The aim of this study was to analyze the effects of different resistance exercise orders on training intensity in middle-aged and older women. Twenty-three participants (age 50-78 years) were randomized into two RT groups: One group started training sessions performing multi-joint exercises followed by single-joint exercises (MS, n = 12; 58.92 ± 5.53 years), while the other group performed their session in the opposite order (SM, n = 11; 57.93 ± 11.89 years). Both groups completed RT sessions twice a week for 16 weeks using 7 exercises performed in 3 sets of 10-15 repetitions maximum, in the morning hours. Total training load was registered for all exercises session by session during the entire intervention period. Both training groups significantly increased training intensity after the intervention regardless of the exercise order employed with no significant deference between order.
Aging, Exercise prescription, Elderly
Among the many modes of physical exercise employed by older adults, resistance training (RT) has been widely utilized due to its potential to increase fat-free mass [1], enhance muscular strength [2-5], reduce body fat [6,7], decrease blood pressure [8], and promote positive changes in lipid profile [9] and functional capacity [10]. Any one or combinations of these changes are likely to enhance total well-being [11] and improve quality of life [12] in this population.
Therefore, researchers have invested a considerable amount of time analyzing the benefits of RT programs in older adults, especially by manipulating program variables. Factors such as weekly training frequency [4,13,14], number of sets and repetitions [5,7,15], rest interval [16], training system [2], and speed of movement [17] have been explored. The magnitudes of adaptations provided by a RT program are usually dependent on the proper manipulation of these training variables [12,18].
Although not specifically a training variable, exercise order (EO) is a structural variable [18] that has been explored in order to analyze the possible effects of different EO on training outcomes. Studies have focused on the effects of EO on blood pressure [19-21], muscular strength and hypertrophy [10,22-24], body composition [24,25], functional capacity [24], strength performance [23], and anabolic hormones [22], as well as cardiovascular disease risk factors [26]. The majority of these studies have shown no difference in the effect of EO on these parameters, indicating that the benefits derived from a RT program are not influenced by EO manipulation.
However, none of the previous investigations focused on analyzing the effects of EO on training intensity. Considering that RT at a higher-intensity may produce more significant improvements in muscular strength and functional fitness when compared to moderate-intensity protocols in older adults [27], it seems crucial to verify whether EO may interfere with training intensity during a RT program in older women. Jesus and colleagues [23], for example, showed that different EO employed in a training session might affect the number of repetitions performed in older women. This suggests that when an exercise is performed at the end of the training session, regardless of the size of the muscle group involved, there might be a significant reduction in the number of repetitions performed [23] and hence lower the total workload. Another study involving older women revealed that starting an exercise sequence with multi-joint exercises and proceeding to single-joint exercises did not appear to affect performance in the later exercises; however, the reverse sequence (single-joint to multi-joint exercises) produced a reduction in the total number of repetitions [28].
Currently, there is a lack of studies that have focused attention on the effects of different EO on RT program intensity. Although it was a secondary outcome, only one investigation has shown that the volume-load [load × sets × repetitions] was not different between different EO in older women [24]. Therefore, the aim of the current study was to analyze the effects of different resistance EO on training intensity in middle-aged and older women. We hypothesized that different EO would not affect training intensity differently.
Participants were recruited via newspaper notification, radio advertisements, and home delivery of flyers throughout the central city and residential neighborhoods. Initially, 41 women volunteered to participate in this study. All interested participants initially completed a detailed health history and physical activity questionnaires. Those who were admitted to the study were required to meet the following inclusion criteria: Non-hypertensive (systolic blood pressure < 140 mmHg and diastolic blood pressure < 90 mmHg), non-diabetic, free from any cardiac or renal dysfunction, non-smokers, not receiving hormonal replacement therapy, not performing any physical exercise more than once a week during the preceding 6 months. After individual interviews, 9 volunteers were excluded because they did not meet all inclusion criteria. The 32 participants included in the study then performed a diagnostic, graded exercise stress test with a 12-lead electrocardiogram reviewed by a cardiologist. They were cleared for participation in the study with no restrictions. Written informed consent was obtained from all participants after being provided with a detailed description of investigation procedures, benefits, and possible risks. This investigation was conducted according to the Declaration of Helsinki and approved by the local University Ethics Committee (Process 2.754.821).
The 32 women were randomly assigned to one of two groups: One group performing RT from multi-joint to single-joint exercises (MS, n = 16) while the other group performing RT from single-joint to multi-joint exercises (SM, n = 16). Both groups performed 3 sets of 10-15 repetitions in 7 whole-body exercises twice a week for 16 weeks in a specific EO. Throughout the intervention period, 9 participants dropped out of the study due to surgery, injury, personal reasons, or loss of interest. Therefore, 23 women completed the study (MS = 12, SM = 11). Figure 1 presents the schematic design of participant recruitment and allocation.
