Current first-line treatments for idiopathic membranous nephropathy often insufficiently reduce proteinuria and creatinine. Additional treatments options are needed for these refractory cases. Herein, we describe the case of a 68-year-old white male with worsening dyspnea and peripheral lower extremity edema with biopsy-proven membranous nephropathy, without any identifiable secondary causes of the disease. He failed to achieve partial or complete remission after initial therapy of enalapril, atorvastatin and furosemide followed by several regimens containing corticosteroids, cyclophosphamide, cyclosporine, myclophenalate mofetil, and rituximab. However, he had an excellent response to H.P. Acthar® gel, achieving complete remission of proteinuria and marked improvement in renal function. After 12-months standard therapy, his 24-hour urine protein decreased from 15.020 g to 0.380 g and serum creatinine from 1.94 mg/dL to 1.53 mg/dL. Upon cessation for three months, however, he relapsed. H.P. Acthar® therapy was restarted and continued as maintenance drug for 30-months, after which his 24-hour urine protein reached its lowest of 0.282 g and serum creatinine 1.27 mg/dL. The patient remained symptom-free and endorsed a better quality of life. While other case reports describe patients using ACTH gel as a maintenance therapy, none thus far has extended therapy to 30-months.
Idiopathic membranous nephropathy, Nephrotic syndrome, ACTH gel
Idiopathic membranous nephropathy or primary membranous nephropathy is a subtype of nephrotic syndrome, autoimmune in origin with antibodies against a glomerular podocyte membrane protein receptor [1]. Gold standard for diagnosis is renal biopsy, however, biomarker staining can aid in diagnosis, including anti-phospholipase A2 receptor (PLA2R) antibodies and overall IgG or individual IgG subclasses [2]. Furthermore, potential secondary causes of membranous nephropathy must also be excluded, such as certain drugs, toxins, malignancies, infections and autoimmune diseases. First-line therapy consists of corticosteroids and alkylating agents, specifically cyclophosphamide, cyclosporine, mycophenolate mofetil as well as rituximab, which are often resistant [3]. Although therapeutic options for idiopathic membranous nephropathy remain limited, they have demonstrated potential control of proteinuria with complete or partial remission of nephrotic syndrome associated with a slower rate of disease progression and prolonged renal survival [4]. Most recently, refractory cases have shown sufficient response to 12-months course of intramuscular natural ACTH, derived from porcine pituitary gland, known as H.P. Acthar® therapy.
We present a case of a 68-year-old Caucasian male with a past medical history significant for essential hypertension on oral enalapril 20 mg daily and no prior history of diabetes. He presented with complaints of mild dyspnea and progressively worsening peripheral lower extremity edema for several weeks. On initial evaluation, his blood pressure was 134/82 mmHg, heart rate was 76 bpm, and he had 3+ pitting edema in bilateral distal lower extremities up to his knees. Laboratory tests were remarkable for serum creatinine 1.82 mg/dL (normal range 0.7-1.2 mg/dL), plasma glucose 96 mg/dL (normal range 70-130 mg/dL), total cholesterol 212 mg/dL (normal range < 200 mg/dL), LDL cholesterol 127 mg/dL (normal range < 100 mg/dL), and 24-hour urine protein 13.650 g (normal range < 150 mg). Medications were optimized with higher dose enalapril, addition of furosemide as well as atorvastatin and starting a low salt, low protein diet. He subsequently had a renal biopsy which revealed some globally sclerotic glomeruli on light microscopy, granular global sub-epithelial deposits on immunofluorescence and global sub-epithelial electron dense deposits with complete effacement of podocyte foot processes on electron microscopy, all of which are consistent with membranous nephropathy. Additionally, biopsy stained positive for IgG, C3, kappa and lambda. Of note, the anti-phospholipase A2 receptor (PLA2R) antibody staining was not performed on the biopsy but patient was seropositive for anti-PLA2R antibodies prior to any treatment and only when available was followed before and after each treatment [5]. It was also not stained for IgG subclasses. After the biopsy results were obtained, patient had age-specific cancer screening including PSA and colonoscopy, as well as Hepatitis B, Hepatitis C, RPR and ANA screening to rule out secondary causes of membranous nephropathy. All exclusionary criteria were met and the patient was diagnosed with idiopathic membranous nephropathy.
