Utilization of diverse anti-acid materials is necessary for the preparation of compound omeprazole capsules. However, to gain the satisfied anti-acid effect, use of large amount of anti-acids is always difficult to swallow. This study aimed to develop a lightweight compound omeprazole capsule which could achieve immediately drug releasing with high anti-acid ability in stomach.
Omeprazole was encapsulated in β-cyclodextrin to improve the drug solubility and stability. The influence of different factors on the efficiency of the drug encapsulation was investigated. In addition, the omeprazole inclusions were assessed by Fourier transform-infrared spectroscopy, differential scanning calorimeter, and X-ray diffraction. Finally, anti-acids materials such as magnesium oxide (MgO) and sodium bicarbonate (NaHCO3) were used to reduce the weight of the capsule contents.
Compared to the market omeprazole capsule (ENCHENG®), the omeprazole compound capsule demonstrated significantly improved drug dissolution (the maximum release ratio was 95.42 ± 2.51%) in simulated gastric environment. Moreover, rabbit pharmacokinetics showed that the area under the plasma concentration-time curve (AUC0-t) was significantly increased to 54180.11 ± 6483.16 min•ng•mL-1 (p < 0.05), compared with that (39011.55 ± 6637.08 min•ng•mL-1) of the currently used capsules (ENCHENG®).
The light compound omeprazole capsule could be an effective and swallowable oral delivering system for Acid-Related Disorders.
Omeprazole, β-cyclodextrin encapsulation, Drug delivery
Acid-related disorders (ARDs) are defined as a category of gastrointestinal disorders that are closely related to the effects of acid attacks [1]. ARDs mainly include peptic ulcer diseases (PUD), gastroesophageal reflux disease (GORD) and functional dyspepsia (FD) [2-3]. In recent years, the incidence rate has gradually increased about 5 times in western countries [4]. In general, changes in lifestyle such as weight loss [5-7], elevation of the head [8], abdominal breathing [9], and smoking cessation [10], can relieve acid-related symptoms. Medications including proton pump inhibitors (PPIs) [11] and H2 receptor antagonists [12] can also help. Studies have shown that PPIs have better effects than H2 receptor antagonists in the relief of Acid-related symptoms and are the first choice for the treatment of most ARDs [13-15].
Currently, omeprazole (OMZ) is a representative drug of the first generation of PPIs. It inhibits the proton pump in the gastric parietal membrane and prevents H+ in the cell wall from being transported into the gastric juice, thereby inhibiting the secretion of gastric juice. It is widely used for the treatment of gastric and duodenal diseases [16,17], and it also has a good therapeutic effect on most ARDs [11]. OMZ is very poorly soluble [18], but it has high permeability and is highly absorbable (> 90%) in the intestinal tract. It belongs to the biopharmaceutics classification system (BCS) class II [19] and the dissolution rate is a key factor for that ensures a better release. Therefore, increasing the solubility can effectively improve the release behavior of OMZ. Cyclodextrin (CD) is a water-soluble cyclic oligosaccharide obtained by hydrolysis of starch [20]. It has a hydrophobic cavity and a hydrophilic outer surface. It can form inclusion complexes with hydrophobic drug molecules to increase solubility and stability [21-23]. CD has been extensively studied due to its low toxicity and low immunogenicity [24]. β-cyclodextrin (β-CD) is the cheapest available CD [25] and its use to form OMZ inclusion complexes (OMZ-CD) could improve solubility and stability.
OMZ is known for being easily decomposed into a structure that is not efficiently absorbable by humans in an acidic environment, as its oral formulation is usually an enteric preparation [26]. The enteric coating protects the drug against gastric acid damage, but its release delays drug release. In February and March of 2006, the Food and Drug Administration of the United State (US FDA) approved OMZ capsules (OMZ/Sodium bicarbonate) and compound OMZ chewable tablets (OMZ/Sodium bicarbonate/magnesium hydroxide) respectively [27]. The specifications of the capsules were 20 mg/1100 mg and 40 mg/1100 mg, and those of the chewable tablets were 20 mg/0.6 g/0.7 g and 40 mg/0.6 g/0.7 g [28]. Both of these drugs have been formulated with the addition of micronized antacids [29], so that they can rapidly increase the pH of gastric juice to release OMZ, and rapidly reach the maximum concentration in plasma. However, the weight of the capsule contents is as high as 1160 mg [30], which makes swallowing difficult. It is therefore vital to use other safe antacids and reduce the weight of the preparations so that smaller capsules can be used to reduce swallowing difficulty.
