Peritoneal dialysis related peritonitis is a major risk factor for drop-out of patients on continuous ambulatory peritoneal dialysis. Data on factors affecting outcome of chronic peritoneal dialysis related peritonitis and microbiology is limited. In this regard, a retrospective, observational study was conducted at Post Graduate Institute of Medical Education and Research, Chandigarh, India, wherein we reviewed medical records of chronic peritoneal dialysis patients for 3 years between 01 July 2015 and 30 June 2018. We abstracted data pertaining to social, demographic and clinical characteristics of patients, occurrence of peritonitis including microbiological spectrum and outcomes. Conventional culture method involving manual inoculation was used in initial 1½ years, after which automated culture (BACTEC) was used. A total of 334 chronic peritoneal dialysis patients were screened retrospectively for infective peritonitis. Out of these, 74 patients had 97 episodes of peritonitis; 54 patients had single episode and 19 had two episodes (repeat-16 and relapsing-3) and none had preceding or ongoing exit site or tunnel infection. Occurrence of peritonitis was highest during monsoon (36%) and least during autumn (12%). Cumulative culture positivity was 39.2% with gram-positivity in 60.5% patients. Predominant microorganism was Staphylococcus epidermidis (23.7%) followed by Escherichia coli (13.2%). 51 patients (74 episodes) recovered with antibiotic therapy alone, while 23 patients required peritoneal catheter removal in view of refractory (n-20)/fungal (n-3) peritonitis. 6.8% patients had peritonitis related mortality. Outcome with respect to recovery was comparable (76.3%) in culture positive and culture negative episodes.
Peritoneal dialysis related peritonitis, Culture negative peritonitis, Seasonal variation, Treatment outcome
In India, it is estimated that over 150 per million persons develop end-stage renal disease (ESRD) each year [1]. Hemodialysis (HD) is the most common renal replacement modality, followed by transplantation and peritoneal dialysis (PD) is distant third, usually per-force choice for patients in whom HD is either not feasible (difficult terrain, affordability, arterio-venous access related issues) or is contraindicated [2].
It is estimated that chronic PD is utilized as a modality for long-term dialysis in more than 8500 patients in India [3]. Despite advancements in technique and new generation of solutions [4], infective peritonitis (about 0.5 episodes per patient per year) remains a major cause of PD drop-out, besides catheter loss and transfer to HD [5]. Multiple risk factors such as socio-demographic, climate change, diabetes and presence of tunnel/exit site infection have been associated with development of peritonitis.
Microbiological spectrum of PD peritonitis in developing countries may be different from developed countries, possibly due to differences in social, cultural and environmental practices [6]. There has been an increasing trend in the incidence of gram-negative peritonitis [7]. Early diagnosis with prompt initiation of therapy is critical in preventing adverse outcomes [8]. The contemporary focus has shifted from lowering peritonitis rates to improving outcome by early identification of culprit organisms [9].
With this background, we aimed to determine the incidence of infective peritonitis including microbiological spectrum and assess clinical outcomes following infective PD peritonitis.
This is a single center, retrospective, observational study conducted by the department of Nephrology, PGIMER, Chandigarh, India. Our department provides both outpatient as well as inpatient services to over 100 chronic PD [continuous ambulatory peritoneal dialysis (CAPD)/automated peritoneal dialysis (APD)] patients per month (including new as well as established patients), hailing primarily from northern and central India. All ESRD patients on chronic PD (CAPD/APD) who had attended the PD clinic from 01 July 2015 till 30 June 2018 were screened retrospectively for infective PD peritonitis. We identified patients who had infective PD peritonitis according to the International Society of Peritoneal Dialysis (ISPD) 2016 guidelines [10]. Patients with history of peritonitis in preceding one month, use of immunosuppressants (except topical steroid) and peritonitis secondary to non-infective causes were excluded.
