Background: PTB can mimic many chronic lung diseases resulting in misdiagnosis with serious consequences.
Objectives: To appraise all SN PTB patients who were referred to us from lower health facilities after unsuccessful treatment in order to confirm the appropriate diagnosis.
Methods: A cross sectional study at the pulmonary section of our hospital.
Results: The median age of our patients was 46 with interquartile range of 32 to 54 years. The commonest presenting symptom was difficulty in breathing which was present in almost 90% of them (30 out of 34), cough was present in 24 with sputum production in 22 while haemoptysis was reported in 3. All the 5 patients with malignancy reported chest pain. Sixty eight percent of the patients were referred from Peripheral TB DOT centers and sputum smear tests were done in 82% of them while radiologic tests were done in less than 50% of the patients. The final diagnoses include COPD, malignancy, sarcoidosis, interstitial lung diseases and fungal infection among others.
Conclusion: Many lung diseases are misdiagnosed as SN PTB because of similarity in clinical presentation, overreliance on diagnostic test with low TB detection and non adherence to local guidelines. We advocate for WHO-recommended rapid molecular test for all our suspected TB cases and prompt referral of difficult to diagnose cases.
International and national bodies have produced guidelines for diagnosis, treatment and control of the tuberculosis (TB) [1-5]. While the diagnosis of smear positive pulmonary TB (PTB) cases is more straight forward, that of smear negative (SN) PTB and extrapulmonary TB is usually more difficult due to low detection rate by smear microscopy, long time to culture-confirmation and variable sensitivity of molecular tests [6-10]. The diagnosis of SN PTB is greatly improved by Xpert MTB/RIF test [11].
PTB can mimic many chronic lung diseases resulting in misdiagnosis with serious consequences. It is important that all cases of TB are promptly and properly diagnosed so that treatment can be commenced early in order to prevent avoidable complications and deaths. On the other hand, wrongly treating a patient without TB as one can lead to delay in appropriate diagnosis, exposure of patients to needless anti TB drugs with risk of adverse effects [3,7,10]. This is why world health organization (WHO) advocated for increase bacteriological confirmation by scaling up the use of diagnostics such as rapid molecular tests as the initial tests for TB [1]. Unfortunately, many middle and low income countries still rely on smear microscopy with its low rate of TB detection [6-8].
In Nigeria, all TB suspects who are SN are to be referred by the field officers to the medical officer for further investigations and treatment [12]. Regrettably, patients are either not referred or when they are referred; they are not properly assessed and investigated before commencement of anti TB drugs.
The idea for this study was conceived because we observed delays in referral of SN PTB patients to us for further assessment. The objective of this study was to appraise all SN PTB patients referred from lower health facilities after unsuccessful treatment in order to confirm the appropriate diagnosis.
A cross sectional study of all patients who were referred to us after unsuccessful treatment for SN PTB.
Study was carried out at the pulmonary section of the Department of Medicine, University of Ilorin Teaching Hospital (UITH). The city of Ilorin is the capital of Kwara state which is one of the six states in North Central geopolitical zone of Nigeria. The University of Ilorin Teaching Hospital is a 600-bed tertiary hospital which serves as a major referral center for kwara state and other neighbouring states.
All consenting adult patients who were referred to us after initial unsuccessful treatment for SN PTB were recruited consecutively over a period of two years. They were all reviewed and appropriate tests were ordered to bacteriologically confirm or rule out pulmonary TB. All the patients tested negative to GenXpert MTB/RIF and sputum culture and hence were declared as not having PTB. They were further investigated based on their clinical features and the final diagnoses are presented under results.
A questionnaire was designed to obtain the following information from the participants: age, sex, complaints duration, duration of treatment at referral center before presenting to us, laboratory and radiologic tests done at referral facilities and final diagnosis after our assessment.
We did not do any form of intervention in the patients. All investigations and treatment given to participants were based on the nature of their illness. However, their consent was obtained before data inclusion in the study.
Data was analyzed using SPSS version 20. Age and duration of treatment before patients were referred to us were presented as median with interquartile range while other variables were summarized as frequencies.