In this study, we successfully prepared OMZ-CD, which were characterized and compared with micronized OMZ. An improved OMZ immediate-release capsule was prepared, and in vitro release behavior and pharmacokinetics studies in rabbits were investigated.
The following materials were obtained from commercial suppliers and used as received: OMZ (Shouguang Fukang Pharmaceutical Co., Ltd, China), OMZ Control (China National Institute for the Control of Pharmaceutical and Biological Products, China), β-CD (Anhui Sanhe Pharmaceutical Excipient Co., Ltd., China), Hydrocarbonate Sodium (NaHCO3, [Nanjing Chemical Reagent Co., Ltd., China]), Lightweight Magnesium Oxide (MgO, [Xisheng Scientific Co., China]), HPMC Capsule (0 #, [Suzhou Capsule Co., Ltd, China]). All other reagents were of analytical grade.
Briefly, the clathrate was prepared by the saturated aqueous solution method. The β-CD was completely dissolved in sodium hydroxide (NaOH) aqueous solution (pH = 11). Different amounts of OMZ powder were then added to the β-CD solution in a molar ratio of 1:1, 1:2, or 1:3. The mixture was stirred at different temperatures (30, 45, and 60 ℃) for 1, 3, and 5 h respectively. After the solution was left to cool to room temperature and stored at 4 ℃ for 12 hours, it was filtered by suction, washed with anhydrous ethanol three times, and vacuum dried at 25 ℃ for 12 hours to obtain OMZ-CD.
The encapsulation efficiency (EE) of OMZ-CD powder which we got was obtained by dissolving 10 mg of OMZ-CD in 50 mL of ethanol for 30 minutes under ultrasound. After dissolution, the sample was diluted to 100 mL with sterile ultra-pure water (ddH2O), and then analyzed with UV-752 spectrophotometer (Qinghua, Shanghai, China) at 302 nm (standard curve A = 0.0418C + 0.0159, R2 = 0.9992). The EE was calculated using the following equation:
The crystallinity of freshly prepared sample was obtained at room temperature by PXRD (MAX 2500 X-ray diffract meter, Rigaku, Japan). The step size is 0.02°. The angle is from 3° to 40°, scan speed of 8°/min on 40 mA, 40 kV conditions [31]. Samples were made from OMZ powder, simple β-CD powder, physical mixture of OMZ and β-CD, and milled OMZ-CD powder, then were analyzed after drying.
DSC-204 (Netzsch, Germany) system was used to obtain the thermo grams of the samples [32]. All experiments were operated from 45 to 300 ℃ at a heating rate of 10 ℃/min under constant purging of nitrogen at 20 mL/min. Samples were made from OMZ powder, simple β-CD powder, physical mixture of OMZ and β-CD, and milled OMZ-CD powder, then were analyzed after drying.
FTIR spectrometer (Paragon, 1000, PerkinElmer, USA) was used to obtain FTIR spectra at room temperature. OMZ powder, β-CD powder, physical mixture of OMZ and β-CD, and milled OMZ-CD powder were triturated with KBr in a ratio of 1:100 before pressed to form pellets. The scanned range was from 400 to 4000 cm−1 with the application of 16 scans at a nominal resolution of 4 cm−1. Samples were analyzed after drying [33].
The inclusion ratio was determined by the equimolar continuous change method [34,35]. Different concentrations of OMZ and β-CD mixed solution (total concentration of 1.0 × 10-4 mol/L) was prepared with pH 11 NaOH solution. The molar fraction of OMZ was from 0.1 to 0.9, the rest was β-CD. The solution was then incubated in a shaker at 200 rpm at 5 ℃ for 6 h, and left for 12 h. The optical density (OD) was measured with UV-752 spectrophotometer (Qinghua, Shanghai, China) at 302 nm with the NaOH solution at pH 11 used as blank. The inclusion ratio was determined based on the UV absorption data.