Medical records were retrospectively screened to enroll eligible patients and information related to demographic and clinical characteristics; type of peritonitis, time taken for developing current peritonitis episode and type of dialysis solution (glucose/non-glucose based) was abstracted. Seasonal variation of the episodes (Winter - December to February; Summer - March to June; Monsoon - July to September; Autumn - October to November) was also assessed.
Conventional culture method (involving manual inoculation and enrichment step followed by plating with selective media) was used in the initial 1½ years (01 July 2015 - 31 December 2016) followed by automated culture method - BACTEC (01 January 2017 - 30 June 2018) for processing of test samples. Laboratory data (total and differential cell count, gram stain, culture and sensitivity of dialysate effluent and complete blood count) were recorded at baseline.
Follow-up data was collected on day 3 ± 1 (visit 2), 5 ± 1 (visit 3), 14 ± 2 (visit 4) and 45 ± 7 (visit 5). Peritonitis related mortality was defined as death occurring with a positive peritoneal dialysate culture/due to sepsis, during hospitalization for peritonitis or within 4 weeks after onset of peritonitis [11].
Empirical intra-peritoneal (IP) antibiotics (vancomycin and ceftazidime) targeting both gram-positive and gram-negative organisms were started in treatment naïve patients as per departmental protocol and were thereafter revised based on culture and sensitivity reports. Patients already initiated on antibiotics from referring hospital whether IP/parenteral were continued/revised as per sensitivity reports/clinical assessment. Any clinical deterioration (onset of systemic features/severe sepsis/shock) mandated switch from IP to parenteral antibiotics. Antifungal prophylaxis was initiated from 5th day onwards in all non/slowly resolving/refractory peritonitis episodes.
All enrolled patients with non-missing outcome data were included for analysis. Descriptive statistics were used to describe characteristics of study subjects. Data has been presented as mean ± SD (95% CI) and median (interquartile range) as appropriate. Categorical variables such as gender and co-morbidities were expressed in percentage. Frequency of peritonitis by gram-positive/gram-negative organisms, Mycobacterium tuberculosis and fungus was also estimated and expressed in percentage. Two-tailed P values < 0.05 were considered statistically significant.
A total of 334 patients on chronic PD were screened retrospectively for peritonitis. 88 patients had abdominal pain with turbid effluent; however, 14 patients with non-infective etiology were excluded (Figure 1). A total of 74 patients (Males - 43; Females - 31) with overall 97 peritonitis episodes were observed during the study period (Figure 2).
 Figure 1: Study design.
View Figure 1
Figure 1: Study design.
View Figure 1
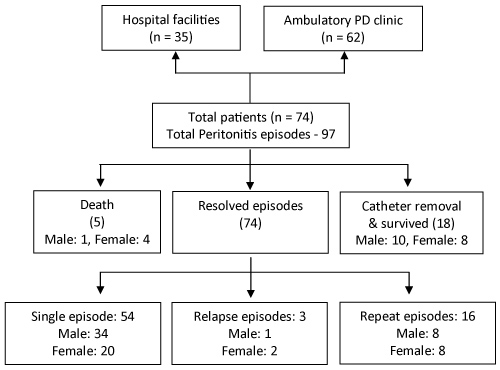 Figure 2: Follow up and outcomes of peritonitis.
View Figure 2
Figure 2: Follow up and outcomes of peritonitis.
View Figure 2
The mean (standard deviation) age (years) was 54.69 (12.3) for males and 55.24 (14.4) for females. The median (range) duration (years) of ESRD was 3.45 (0.15-13.68) and that of peritoneal catheterisation was 2.54 (0.02-13.21), respectively. A total of 37 (50%) patients had opted for CAPD while remaining were compelled either due to arterio-venous access related issues - 14 (19%) or not tolerating HD - 23 (31%). Baseline demographic parameters in index study as summarized in Table 1 did not differ between either sex except for proportion of male chronic PD patients who received services of care-giver (mostly wives) was statistically significant (p < 0.02) in comparison to female chronic PD patients who mostly self-performed, nevertheless incidence of peritonitis was matched.