We received a total of 34 patients who were initially diagnosed and treated for SN PTB at the referral health care facilities over a period of two years. The patients were referred to us because they either did not improve or continued to deteriorate while on treatment for TB. The presenting symptoms are as shown on Table 1. Twenty of them were males and their median age was 46 with interquartile range of 32 to 54 years. The commonest presenting symptom was difficulty in breathing which was present in 30 of them. All the 5 patients with malignancy (mesothelioma and lung cancer) reported chest pain.
Table1: Presenting symptoms in the 34 patients. View Table 1
The bulk (23; 68%) of the patients were referred from Peripheral TB DOT centers and sputum smear tests were done in most (28; 82%) of them while radiologic tests were done in less than 50% of the patients (Table 2).
Table 2: Showing referral heath facilities and tests done before referring patients to us. View Table 2
As shown on Table 3, the final diagnoses in the patients are chronic obstructive pulmonary disease (COPD) in seven of them, sarcoidosis in six, idiopathic interstitial lung disease in six, lung cancer in four, fungal infection in four and four cases of connective tissue disease associated lung disease. Sickle cell related lung disease and pleural mesothelioma were diagnosed in two patients.
Table 3: Final diagnosis in the 34 patients. View Table 3
The median duration of treatment before referring to us was 2 months with interquartile range of 3 weeks to 4 months.
MJ was a 38 year old teacher who was referred to us with difficulty in breathing, weight loss of 10 months and abdominal swelling of 3 months. There was no cough, fever or nocturnal sudation. He had poorly localized abdominal discomfort. There was no jaundice and no hiccup. There was no occupational exposure. At the onset of the illness he presented to the medicine department of a Federal medical center where he was investigated and was diagnosed as left pleural effusion secondary to SN PTB. Serial sputum and pleural fluid GenXpert MTB/RIF were negative. He had chest tube inserted and was commenced on anti TB drugs at the referral hospital. However, he was referred to us for further evaluation after 3 months because his condition continued to deteriorate.
Examination revealed a chronically ill looking man who was not pale; there was no fever (temperature was 36 oC). He had left axillary lymph node which was about 2 × 2 × 2 cm and bilateral pitting pedal oedema, SPO2 was 96% on room air.
Respiratory system: The rate was 32 breaths per minute and had a chest tube inserted on the left hemithorax. There was reduced chest expansion and reduced tactile fremitus with dull percussion note over the left lung. Breath sound and vocal resonance were also absent. The right lung was clinically alright.
Abdomen was uniformly distended, moves with respiration and there was vague generalized tenderness. There was no organomegaly. Ascites was demonstrable by shifting dullness. The bowel sound and rectal examination were normal.
The other systems were normal.
He came with chest computer tomography (CT) scan (Figure 1) from the referral hospital. It showed thickened pleural lining of the left hemithorax, containing air-fluid level. Chest tube was noted in situ, with tip within the cavity and complete collapse of the left lung towards the hilum. Small nodules were reportedly seen diffusely in the right lung field. Multiple areas suggestive of bone metastases were reported in the mid portion of the sternum and the vertebral ends of the 7th and 12th ribs on the left.