Equal doses (OMZ 20 mg) of OMZ, OMZ and β -CD, and OMZ-CD ware prepared with 1 × phosphate-buffered saline (PBS) pH 6.86 into a 10 mL brown volumetric flask, respectively. The solutions were placed in a 25 ℃ water bath thermoshake for 24 h to reach the equilibrium. After the shaking was completed, the suspension was centrifuged at 3500 rpm for 10 minutes and the precipitate was filtered through a 0.45 μm of microporous membrane. Then amount of OMZ in the filtrate was measured accordingly [36].
The concentration of OMZ was measured by high-performance liquid chromatography (HPLC) using LC-10AT (Shimadzu, Tokyo, Japan). All HPLC tests were carried out in a reversed-phase column (Inertsil® ODS-SP, 4.6 mm × 250 mm, i.d. 5 μm, GL Sciences, Tokyo, Japan) at 35 ℃ and under ultraviolet spectrophotometer at 302 nm. A mixture of methanol and water (75:25, v/v) was used as mobile phase at a flow rate of 1.0 mL/min. All measurements were performed in triplicate.
OMZ-CD powder and micronized OMZ were taken as the prescriptions and mixed with 50 mL of 0.1 mol/L hydrochloric acid (HCl) solution. A volume of 500 μL of the solution was sampled at 5, 10, 15, 20, 30, 45, and 60 minutes after stirring and filtered with a 0.45 μm-microporous membrane. An amount of 200 μL of the filtrate was accurately weighed, and 2 mL of 0.01 mol/L NaOH solution was added to be the test solution. The peak area was determined by HPLC (Shimadzu, Kyoto, Japan) to estimate the remaining drug content.
Pre-metered micronized OMZ, OMZ-CD powder, and OMZ and β-CD powder mixture containing the same amount of clathrate compound were respectively loaded into HPMC capsules. The release was performed in water and phosphate-buffered saline (PBS) pH 6.8, respectively. This study used the basket method in which the speed is 100 r/min and the temperature is (37 ± 0.5) ℃. A volume of 10 mL of solution was taken at 5, 10, 15, 20, 30, 45, and 60 minutes and immediately filtered through a 0.45 μm-microporous membrane. One milliliter of 0.1 mol/L NaOH solution was added to 5 mL of the filtrate (the test solution). The corresponding drug concentration and cumulative release percentage were calculated by HPLC peak area [37].
The pH-time curves of NaHCO3 and Na2CO3, MgO and Mg(OH)2 were compared to determine the type of antacid. The amount of one antacid was fixed while that of another antacid varied. The final amount of antacid was determined by comparison of the pH-time curves. The antacid was added to 50 mL of 0.1 mol/L HCl solution and stirred at a constant rate of 100 r/min. After 6 minutes, 1.0 mol/L HCl solution was added at a rate of 0.5 mL/min by a constant flow pump. The pH was measured with a pH meter (Inesa, Shanghai, China) [28].
The prescribed amount of OMZ-CD, NaHCO3, and MgO was sieved through 60 mesh 3 times, and the mixture was evenly filled into HPMC No. 0 capsules.
Marketed capsules and the capsules we developed were put into 50 mL of 0.1 mol/L HCl solution and stirred at a constant rate of 100 r/min. After 6 min, 1 mol/L HCl solution was added at a rate of 0.5 mL/min by a constant flow pump. All the solutions were incubated in a (37 ± 0.5)℃ -water bath during the entire process. At 5, 10, 15, 20, 30, 45, and 60 minutes, 500 μL of the solution were immediately collected and filtered with a 0.45 μm-microporous membrane. One milliliter of 0.01 mol/L NaOH solution was added to 100 μL of the filtrate (the test solution). The corresponding drug concentration and cumulative release percentage were calculated by HPLC peak area [28].