Table 1: Demographic characteristics. View Table 1
Of the 74 patients, 64 (86%) were on CAPD with median (range) duration (months) of 12.58 (0.8-134) and 10 (14%) were on APD with median duration (months) of 9.13 (3.8-16.3). Underlying renal disease was diabetic nephropathy in 33 (44.6%) patients, chronic glomerulonephritis in 15 (20.3%) and remained idiopathic in 26 (35.1%) patients. Glucose-based dialysis fluid was used in 60 (81.1%) patients with additional icodextrin use in 14 (18.9%) patients. Majority (79.7%, n = 59) had undergone 3 × 2 L exchanges/day.
Overall 54 patients had single episode of peritonitis (Males - 34, Females - 20). 19 patients had second episode (Males - 8, Females - 11) with majority being repeat episodes {n-16; median duration of 77 (32-375) days}. 3 patients had relapsing peritonitis; median duration of 14 (10-25 days) and a single male patient had five episodes of infective PD peritonitis. No patient had prior or ongoing exit site or tunnel infection. Amongst 19 patients who had second episode of peritonitis, only identifiable breach in technique was a recent change in the caretaker in 13 patients, of which only 4 patients had formal training in PD care. We observed that the frequency of peritonitis episodes (36%, n = 35) was highest during the monsoon season (Table 2) followed by (30%, n = 29) episodes during winter and least (12%, n = 12) peritonitis episodes during autumn.
Table 2: Micro-organism wise - monthly distribution of peritonitis. View Table 2
At baseline, all individuals had cloudy effluent. At presentation, there was increased dialysate leukocyte count with median (range) count of 900 (150-15000) cells/mm3, and differential count had neutrophil predominance [median (range) - 81% (68-100)]. A total of 16 different micro-organisms were isolated (Table 3) with cumulative culture positivity in 39.2% (n = 38/97). In initial 1½ years culture positivity was noted in 32.7% (n = 16/49) and increased to 45.8% (n = 22/48) with use of automated culture technique in the latter half of study period. All culture positive samples demonstrated single micro-organism. Among culture positive episodes, 60.5% (n = 23/38) and 31.6% (n = 12/38) were caused by gram-positive and gram-negative microorganisms respectively with predominant microorganism being Staphylococcus epidermidis (23.7%) followed by Escherichia coli (13.2%). Three peritonitis episodes (7.7%) were caused by Candida species. Diagnosis of tubercular etiology in two patients was retrospective following peritoneal catheter removal through contrast imaging and omental biopsy; both patients improved after anti-tubercular therapy (ATT) and subsequently opted for HD modality.
Table 3: Micro-organism wise peritonitis episodes and outcome. View Table 3
The most frequently prescribed antibiotics were IP vancomycin and ceftazidime as per our departmental protocol. Switch from IP to parenteral antibiotics in view of clinical deterioration (onset of systemic features /severe sepsis /shock) was required in 23% of peritonitis episodes.
Recovery was noted in 68.9% patients (n = 51/74) and 74.8% episodes (n = 74/97). 63.9% (n = 62/97) of infective peritonitis episodes were managed in outpatient setting. However, 36.1% (n = 35/97) of infective peritonitis episodes necessitated inpatient management. 23 patients required removal of peritoneal catheter in lieu of refractory (n-20)/fungal (n-3) peritonitis. Mortality related to peritonitis was seen in 5 patients {Escherichia coli-1, Candida-1, culture negative-3}. Outcomes with respect to recovery were comparable (76.3%) in both culture-positive (n = 29/38) and culture-negative (n = 45/59) episodes. Staphylococcus epidermidis peritonitis was observed in 9 patients out of which 8 recovered and 1 required peritoneal catheter removal. Escherichia coli peritonitis was observed in 5 patients out of which 2 recovered, 2 required peritoneal catheter removal and 1 patient expired following refractory septic shock. Overall 6.8% (n = 5/74) patients had peritonitis related mortality (Escherichia coli-1, Candida-1 and culture negative-3).