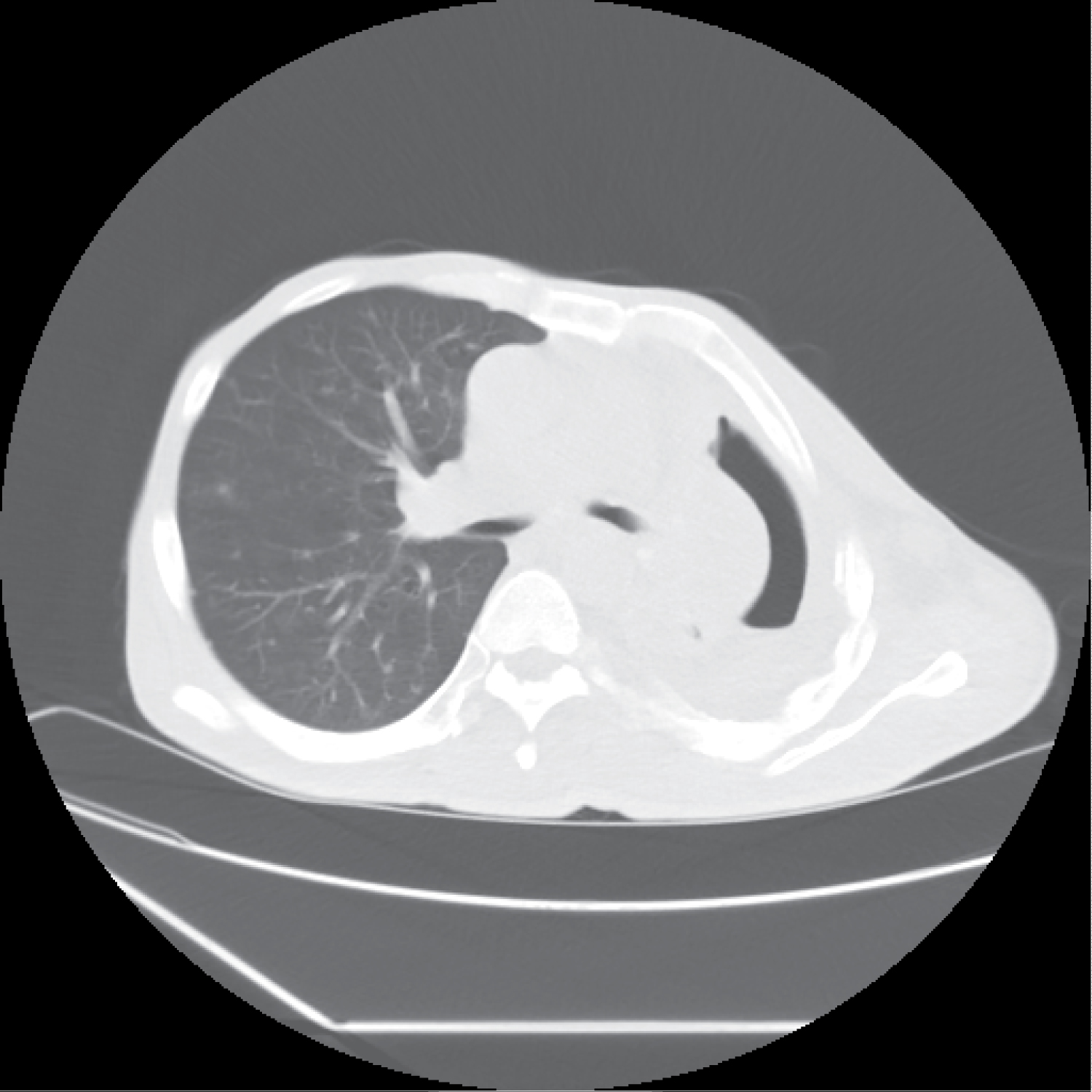 Figure 1: Pleural thickening of the left hemithorax, complete collapse of the left lung to the hilum with destruction of the vertebral ends of the rib on the left.
View Figure 1
Figure 1: Pleural thickening of the left hemithorax, complete collapse of the left lung to the hilum with destruction of the vertebral ends of the rib on the left.
View Figure 1
The cardiothoracic unit was invited to review him. He had video assisted thoracoscopic surgery with pleural sampling which came out to confirm pleural mesothelioma (epitheloid variant). The left axillary lymph node also revealed spread of the malignancy to it. Alas, the patient succumbed to the illness two days after diagnosis was confirmed.
OT was a 37 year old man referred with breathless of 7 months duration as well as cough with yellow sputum, fatigue and fever of 2 weeks. He had been working as an estate surveyor for the last 5 years and had occasional dust exposure. Smoked 17 pack years from age 19 until 3 weeks prior to presentation. He also smoked cannabis everyday from the age of 20 till 30 and then occasionally till 2 months before presentation. There were no skin changes, claudication, dysphagia, joint pains, mouth dryness or any eye symptoms. He presented at a general hospital where he was diagnosed and treated for SN PTB but was referred to us as a case of anti TB treatment failure when he did not improve.