The animals were obtained from the Laboratory Animal Center of China Pharmaceutical University. Healthy New Zealand rabbits (weighing 1.6-2.0 kg) were fasted overnight and divided into two groups. Meeh-Rubner's formula was used to determine the dose and drugs were filled in small capsules to give the rabbits.
After a single oral administration of marketed compound capsules (ENCHENG®), about 2 mL blood samples were collected in heparinized tubes at 5, 10, 20, 30, 45, 60, 90, 120, 180, 240, 360, and 480 min. The blood samples were centrifuged at 4000 rpm for 10 min. The upper plasma was separated and kept at -20℃ until use [38].
Plasma sample was prepared by mixing 200 μL plasma and 200 μL β-naphthol methanol solution (10 μg/mL) as the internal standard substance. After being vortexed for 2 min, the mixture was centrifuged at 8000 rpm for 10 min to remove plasma proteins. The supernatant was injected into HPLC for analysis.
LC-10AT liquid chromatography (Shimadzu, Kyoto, Japan) was used for analysis. The tests were carried out in a reversed-phase column (Inertsil® ODS-SP, 4.6 mm × 250 mm, i.d. 5 μm, GL Sciences, Tokyo, Japan) at 35℃ and under ultraviolet spectrophotometer at 302 nm. A mixture of acetonitrile and water (55:45, v/v) was used as mobile phase at a flow rate of 1.0 mL/min. Methodological studies, e.g. precision of with-in and between days and recovery were demonstrated to meet the requirements of the methodology.
DAS 2.0 software (Shutcm, Shanghai, China) is used to analyze data. The peak plasma of drug concentration (Cmax) and the time to reach peak concentration (Tmax) were obtained from the plasma concentration–time curves of OMZ [39]. The linear trapezoidal rule was used to calculate the area under the plasma concentration-time curve (AUC).
Effect of different molar ratios of OMZ and β-CD, inclusion time and inclusion temperature on the EE (%) of OMZ-CD are shown in Table 1. With the same inclusion time and inclusion temperature, the EE (44.28 ± 1.71%) was the highest when the molar ratio of OMZ to β-CD was set to 1:2 and the inclusion time for 3 hours. Increasing of the temperature was beneficial to the improvement of the EE. When the inclusion temperatures were 30 ℃, 45 ℃, and 60 ℃, the EE were 44.28 ± 1.71%, 45.07 ± 1.29%, and 47.10 ± 0.63%, respectively.
Table 1: Effect of different molar ratios of OMZ and β-CD, inclusion time and temperature on the encapsulation efficiency of OMZ-CD (mean ± SD, n = 3).View Table 1
The pattern of X-ray diffraction, DSC and FTIR of OMZ, β -CD, physical mixture of OMZ and β -CD, and OMZ-CD are showed in Figure 1a, Figure 1b, and Figure 1c, respectively. The pattern of OMZ-CD was different from those of OMZ, β-CD, physical mixture of OMZ, and β-CD; while the pattern of physical mixture of OMZ and β-CD was just a superposition of those of OMZ and β-CD.
 Figure 1: Property investigation of OMZ-CD a) X-ray diffraction of samples; b) DSC thermograms of samples; c) FITR of samples; d) Determining of the inclusion ratio by the equimolar continuous change method. View Figure 1
Figure 1: Property investigation of OMZ-CD a) X-ray diffraction of samples; b) DSC thermograms of samples; c) FITR of samples; d) Determining of the inclusion ratio by the equimolar continuous change method. View Figure 1
The determination of inclusion ratio is showed in Figure 1d. The WOMZ*△A was used to plot the WOMZ. WOMZ referred to the molar fraction of OMZ in the mixture. ΔA referred to the difference in UV absorption intensity between OMZ before inclusion and OMZ after inclusion. The curve showed an arc. When the molar ratio of OMZ to β-CD was 1:1, the value of WOMZ*△A was the largest.