We initiated several first-line treatment regimens as per KDIGO guidelines, including steroids, cyclophosphamide, cyclosporine, mycophenolate mofetil and rituximab [6]. Their respective outcomes were evaluated as follows. Complete remission was defined as 24-hour urine protein < 0.3 g, on two consecutive values greater than one week apart, with normal serum albumin (3.4 to 5.4 g/dL) and normal serum creatinine. Partial remission was defined as 24-hour urine protein < 3.5 g and 50% or greater reduction from baseline values with similar parameters as above. If neither complete nor partial remission was achieved, they are classified as non-responders. Additionally, relapse was defined as an increase in 24-hour urine protein > 3 g after achievement of complete remission or a novel increase in proteinuria after achievement of partial remission.
Initial treatment management was a six month modified Ponticelli regimen, which included alternating monthly cycles of intravenous corticosteroids and cyclophosphamide, with post-treatment 24-hour urine protein 12.62 g and serum creatinine 1.74 mg/dL [7]. This was followed by six months of cyclosporine with post-treatment 24-hour urine protein 10.36 g and serum creatinine 1.86 mg/dL. Next, he finished an eight month course of mycophenolate mofetil, with post-treatment 24-hour urine protein 10.72 g and serum creatinine 1.88 mg/dL. Finally, patient received rituximab 375 mg/m2 given as four times weekly intravenous infusions for one month duration, with post-treatment 24-hour urine protein 9.63 g and serum creatinine 1.67 mg/dL. At this time, patient was determined to be a non-responder. There was a gap of four months when patient returned with worsening progression of his glomerulopathy with a 24-hour urine protein 15.020 g and serum creatinine 1.94 mg/dL.