Examination revealed that he was dyspnoeic at rest, had low fever (temperature was 37.9 oC). His SPO2 was 92% on room air and it rose to 96% on 3L/minute of 100% supplemental oxygen via nasal prong.
Respiratory system examination revealed tachypnoea with respiratory rate of 32/minute. He had few crackles on the left lung base.
Other systemic examination was normal except for tachycardia.
Pulmonary sarcoidosis was suspected based on chest CT (Figure 2), elevated angiotensin converting enzyme (178.98 U/L) and elevated serum calcium (2.62 mmol/L). Repeated sputum GenXpert MTB/RIF were negative for tuberculosis. Serology for auto-antibodies was normal. Sputum culture grew pseudomonas aeruginosa but negative for fungi and TB. Most of his symptoms improved after treatment with oral levofloxacin for 3 weeks but dyspnoea continued. A bronchoscopic biopsy showed non-specific inflammation. He however requested to be referred to Dubai. A CT guided lung biopsy of the left upper lobe consolidation (Figure 3) which was done in Dubai showed granulomatous inflammation without any caseation hence the diagnosis of pulmonary sarcoidosis was upheld. He was continued on the treatment started by us with great improvement. He is currently being followed up on treatment in our hospital.
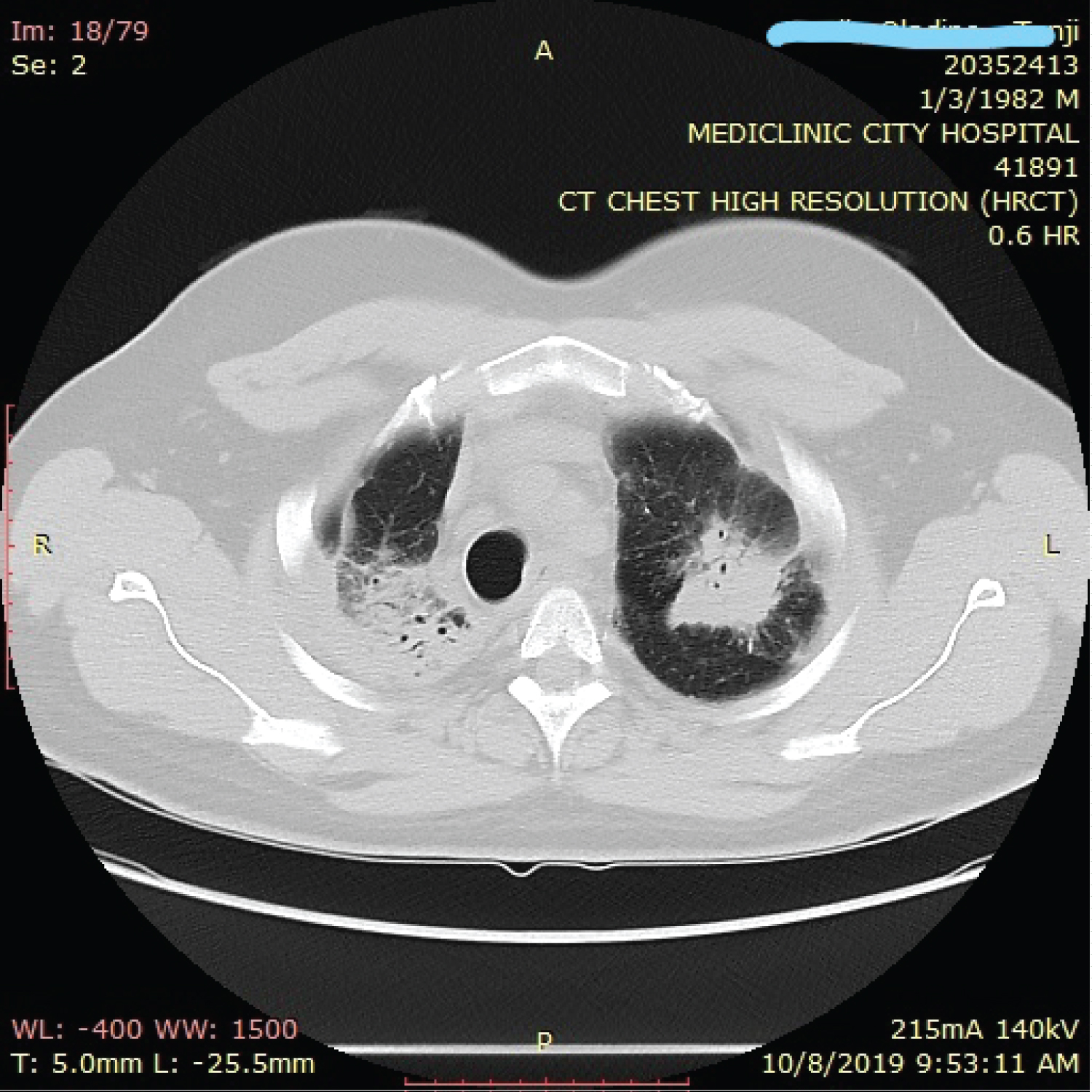 Figure 2: Multifocal segmental consolidation and air bronchogram in both upper lobes.
