Onychomycosis is fungal nail infection, which can be associated with some factors, such as decreased nail growth and immunodeficiency, makes the elderly predisposed to onychomycosis. The objective of this study was to investigate the frequency of onychomycosis in elderly institutionalized, and to verify the effects that the infection had in their daily routine.
This study was carried in gerontological complexes of Goiânia, Goiás, Brazil, with 58 elderly who exhibited clinical suspicion of onychomycosis and a questionnaire was provided to the elderly regarding the effects that the infection had in their daily routine.
Among the 33 cases of the onychomycosis confirmed, 63.6% were female and 36.4% male. The participant ages ranged from 55 to 86 years (51.3 years ± SD = 32.8). In this study, no statistically significant between age (p = 0.362) and sex (p = 0.234) associated of Onychomycosis in institutionalized elderly. The etiological agents Trichophyton rubrum were isolated in 9.1% and Fusarium spp. in 15% of the positive samples. The genus Candida was identified in 46.5% of the samples, and Candida parapsilosis (30.3%) was the most frequent species. The applied questionnaire verified that more than 90% of participants answered that other people notice the presence of the nail lesion; That the of nail injuries influences their choice of shoes; and that perceive the difference in nail characteristics, such as thickness and discoloration.
This study found a higher frequency of onychomycosis in women, and the main etiological agents were Candida spp. and Fusarium spp. The onychomycosis significantly changes the routine of its patients, with most participants reporting that people find it unpleasant to look at their nails and note the problem and they are uncomfortable with the appearance of the lesion. In clinical question, the participants also notice the change in the characteristics of their nails, difficulty in cutting and, nail and finger/toe pain.
Onychomycosis, Elderly, Dermatophytes, Fusarium, Candida parapsilosis
Onychomycosis is an infectious cutaneous disease caused by fungi and occurs in fingernails and toenails. The etiological agents come from three distinct groups of fungi: Dermatophytes, yeasts, or non-dermatophytic filamentous fungi (NDFF) [1,2]. This infection is common in the world population, accounting for about 50% of the nail disorders [3].
Knowledge of the frequency of onychomycosis is important due to the clinical damage that it inflicts on patients. Although this infection does not cause mortality, the inflammatory process in the nail plate can cause pain, lead to difficulties in carrying out daily activities that generate discomforts. Two main types of discomforts may be associated with this ailment: Physical, which mostly related to aesthetics, and psychological, due to the constant constraints, which can lead to depression and anxiety that significantly interferes with individual's well-being and daily life [4,5].
The occurrence of onychomycosis increases according to the age of the studied population, with a predominance in elderly people over 60-years-old [1]. This fact can be explained by the presence of some predisposing factors that are more frequent in individuals at this age and older, such as angiopathy, peripheral neuropathy, use of closed shoes, nail deformity, recurrent traumas, and metabolic disorders such as diabetes mellitus [2]. An example that explains the importance of the knowledge of onychomycosis in the elderly consists of a clinical complication with the evolution for uncontrolled diabetes mellitus. In this case, the evolution of the infection can associated with altered vascular supply, and reduced capacity for tissue repair leading to complications such as gangrene and/or foot ulcer with consequence limb lower amputations [5,6].
Therefore, to avoid a worse prognosis of comorbidities in the elderly, a laboratory diagnosis of onychomycosis is considered very important, because fungal infections cannot be solely defined by the clinical characteristics of the lesions [2,7]. In addition, the correct identification of the etiological agent can help determine the most appropriate choice of treatment, avoiding the relapses of this fungal infection [7]. Thus, the objective of this study was to investigate the frequency of onychomycosis in elderly patients institutionalized in two gerontological complexes in the city of Goiânia, Goiás, Brazil, in addition to verified using a questionnaire, the effects that the infection had in the daily routine of those elderly participants.
A prospective study was conducted in 2016 with individuals institutionalized in two gerontological complexes, located in the Southern and Western regions of the city of Goiânia, in the state of Goiás, Brazil, after approval of the Research Ethics Committee of the University Paulista, number 1,438,062. The gerontological complexes included in the research are institutions in which the elderly are independent during the daily routine. They are elderly with capacity in the execution of physical, social and laser activities, as dance; and also with ability to understand the explanation of the research objectives in the invitation made by the researchers. All participants signed the informed consent form (ICF), and the identifying information remained in absolute secrecy. The researchers responsible with extensive experience in medical mycology carried out the inclusion of the elderly participants in the research, where they established clinical criteria such as subungual hyperkeratosis, inflammatory reaction, color change, dystrophy and onycholysis and destruction of the entire nails plate, so that subungueal scraping was performed. After completing the work all, the participants received the results of the mycological examination and then they were referred to the responsible doctor for each unit for that is prescribed the appropriate treatment.
This study included individuals in the gerontological complexes, 55 years of age or older, and presenting clinical manifestations characteristic of onychomycosis in their fingernails or toenails. In addition, severity of fungal infection damage was classified as mild (< 4 nails involved), moderate (5-8 nails involved) and severe (≥ 9 nails involved) [6]. Individuals who did not accept the terms established in the ICF were excluded from the survey. During the collection of biological material, a questionnaire was given to the participants to verify their main complaints against onychomycosis in their daily routine. The questions were grouped into social, emotional, and clinical; and the answers were standardized as "yes" or "no".
The material was obtained by subungual scraping using blunt scalpels. An antisepsis was performed on the nail with 70% alcohol, and then the material was removed from the more peripheral regions of the lesion, in the transition limit between the normal and infected nail. The clinical material was then sent to the Instituto de Patologia Tropical e Saúde Pública of the Universidade Federal de Goiás for the isolation and identification of etiological agents.