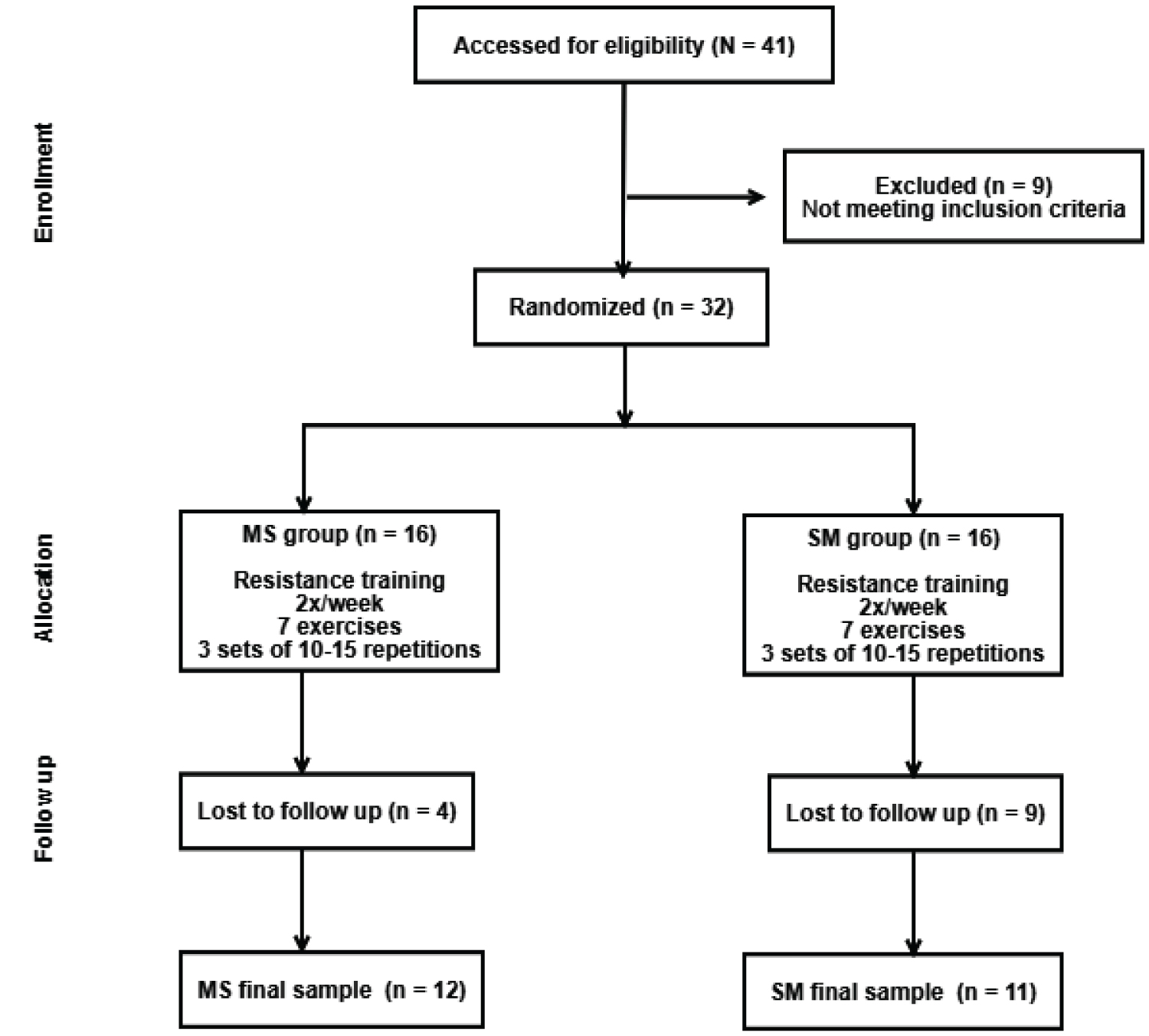 Figure 1: Experimental design (flowchart).
Figure 1: Experimental design (flowchart).
Note: MS = group that performed RT from multi- to single-joint exercises; SM = group that performed RT from single- to multi-joint exercises
View Figure 1
Body mass was measured to the nearest 0.1 kg using a calibrated electronic scale (Omron, Model HBF-214, Illinois, USA), with the participants wearing light workout clothing and no shoes. Height was measured to the nearest 0.1 cm with a stadiometer attached to the wall (E120A-Tonelli), with participants standing with no shoes. Body mass index (BMI) was calculated as body mass (kg) divided by height (m 2 ).