We initiated H.P. Acthar® gel therapy, 80 units subcutaneous corticotrophin administrated twice weekly. After 12-months, his 24-hour urine protein markedly decreased to 0.380 g and his serum creatinine decreased to 1.53 mg/dL. Acthar® therapy was considered completed. After three months of cessation, patient relapsed and his 24-hour urine protein increased to 3.105 g and serum creatinine increased to 1.75 mg/dL. Acthar® therapy was restarted and continued for 2.5 years. At 6-months, patient demonstrated reduction of his 24-hour urine protein, at 0.382 g. After 30-months, patient achieved complete remission of proteinuria on continuous Acthar® maintenance with 24-urine protein 0.282 g and serum creatinine 1.27 mg/dL (Figure 1 and Figure 2). No adverse reactions were noted.
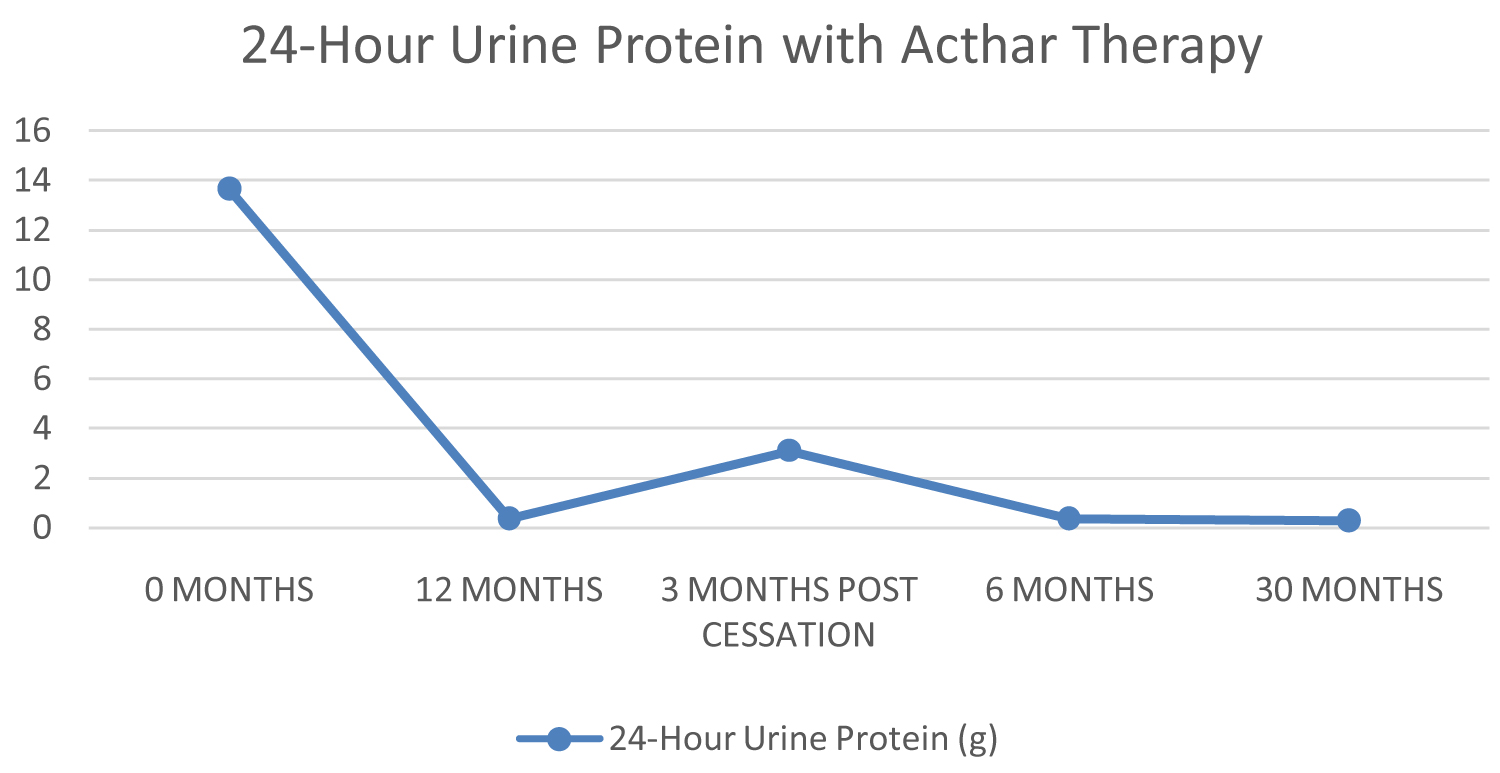 Figure 1: 24-hour urine protein during increasing length of treatment duration.
View Figure 1
Figure 1: 24-hour urine protein during increasing length of treatment duration.
View Figure 1
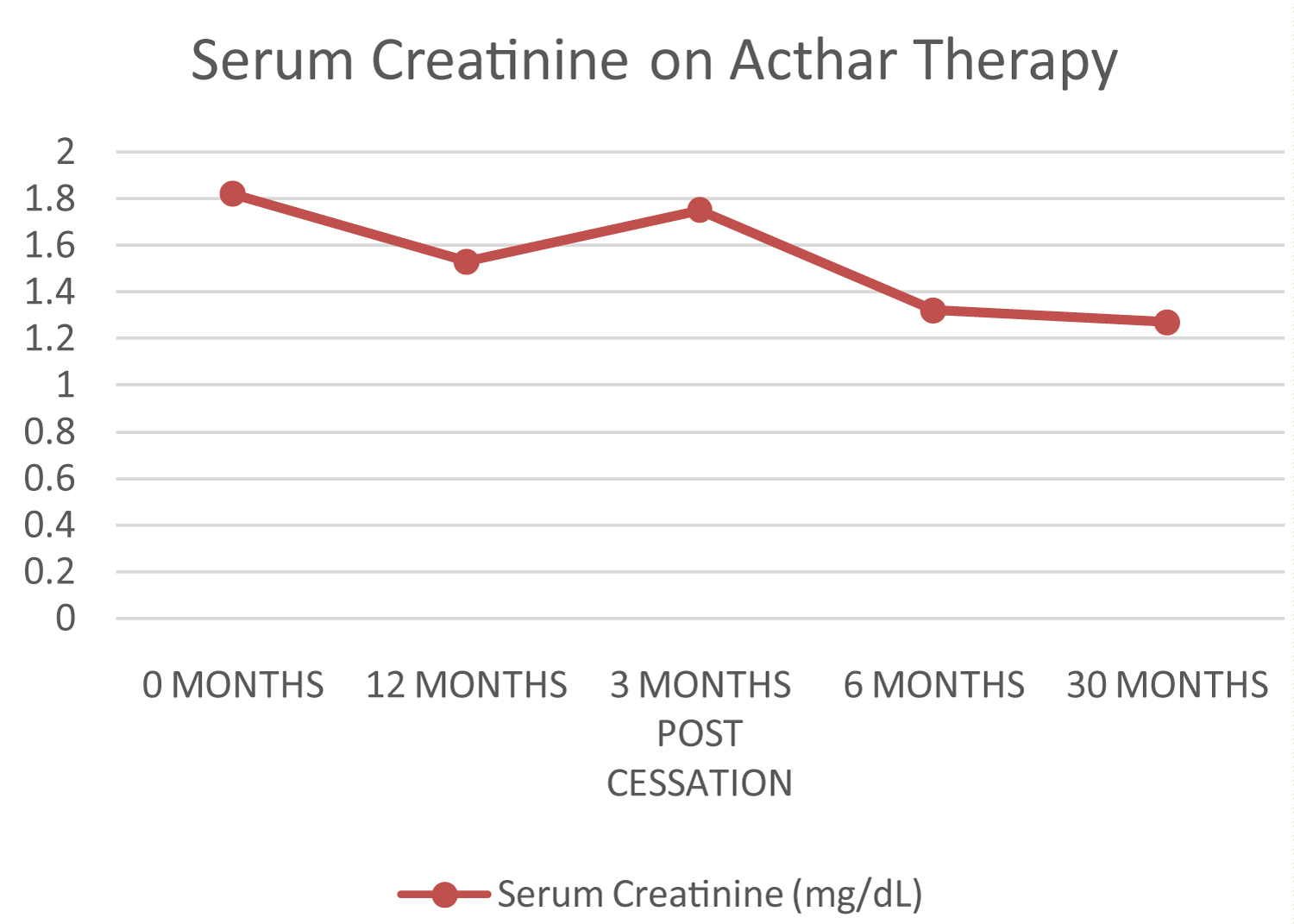 Figure 2: Serum creatinine during increasing length of treatment duration.
View Figure 2
Figure 2: Serum creatinine during increasing length of treatment duration.
View Figure 2
Acthar® therapy provided complete remission in 12-months for this case of refractory idiopathic membranous nephropathy, but when discontinued for three months, the patient relapsed. Upon re-initiation of H.P. Acthar® gel, patient again went into complete remission and sustained in remission for 30-months. The patient tolerated the extended therapy well; he remained symptom-free with no drug side effects, including dizziness, diarrhea, and glucose intolerance. Moreover, he endorsed an improvement in quality of life and was able to return to his previous daily routine with resolution of shortness of breath and lower extremity edema.