View Figure 2
Figure 2: Multifocal segmental consolidation and air bronchogram in both upper lobes.
View Figure 2
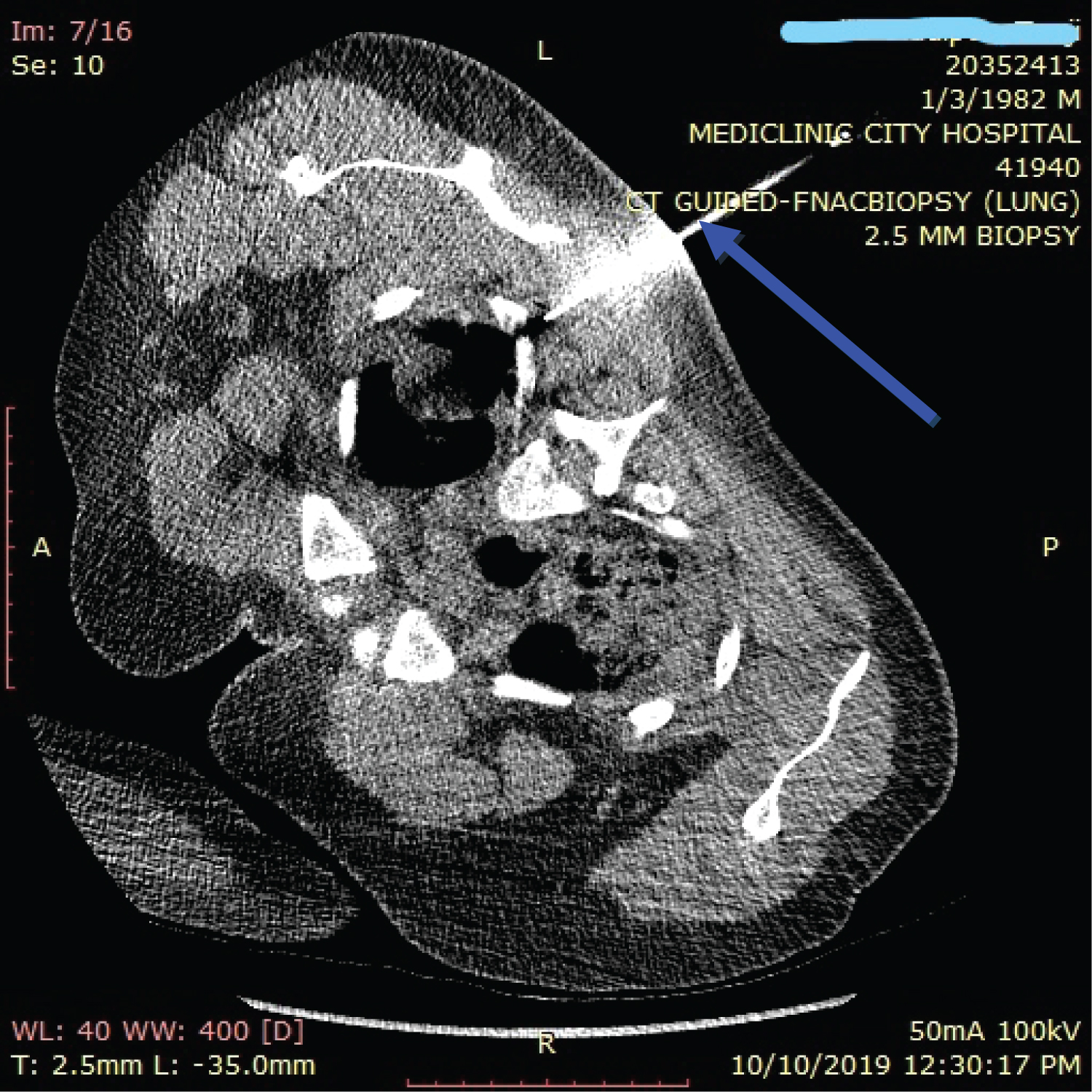 Figure 3: Computerized tomography guided needle (blue arrow) lung biopsy of the left upper lobe consolidation.