The result of saturated solubility of OMZ, physical mixture of OMZ and β-CD, and OMZ-CD in water and PBS pH 6.86 buffer are showed in Figure 2a. The saturation solubility of OMZ in water and PBS (pH 6.8) were 75.38 ± 1.52 μg/mL and 80.26 ± 1.50 μg/mL respectively. The saturation solubility of physical mixture of OMZ and β-CD was a little higher (121.66 ± 2.48 μg/mL in water, 118.29 ± 0.32 μg/mL in PBS pH 6.86) than that of OMZ. By contrast, the saturation solubility of OMZ-CD was increased by approximately 4.8 times and 3.5 times compared to that of OMZ in water and PBS (pH 6.8) respectively.
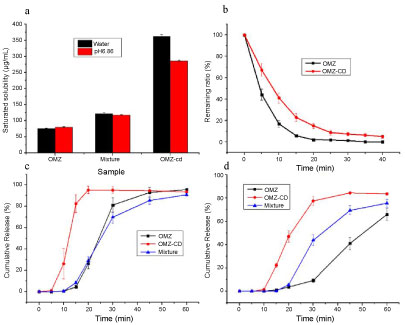 Figure 2: Property investigation of OMZ-CD a) Saturated solubility of OMZ, physical mixture of OMZ and β-CD, and OMZ-CD in water and pH 6.86 buffer; b) Acid resistance measurement of OMZ-CD and micronized OMZ; c) Dissolution profiles of OMZ releasing from micronized OMZ, OMZ-CD powder and mixture of OMZ and β-CD powders in water; d) Dissolution profiles of OMZ releasing from micronized OMZ, OMZ-CD powder and mixture of OMZ and β-CD powders in pH 6.86 media. Data are shown as the means ± SD (n = 3). View Figure 2
Figure 2: Property investigation of OMZ-CD a) Saturated solubility of OMZ, physical mixture of OMZ and β-CD, and OMZ-CD in water and pH 6.86 buffer; b) Acid resistance measurement of OMZ-CD and micronized OMZ; c) Dissolution profiles of OMZ releasing from micronized OMZ, OMZ-CD powder and mixture of OMZ and β-CD powders in water; d) Dissolution profiles of OMZ releasing from micronized OMZ, OMZ-CD powder and mixture of OMZ and β-CD powders in pH 6.86 media. Data are shown as the means ± SD (n = 3). View Figure 2
The plot of the content of OMZ-CD and micronized OMZ over time under simulated gastric acid conditions is shown in Figure 2b. OMZ was degraded very fast under acidic conditions, while the degradation rate reduced after being prepared as inclusion compound. After a certain time both were close to 0. Fitting the data by DAS 2.0 software (Shutcm, Shanghai, China), it was found that the half-life of the micronized drug substance was 4.00 ± 0.43 min, while it was 7.59 ± 0.83 min for OMZ-CD. The area under the curve of the latter was approximately 1.80 times than that of the former.
The dissolution profiles of micronized OMZ, OMZ-CD powder, and a mixture containing the same amount of OMZ and β-CD powders of the inclusion complex in water and PBS pH 6.8 are shown in Figure 2c and Figure 2d respectively. In water, the HPMC capsule ruptured in about 5 min and then the drug began to release. The release rate of OMZ-CD was significantly higher than that of micronized drug substances and mixtures, while the difference between the latter two was not obvious. OMZ-CD could release over 80% in 15 min and nearly 100% in 20 min. All the three could release more than 90% within 1 h. In phosphate-buffered saline (PBS) pH 6.8, the release of the three was lower than in water, and the difference was significant. The fastest was OMZ-CD, followed by the mixture, and the slowest was micronized drug substance.
Figure 3a and Figure 3b are the pH-time curves for the same mass of NaHCO3 and Na2CO3, MgO and Mg(OH)2, respectively. Figure 3c is a pH-time curve of immobilized 400 mg MgO screened for 150 mg, 250 mg, and 350 mg NaHCO3, respectively. Figure 3d is a pH-time curve of immobilized 250 mg NaHCO3 screened for 300 mg, 400 mg, and 500 mg MgO, respectively. Initially, the addition of an excess of antacid caused a rapid increase of the pH of the solution which stayed at a high value. As the hydrochloric acid was added, the excess antacid was completely attenuated, and thereafter, the pH dropped rapidly.
