the Hospital General de Mexicali. This private laboratory sponsored the measurement of free testosterone levels. No royalties or economic benefits existed for any of the involved researchers.