View Figure 3
Figure 3: Computerized tomography guided needle (blue arrow) lung biopsy of the left upper lobe consolidation.
View Figure 3
TD was a 50 year old man referred with cough of 2 months which was initially productive of yellowish sputum but turned to frank blood 2 days before presenting to hospital. Each episode of blood was about 20 mls, occasionally with clots but there was neither postural dizziness nor fainting attacks. He also complained of painful swelling of right breast of about 1 month. There was no family history of breast cancer. There was no fever, no weight loss, no chest pain but he had mild dyspnoea on moderate exertion. There was no smoking or occupational exposure and no contact with individual having chronic cough. He had no symptoms suggestive of a connective tissue disorder.
He was recently diagnosed with diabetes mellitus in the course of the current illness but was diagnosed hypertensive about 5 years earlier. He was commenced on metformin and glimepiride for diabetes and lisinopril for hypertension at the referral hospital. He was also managed as a case SN PTB with anti TB drugs which was commenced about 2 weeks earlier but was referred to us when he started coughing blood.
His general and systemic examinations were unremarkable except for a blood pressure of 150/100 mmHg and a tender swelling in the right breast. He had no peripheral lymphadenopathy.
He was admitted as a case of moderate haemoptysis likely due to chest infection or metastatic malignancy in a diabetic hypertensive patient. His sputum Xpert MTB/RIF assay did not detect MTB. Serology for auto-antibodies was negative. His erythrocyte sedimentation rate was 52 mm/hour (range 0-20) and haemoglobin of 11.5 g/dl. His HIV screening was negative. He did a chest CT (Figure 4) which shows ground glass opacity with perivascular consolidation in the right upper lobe. The CT also showed an irregular right breast soft tissue swelling.