 Figure 3: Choice of antacids a) The pH-time curves of NaHCO3 and Na2CO3; b) The pH-time curves of MgO and Mg(OH)2; c) The pH-time curve of immobilized 400 mg MgO screened for 150 mg, 250 mg and 350 mg NaHCO3; d) The pH-time curve of immobilized 250 mg NaHCO3 screened for 300 mg, 400 mg and 500 mg MgO. View Figure 3
Figure 3: Choice of antacids a) The pH-time curves of NaHCO3 and Na2CO3; b) The pH-time curves of MgO and Mg(OH)2; c) The pH-time curve of immobilized 400 mg MgO screened for 150 mg, 250 mg and 350 mg NaHCO3; d) The pH-time curve of immobilized 250 mg NaHCO3 screened for 300 mg, 400 mg and 500 mg MgO. View Figure 3
The prescription information of both marketed compound OMZ capsules and compound OMZ capsules we developed are showed in Table 2. The appearance of the capsules is shown in Figure 4a. The capsules we developed were prepared by mixing and filling 170 mg of OMZ-CD, 250 mg of NaHCO3, and 400 mg of MgO into No. 0 HPMC capsules. By contrast, market capsules are prepared by mixing 1100 mg NaHCO3 and suitable recipients and filling into a No. 00 capsule.
Table 2: Prescription information of self-made capsules and market capsule. View Table 2
The dissolution profile of commercial formulations and the formulations we developed under simulated gastric acid conditions are indicated in Figure 4b. Y-axis indicates the ratio of the current drug content to the complete release of the drug, expressed in percentage. Commercial sample released very fast in the early stage, then, slowed down and the drug content began to decrease after the maximum release was reached. Finally, the drug content became 0. Same as the commercial sample, the inclusion compound capsules released rapidly at first. When reached the maximum level, the release stopped, then the drug content began to decrease to 0.
The plasma concentration-time curves after rabbits were fed marketed compound OMZ capsules and the tests are shown in Figure 5. The main pharmacokinetic parameters calculated from these data are shown in Table 3. Commercial capsules showed a typical immediate release curve, whereas the tests were more pronounced. The average value of Cmax was 686.06 ± 69.94 ng/mL after oral administration of the test, which was more than that of marketed capsules. The t1/2 of the test was 52.41 ± 8.45 min, while the value of marketed capsules was 44.11 ± 1.79 min. The relative bioavailability of OMZ was 138.88% compared to marketed capsules.
Table 3: Pharmacokinetics parameters obtained following oral administration of marketed capsules and the test to rabbits (mean ± SD, n = 3). View Table 3
OMZ is a highly lipophilic compound with low oral bioavailability that shows low stability related with rapid hydrolysis of its structure under acidic conditions (half-life of the micronized drug substance was 4.00 ± 0.43 min) (see Figure 2b). Also, OMZ is very poorly soluble [18]; the saturation solubility of OMZ in water and PBS (pH 6.8) were 75.38 ± 1.52 μg/mL and 80.26 ± 1.50 μg/mL (see Figure 2a). In an attempt to minimize these drawbacks, the aim of this work was to evaluate the capability of OMZ for the oral delivery of drug when associated to CD.
After being determined by the equimolar continuous change method [34-35], the result of inclusion ratio measurement showed that OMZ and β-CD were 1:1 inclusion (see Figure 1d), which meant that one OMZ molecule was linked to only one β-CD molecule, and one β-CD molecule was also related to only one OMZ molecule. But in the preparation of OMZ-CD, when the amount of β-CD was increased, the reaction equilibrium was promoted to move to the right, and thus the molar ratio of 1:2 to 1:1 had better EE (see Table 1). By contrast, when the molar ratio was 1:3, excessive β-CD was difficult to remove and the EE of the resulting product was reduced. Though increasing the temperature was beneficial to the improvement of the EE, but higher temperatures made OMZ more unstable and the solution turned yellow, decreasing the entrapment rate. Thus, from both the perspective of energy conservation and stability of drug, 30 ℃ was selected for the reaction temperature.