Both training groups performed the same program differing only in EO (Table 1). The RT program was composed of 7 exercises with 3 sets of 10-15 repetition maximum for each exercise. Participants were instructed to inhale during the eccentric muscle action and exhale during the concentric muscle action, while maintaining a constant movement velocity at a ratio of 1:2 for concentric and eccentric phases, respectively. Rest intervals between sets and exercises were 2-min and 3-min, respectively. Instructors adjusted loads of each exercise according to the participant’s ability and improvements in exercise capacity throughout the study to ensure performance with as much resistance as possible while maintaining proper execution technique.
Table 1: Resistance exercise sequence performed during 16 weeks according to the different EO. View Table 1
Instructors personally supervised all participants during the entire intervention to insure training intensity in each exercise. Instructors recorded the load (kg) applied in each exercise during each training session to insure the highest training load possible. Total training load for each participant was calculated as the product of the highest resistance lifted (in kg) by the repetitions completed in each exercise during the two training sessions performed each week.
Normality was checked by the Shapiro-Wilk’s test. Data were expressed as means and standard deviations. Baseline differences between groups were explored with an independent t-test, with Levene’s test used to analyze homogeneity of variances. Two-way analysis of variance (ANOVA) for repeated measures was used for within-group comparisons. In variables where sphericity was violated as indicated by Mauchly´s test, analyses were adjusted using a Greenhouse-Geisser correction. When the F-ratio was significant, Bonferroni’s post hoc test was employed to identify mean differences. For all statistical analyses, significance was accepted at p < 0.05. Data were stored and analysed using JAMOVI software, version 2.3.28.
There were no differences in age and anthropometric variables between groups at pre-training (Table 2).
Table 2: General characteristics of the groups pre-training. View Table 2
Figure 2 presents the total training load, in kg, for both training groups. In all exercises, total training load significantly increased in every 4-week block, except between weeks 9-12 and weeks 12-16, in which total training load did not increase for any of the exercises or groups (p > 0.05). All the total training load increments were similar between the different EO.
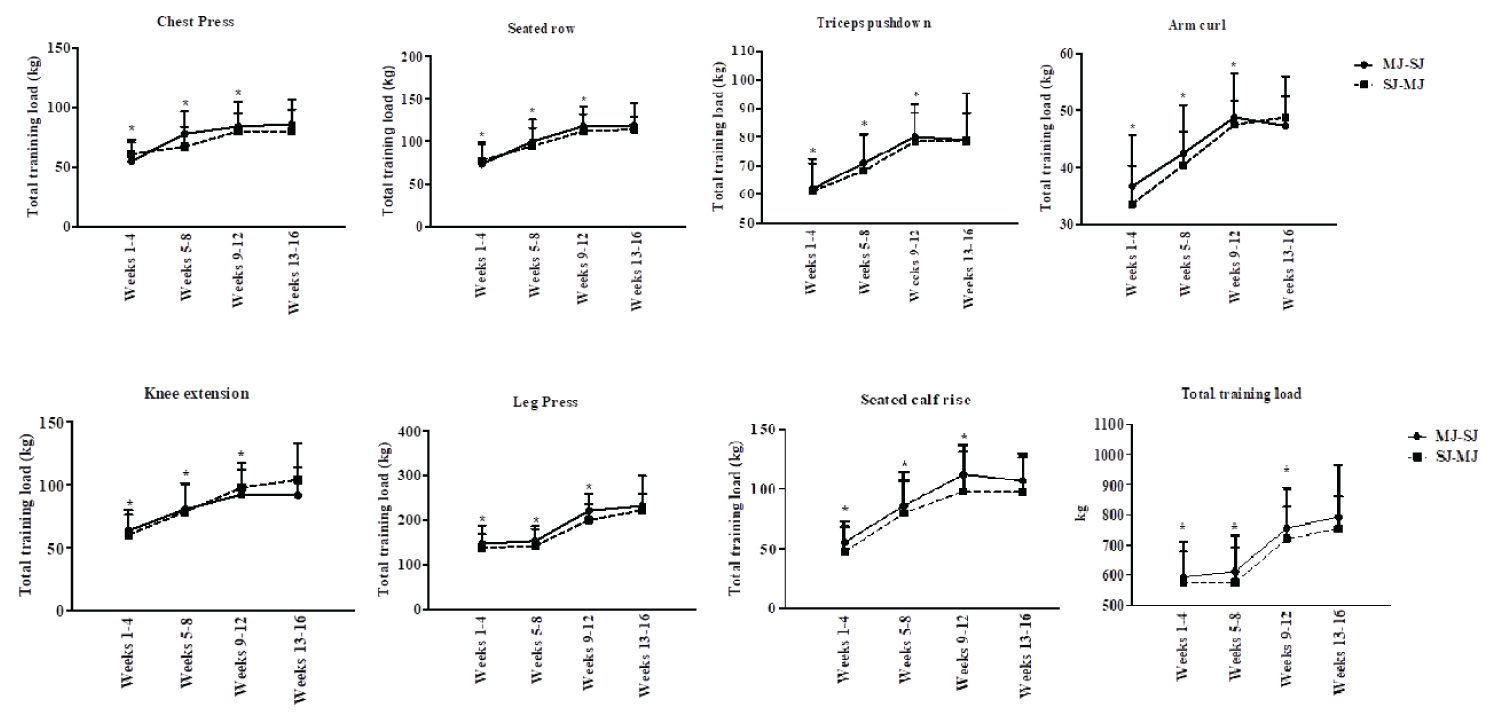 Figure 2: Total training load for the training groups for each of the resistance exercises performed, and total training load, in kg.