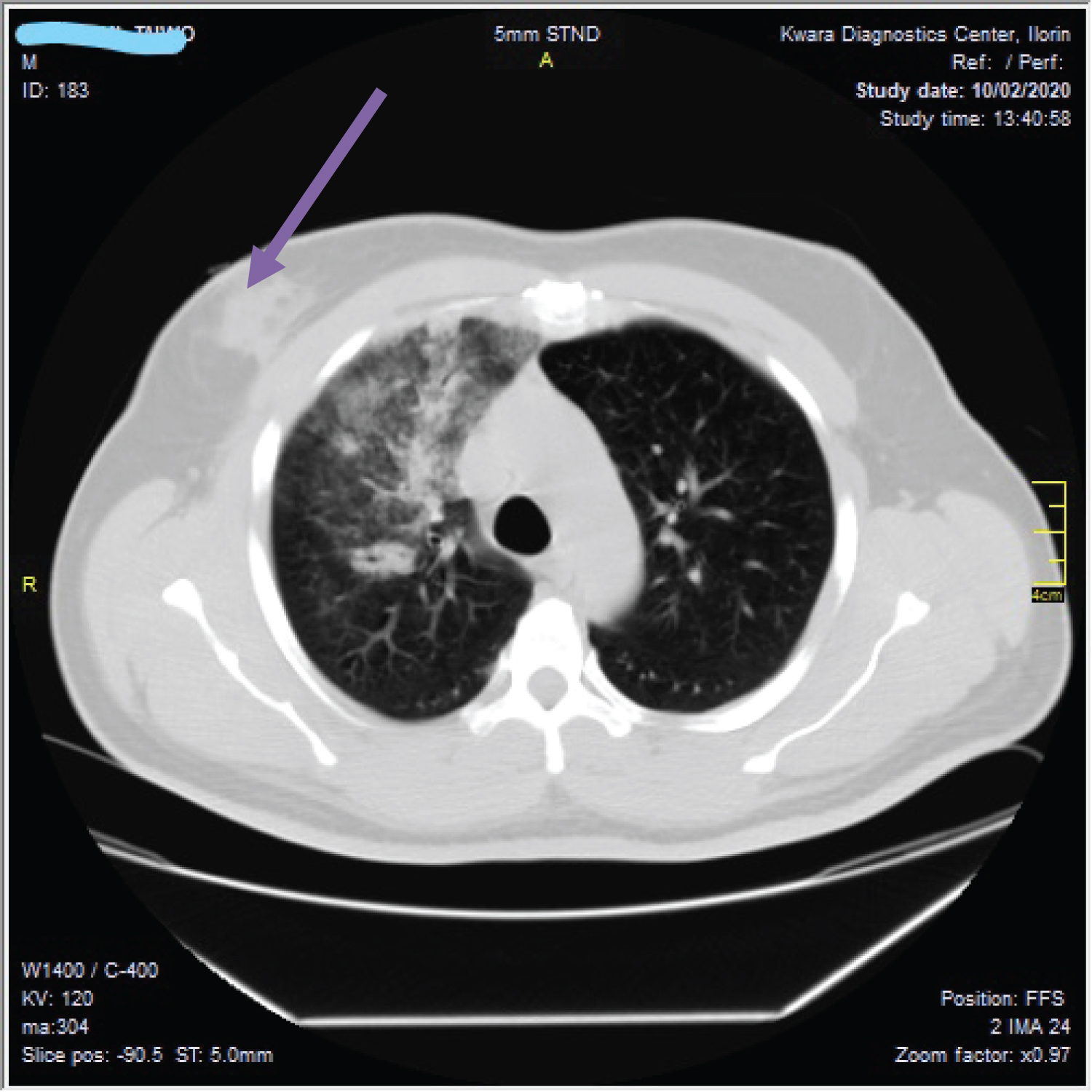 Figure 4: Ground glass opacity with perivascular consolidation in the right upper lobe and an irregular (purple arrow) soft tissue swelling in the right breast.
View Figure 4
Figure 4: Ground glass opacity with perivascular consolidation in the right upper lobe and an irregular (purple arrow) soft tissue swelling in the right breast.
View Figure 4
Fine needle aspiration of the breast swelling was negative for malignancy. Result of fungal studies showed that Candida species was cultured from the sputum.
His haemoptysis stopped within few days of oral tranexamic acid though was still coughing. The cough improved and later stopped with use of capsule Itraconazole. The painful breast swelling also completely resolved with the antifungal treatment and the patient has remained clinically stable on follow up at our outpatient clinic for his diabetes and hypertension.
TB can mimic many diseases and it is important to make correct diagnosis promptly so as to commence appropriate treatment. Misdiagnosis of conditions mimicking PTB is compounded by negative sputum smear in some cases of PTB. Smear microscopy, with its limitation is still done in many middle and low income countries [6-8,13]. This is aggravated by poor supplementary imaging and laboratory data to support an empiric diagnosis. SN PTB is a recognized clinical entity and our national guidelines recommend that the patient should be referred for further evaluation [12]. Frequently, these patients are either not referred or they are not properly assessed before commencement of anti TB drugs. Oshi, et al. also reported sub-optimal adherence to the recommendations of our national TB guidelines by health care workers [14].