EE increased as the inclusion time increased, but decreased when the reaction time was too long. Stirring for a long time may destroy the weak intermolecular force of OMZ-CD, resulting in reduced packaging efficiency [36]. Consequently, OMZ-CD was prepared under the optimal conditions by stirring OMZ and β-CD at a molar ratio of 1:2 at a constant temperature of 30℃ for 3 hours.
We used X-ray diffraction, DSC, and FTIR to characterize the generated OMZ-CD. The X-ray diffraction pattern of physical mixture of OMZ and β-CD showed characteristic peaks at 2θ of 4.515, 9.019, 12.342, 12.778, 17.165, and 23.928 (see Figure 1a). All of these had appeared in the pattern of OMZ and β-CD, which meant the mixture was simple powder of OMZ and β-CD. But in the pattern of OMZ-CD, most of the characteristic peaks that consisted with OMZ disappeared. It showed that OMZ in the inclusion complex was not present in crystalline form but in amorphous state [33].
In Figure 1b, the DSC curve of OMZ showed that it was a typical crystalline anhydrous material. The sharp melting endotherm at 159.8℃ meant the melting point of the drug. The exothermic effect at 173.9 ℃ was due to its thermal decomposition [40]. The curve of β-CD showed a broad endothermic effect around 60 ℃ associated with crystal water losses [41]. The curve of the physical mixture of OMZ and β-CD showed that the characteristic peaks at 159.8 ℃ was still exist, meaning that OMZ had basically maintained its original crystallinity [42]. The disappearance of the OMZ melting point in the curve of OMZ-CD suggested the formation of a true inclusion complex [43].
In Figure 1c, OMZ had a complex absorption pattern below 1600 cm−1. However, β-CD absorbed more in the 3500-2800 cm−1 region. No new peaks appeared in the spectra of binary systems, meaning that no chemical bonds were created. The characteristic peaks of the drug could still be observed in the spectrum of the physical mixture, which was the superposition of the characteristic peaks of OMZ and β-CD. The two sharp peaks of OMZ at 1631.0 cm−1 and 1510.2 cm−1 which were CH deformation, CC stretching (P, BI) and CH + NH deformation (BI) [44], were significantly reduced in the diffractogram of the inclusion complexes. The bending vibrations of the methoxy groups of OMZ at 1204.6 cm−1 was decreased in the spectra of OMZ-CD because of the restriction due to the inclusion of this group within the CD cavity [33]. Therefore, it had been demonstrated that OMZ-CD had formed.
As a water-soluble auxiliary material, β-CD can improve the surface wet ability of OMZ to increase the saturation solubility of OMZ in the physical mixture. As a result, the saturation solubility of the physical mixture was slightly increased compared to that of the drug (see Figure 2a). However, the saturation solubility of OMZ-CD was increased more. This could explain the reason why inclusion compound let OMZ give a better performance in in vitro drug release (see Figure 2c and Figure 2d). OMZ is an acidic drug so it was more difficult to release in a buffered salt solution than in water. The difference in the saturation solubility of the three substances led to a more differentiated dissolution behavior when they released in phosphate-buffered saline (PBS) pH 6.8.
The commercial compound OMZ capsules were prepared by mixing large-dose antacids and suitable recipients and filling into a No. 00 capsule, making it large, heavy, and difficult to swallow [30]. To this end, this study also aimed to reduce the use of antacids and reduce the weight of the preparations by choosing other safe antacids.
The acid resistance of magnesium salt was higher than that of sodium salt (see Figure 3a and Figure 3b). However, sodium salt could generate a large number of bubbles when it came in contact with the acid solution, and quickly neutralized the acid while promoting dispersion. Therefore, the selected antacid was mainly magnesium salt to which was added a small amount of sodium salt to promote dispersion. MgO of the same quality had a higher acid-Fighting effect than Mg(OH)2 (see Figure 3b). Compared with Na2CO3, NaHCO3 was gentler with pH value (see Figure 3a). Ultimately, we have chosen a mixture of MgO and NaHCO3 as antacid.