Figure 2: Total training load for the training groups for each of the resistance exercises performed, and total training load, in kg.
MS = group that performed RT from multi- to single-joint exercises; SM = group that performed RT from single- to multi-joint exercises. Data are presented as mean and standard deviation.
View Figure 2
The current study sought to determine the effect of different resistance EO on training intensity in middle-aged and older women. The results showed significant increases in training intensity throughout the entire intervention, except after the 12 th week of training where intensity seemed to have reached a plateau. Despite this plateauing in intensity, there was no significant difference in training intensity between the two EO, which confirms our original hypothesis that EO does not systematically alter the workload and subsequently improvements in function.
A recent study also showed that different EO produced similar increases in volume-load employed during training [24]. The older women in that study were submitted to 12 weeks of a RT program performed in 3 different EO (MS, SM, and alternating between upper and lower body order). Volume-load was calculated by multiplying load by sets by repetitions for each of the eight exercises and then summing the total load week by week. The major difference between the previous study [24] and the current investigation was the training loads in the current study were analyzed in isolation, without possible interference of the other training variables (i.e., sets or repetitions). In addition, our participants were novice to resistance exercises, while participants in the other study were resistance-trained older women.
Nunes and colleagues [29] submitted resistance-trained older women to four different EO in order to analyze the impact of EO on the load lifted. They observed no difference in training intensity among the different EO employed. Although the current investigation analyzed acute effects of EO on the load lifted, it is reasonable to assume that in a chronic perspective, the results would be similar. To the contrary, Tomeleri and colleagues [22] found that older women submitted to a RT program 3 times per week for 12 weeks with different EO produced higher volume-load (load × sets × repetitions) for the MS group than for the group that performed the SJ order. This was especially true when performing the chest press, leg press, and knee extension exercises. Since the RT protocols in their study were very similar to those in the current study (i.e., number of repetitions and exercises), a plausible explanation for the difference in results might be related to the possible influence of EO on volume-intensity training parameters [23,24]. Jesus and colleagues [23] submitted 12 resistance-trained older women to two different EO in an acute protocol and observed that the EO influenced the number of repetitions performed. This showed that when an exercise is performed at the end of the session, regardless of the size of the muscle group involved, the number of repetitions is reduced.
Overall, RT programs have been shown to confer several positive effects on health-related parameters, well-being, and quality of life, especially in older adults [6,22,24]. Thus, studies such as the current one are strongly recommended in order to provide more effective RT program prescriptions for older women. Nonetheless, some limitations of the current study need to be addressed. This study was composed of older women, which does not allow extrapolation of results to older men. In addition, only two EO were employed in the current study, which might limit extrapolation to other EO.
In contrast, we need to highlight the strengths of our study. The RT programs performed by participants were personally supervised throughout the entire investigation, which promoted homogeneity of training status and loads employed during training sessions. This served to guarantee the same training intensity for each EO group. To our knowledge, this is the first study that monitored training intensity by registering all training loads employed for all exercises performed during the 16 weeks of training. Finally, the RT program employed in this study was a whole-body exercise protocol involving upper and lower body exercises.
In conclusion, results of the current study indicate that both training groups significantly increased training intensity throughout the intervention regardless of the EO employed. These findings are clinically relevant for strength and conditioning professionals, as well as for gerontologists and personal trainers, who work with aging women performing physical exercise. It indicates that it may be left to the discretion of the practitioner to utilize the loading sequence that is most comfortable to them.
We would like to thank the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001; the Fundação de Apoio à UNESPAR for the financial support provided to this study, and all the participants for their engagement in the investigation.