Our first illustrative case assessed by an internist who treated him as SN PTB based on negative sputum and pleural fluid GenXpert MTB/RIF tests. This is even more serious because the patient was sent for a chest CT which reported a left side pleural thickening with fluid collection and other features suggesting mesothelioma with metastasis to the right lung, sternum and the vertebral ends of the 7th and 12th ribs on the left. Yet the patient was sustained on anti TB drugs and was only referred when his condition continued to deteriorate despite anti TB drugs. In all, five of our cases who were initially misdiagnosed as PTB actually had malignancy. Several previous studies have documented cases of lung cancers misdiagnosed as SN PTB [15-18]. These cases should have been promptly referred for further expert assessment.
One of the seven COPD cases almost completed six months of anti TB at a peripheral center. He was referred as a case of TB treatment failure but further evaluation revealed that it was a COPD case which responded promptly to treatment. There are reported cases of misdiagnosis of COPD and endobronchial asthma as SN PTB [19,20]. Prompt referral by peripheral centers to specialist centers with appropriate equipment is mandatory.
Sarcoidosis was another condition misdiagnosed as PTB in six patients. The clinicoradiological features of sarcoidosis are similar to TB, thus posing a great challenge in countries endemic for TB [21,22]. Pulmonary sarcoidosis, is often misdiagnosed as SN PTB. However, misdiagnosis of the 2 conditions should be avoided because their treatments are definitely different [23]. Misdiagnosis of sarcoidosis as TB can lead to delay in appropriate diagnosis, unwarranted use of anti TB drugs with adverse effects, preventable complications and deaths. Conversely, reactivation of tuberculosis after corticosteroid treatment for sarcoidosis is an important concern, especially in environment with high prevalence of latent tuberculosis infection such as ours.
Owing to similar clinical and radiological characteristics fungal infections may be easily misdiagnosed as tuberculosis especially among immunodeficient individuals. The extensive use of antibiotics and steroids has also recently caused a widespread prevalence of fungal pulmonary infection. In many cases, missed fungal pulmonary infection may results in high rate of morbidity and mortality [24]. Oladele, et al. reported chronic pulmonary aspergillosis rather than TB as the cause of disease in 19% of smear and GeneXpert negative, HIV negative Nigerians [25].
All our patients were referred late because they were labeled and treated as SN PTB without following the recommendation of our national guidelines for prompt referral to higher centers [12]. The case managed at the Federal Medical Center should have been referred for further assessment without delay immediately after the chest CT report was received by the internist rather than waiting for three months to see if patient will respond to anti TB drugs. WHO has advised against "therapeutic trial" in TB since 2003 [26]. Furthermore, SN PTB is a recognized clinical entity as defined by guidelines and not a "misdiagnosis waste basket" where complex and confounding cases that should be referred for further expert opinion can be "dumped" while awaiting possible response to unwarranted anti TB drugs.
The results of our study should be interpreted cautiously because it involved relatively few patients who were referred to our center. Despite the limitations of being a single-center study with small sample size, our findings have shown that not all patients diagnosed as SN PTB had TB and that health care providers at various levels have not been properly following our national guidelines on treatment of SN PTB. Hopefully, this report will stimulate larger multicenter work.
Our study has revealed that serious illnesses like lung malignancy are sometimes misdiagnosed and treated as SNPTB in our lower heath facilities thereby delaying opportunities for prompt correct diagnosis and treatment. The misdiagnosis was due to similarity in clinical presentation, overreliance on diagnostic test with low rate of TB detection and lack of adherence to local guidelines among others. We advocate for urgent scale up of the WHO-recommended rapid molecular tests such as GenXpert MTB/RIF as the initial test for evaluation of all our suspected TB cases as well as prompt referral to higher centers (with pulmonologist) of suspected cases who cannot be bacteriologically confirmed at lower centers. We also advocate for a review of our national guidelines on TB treatment and control which was last updated in 2010 (over a decade ago).
Key message of this work: Our work emphasizes the fact TB mimics should not be misdiagnosed as smear negative PTB (SN PTB) because of the consequences as shown in our patients. It highlights the need for health care providers, particularly in TB high-burden and low income countries, to promptly investigate all cases of SN PTB in order to prevent complications and death.