In terms of screening of the amount of antacids, when amount of NaHCO3 was set as 150 mg, the pH value rose slowly and remained below 2.0 at 30 s after administration (see Figure 3c). This may result in the unavoidable degradation of OMZ once contacted with gastric acid in stomach, as the half-life of the OMZ-CD was only 7.59 ± 0.83 min (see Figure 2b). By contrast, the pH value rose faster to reach 6.0 at 30 s when the amount of NaHCO3 was 250 mg. According to a previous study [28], our investigations showed that the peak time of plasma concentration in vivo is about 30 min, and the time for 400 mg MgO to maintain pH above 6 is more than 35 min (see Figure 3d). In order to minimize the dose, 400 mg of MgO and 250 mg of NaHCO3 were selected as antacids. Thus, in the current study, we developed capsules with a better swallow compliance, which had a small volume and less weight by mixing and filling 170 mg of OMZ-CD, 250 mg of NaHCO3, and 400 mg of MgO into No. 0 HPMC capsules. The total weight of the capsule contents was 820 mg. However, the commercial capsule contents weigh up to 1160 mg and are filled with No. 00 capsule (see Figure 4a and Table 2). Investigations on both in vitro drug release (see Figure 4b) and in vivo pharmacokinetics (see Figure 5) showed that compound OMZ capsules that we developed had a better release performance.
With regard to in vitro drug release studies conducted on the compound capsule, the commercial sample released fast in the early stage due to the gas production of NaHCO3. However, due to the small amount of simulated gastric fluid, the prescribed amount of drug substance could not be completely dissolved therein. As the amount of solution increases, the release of the drug substance increased. After the antacids were all neutralized, the pH decreased and the drug substance degraded under acidic conditions. Therefore, the curve appeared to rise first and then decreased.
Because of the large solubility enhance effect of the prepared clathrate, OMZ in capsule that we developed could be completely dissolved under the simulated gastric acid conditions. As the commercial sample, the initial gas production of NaHCO3 allowed the inclusion compound to release rapidly. The presence of MgO maintained a relatively high pH for a relatively long period of time, so that the drug could maintain its maximum release over a long period of time. Similarly, the pH decreased and the drug degraded under acidic conditions after the antacids were all neutralized. Therefore, the curve of the capsules appear to rise rapidly first, maintain at a certain height, and then decrease.
Obviously, the capsules we developed had better release effects than the commercial ones in the simulated gastric environment. On the one hand, the capsules could maintain the pH at a higher level for a longer period of time due to changes in antacids, and OMZ prepared as a clathrate also had better acid stability (see Figure 2b). On the other hand, the solubility of the clathrate compound was greatly enhanced to the micronized drug substance (see Figure 2a), making it released faster and more thoroughly.
As for in vivo studies, the main pharmacokinetic parameters had been improved (see Table 3). Commercial capsules showed a typical immediate release curve, whereas the tests were more pronounced (see Figure 5), showing that the capsules we developed have the potential to perform faster and better.
Several limitations should be acknowledged in the present study. First, the EE was not high enough and the preparation of OMZ-CD increased the weight of the capsule. Second, the pharmacokinetic data lacked the support of human trials. Therefore, further studies would be required to test the new compound OMZ capsules.
This study developed an improved compound OMZ capsule, which could achieve immediate drug release and high anti-acid ability for improved therapeutic effect for ARDs. The β-CD inclusion technology guaranteed high solubility and stability of OMZ in stomach acids. And the screened antacids ensured that the designed capsules possessed lighter weight and higher acid resistance ability compared to commercial capsules. Stomach acid is first neutralized by antacids which lead to the increase of pH after taking the capsule, thus, allowing drugs to release faster and longer. Both in vitro and in vivo investigations have showed that this new capsule is highly fast release and has improved bioavailability compared with the commercially available compound OMZ capsules. Due to the immediate release in the stomach, drug efficacy is produced within few minutes after taking the drug, which can greatly reduce the patient's pain.
The authors gratefully acknowledge the support from National Natural Science Foundation of China (No. 81402859), Top-notch Academic Programs Project of Jiangsu Higher Education Institutions (PPZY2015B164), Administration of Traditional Chinese Medicine of Zhejiang Province (Program No. 2017ZA075).