This study spanning over 3 years offers insight into the etiology and outcomes of PD related peritonitis in patients on CAPD from northern India, which is germane to clinical decision making. Overall peritonitis rate observed in our study was 0.74 episodes per patient per year, which is more than the recommended guidelines of less than 0.5 episodes per patient per year. Most of the peritonitis episodes were managed on out-patient basis, however hospitalization was necessary in about 36% of total peritonitis episodes.
Our study has demonstrated an overall high culture negative rate (60.82%); value far greater than that suggested in ISPD guidelines (< 20%). Culture negativity rate between 28-70% with conventional culture technique [12] and over 50% with use of automated system has already been reported [13] from the Indian sub-continent and summarized in Table 4. Higher culture-negative peritonitis in present study is probably multifactorial with administration of antibiotics before dialysate evaluation in 22% of culture negative peritonitis episodes, might have contributed to false culture negativity. Further non-adherence to ISPD recommendations with regard to culture specimen collection and processing methods during use of conventional techniques might also have contributed to culture negativity. However, sample size is too small to draw firm conclusions.
Table 4: Indian studies: CAPD Peritonitis. View Table 4
We observed higher incidence of gram-positive peritonitis (58.9%) than gram-negative (30.8%); (p < 0.004) results were similar to a study in South India by Gupta, et al. (2011). Nevertheless, clinical recovery in our study was comparable (76.3%) in both culture positive and culture negative peritonitis. Better recovery rate may point towards proper and timely use of empirical antibiotics and later supported by culture and antibiotic susceptibility results.
Initial empirical antibiotic prescription is dictated by local epidemiology, sensitivity pattern, convenience of self-administration by the patient, drug's pharmacokinetics, its cost and effectiveness; and usually includes drugs covering both gram-positive and gram-negative organisms. In the present study, IP vancomycin and ceftazidime were the most frequently prescribed antibiotics, based on favorable pharmacokinetics of vancomycin allowing IP dosing at weekly intervals [14] and literature evidence [15,16].
Incidence of fungal peritonitis in our study (7.7%) was comparable with regards to available literature evidence [17], possibly due to initiation of oral fluconazole prophylaxis from 5th day onwards in all non-resolving [18]/slowly resolving/refractory peritonitis episodes.
Diagnosis of tubercular etiology in 2 patients was made only when fever persisted despite peritoneal catheter removal with raised adenosine deaminase (ADA) in ascitic fluid, necrotic retroperitoneal lymphadenopathy on contrast imaging and omental biopsy revealing caseating necrosis. Improvement following initiation of ATT further confirmed tubercular etiology. Microscopic smear detection of acid-fast bacilli in the dialysate is relatively insensitive [19], with reported sensitivity ranging from 0% to 6% and conventional microbiological diagnostic methods are slow and may not be sensitive enough for establishing diagnosis in a timely manner [20]. We re-emphasize that higher index of clinical suspicion, directed evaluation towards tubercular etiology particularly in culture negative refractory peritonitis and timely institution of ATT may not only help in restoring peritoneal integrity, thereby salvaging the catheter but also helps avoiding PD drop-out.
An in-depth analysis of the reasons for high culture negativity is imperative, nevertheless prompt recognition with early institution of appropriate antibiotics remains pivotal in improving peritonitis outcome.
Although our study lacked standardized culture methods, treatment regimens and standardized indications for treatment change by virtue of its observational and retrospective nature, besides limitation of being a single center study, nevertheless reiterates improved culture positivity with automated culture techniques over conventional culture method.
This single center study is probably one of the largest in terms of cohort and period of time from northern India to describe the demography, microbiology and treatment outcomes of infective PD peritonitis. Information with respect to the seasonal variation and outcomes of peritonitis may help in prognostication besides guiding clinicians to take adequate preventive and therapeutic measures.
The authors would like to place on record the contributions of Baxter India Pvt. Ltd. for helping in coordinating this study.
Authors report no conflict of interest.
Nil.