Although this therapy has shown clinical improvement, mechanism of action remains unknown. One theory is that ACTH binds directly to melanocortin-1 receptors on podocytes; this, in turn, may stabilize the podocyte actin cytoskeleton, decrease effacement of foot processes and decrease glomerular permeability [8]. Others postulate that ACTH binds directly to hyperactive immune cells, including B and T lymphocytes, which decreases autoantibody production and down regulates pro-inflammatory mediators [9]. It also should be noted that ACTH gel for idiopathic glomerular nephropathy is not curative, but it demonstrates potential in reducing symptoms for high grade proteinuria resistant to first-line therapies.
While H.P. Acthar® gel therapy is given for 12-months in refractory primary membranous nephropathy, there is no optimal treatment duration [10]. A few case studies described similar findings with maintenance Acthar® therapy but for a shorter duration than our patient. Watson presented a 46-year-old Caucasian male patient with biopsy proven idiopathic membranous nephropathy resistant to first-line therapy, who demonstrated complete remission with H.P. Acthar® gel after 10-months and sustained remission after 13-months of therapy [11]. Another case study described a 20-year-old female with biopsy-proven idiopathic membranous nephropathy resistant to steroids and cyclosporine therapy but demonstrated complete remission with 24-months of a synthetic ACTH analog [12].
Our case showed H.P. Acthar® gel therapy was effective not only in the short-term but possibly anti-proteinuric and renoprotective with cumulative doses in the long-term. Maintenance Acthar® therapy may be a potential therapy in refractory idiopathic membranous nephropathy but requires further evaluation and trials to define its role.