The subungual scraping material was treated with 20% KOH for 20 min and visualized under optical microscope for direct examination. It was seeded in sabouraud dextrose agar (SAD) plus chloramphenicol and selective agar for contaminating fungi and then incubated at room temperature for up to 30 days. Macroscopic observation of the obtained colonies was the first criterion used to distinguish between filamentous fungi and yeasts. Characteristics such as: Color, texture, surface, and diffusible pigment in the culture medium were analyzed. Microscopic structures, such as hyphae, conidia, yeast (morphology and disposition), and reproduction structures, were made with fragments of the colony between slide and cover slip and a drop of lactophenol cotton blue (Newprov®).
The colonies with yeast-like characteristics were identified according to Kurtzman, et al. [8] by the production of chlamydoconidia in Cornmeal agar (Difco®) plus tween 80, germ tube formation in fetal bovine serum, assimilation and fermentation of carbon sources, and colony staining in CHROMagar™ Candida medium. (Microbiology, France). Filamentous fungi, including dermatophytes and non-dermatophytic filamentous fungi (NDFF), were identified by macroscopy and microscopy of colonies and microculture on a slide when necessary. The criteria to confirm NDFF as and onychomycosis agents were clinically suspected characteristics of onychomycosis, visualization of fungal structures on direct mycological examination with 20% KOH, and growth in the culture medium of at least two samples acquired over a 15-day interval.
All data obtained from the questionnaires were keyed into an Excel spread sheet (Microsoft Excel 2007 software) and the resulting data were analyzed using SPSS for Windows version 20.0. A descriptive statistic was used, with absolute and relative frequencies defined for the studied variables. In addition, inferential statistics was performed using the Chi-square test with significance level of 5%.
Subungual samples were collected from 58 individuals. Onychomycosis diagnosis was confirmed by a positive direct and/or culture examination in 56.9% (33/58) of the samples. Of them, 63.6% (21/33) were from female subjects and 36.4% (12/33) were male. The participant ages ranged from 55 to 86 years (51.3 years ± SD = 32.8). Prevalence of positive results (42.5%) were found in individuals between 76-85 years old (Table 1). In this study, no statistically significant between age (p = 0.362) and sex (p = 0.234) associated of onychomycosis in institutionalized elderly.
Table 1: Demographic and clinical characteristics in institutionalized elderly with onychomycosis in Goiânia, Goiás, Brazil. View Table 1
Among the diagnosed onychomycosis, 87.9% (29/33) were observed in toenails and 12.1% (4/33) in fingernails, according severity of infection all of the cases were classified with mild damage. Regardless of the affected site, the most frequent clinical form was distal/lateral subungual onychomycosis, representing 63.7% of the cases. In 55% of the cases, the lesions had evolved for more than 5 years. In addition, 85% of the participants in the study had some chronic disease, with hypertension and diabetes mellitus the most frequent (Table 1).
According to mycological techniques, among the 33 subungual isolates, 54.6% were identified as yeasts, 21.3% were identified as dermatophytes, and 24.1% were identified as NDFF. The distribution of the identified species of onychomycosis is showed in Table 2.
Table 2: Etiologics agent distribution isolates from onychomycosis in institutionalized elderly in Goiânia, Goiás, Brazil. View Table 2
The applied questionnaire verified that for questions relating to "social" aspects, 94% of the individuals answered that other people notice the presence of the nail lesion. Among the questions in the "emotional" group, 96% stated that the presence of nail injuries influences their choice of shoes. In questions related to "clinical" manifestation, 98% perceive the difference in nail characteristics, such as thickness and discoloration, due to the clinical evolution of the lesions. All the answers from in the applied questionnaire are presented in Figure 1, Figure 2 and Figure 3.
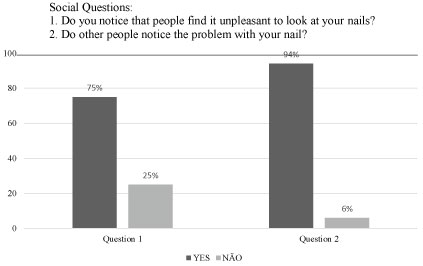 Figure 1: Distribution of the answers YES or NO of the questions related to the social group directed to institutionalized elderly with onychomycosis in Goiânia, Goiás, Brazil.
View Figure 1
Figure 1: Distribution of the answers YES or NO of the questions related to the social group directed to institutionalized elderly with onychomycosis in Goiânia, Goiás, Brazil.
View Figure 1
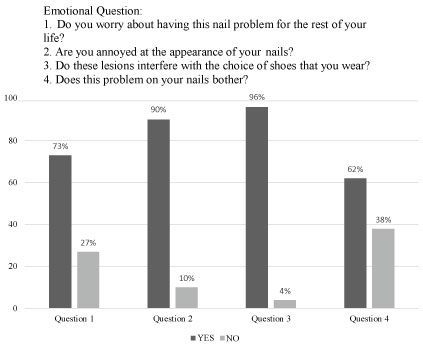 Figure 2: Distribution of the answers YES or NO of the questions related to the emotional group directed to institutionalized elderly with onychomycosis in Goiânia, Goiás, Brazil.
View Figure 2
Figure 2: Distribution of the answers YES or NO of the questions related to the emotional group directed to institutionalized elderly with onychomycosis in Goiânia, Goiás, Brazil.
View Figure 2
 Figure 3: Distribution of the answers YES or NO of the questions related to the clinical group directed to institutionalized elderly with onychomycosis in Goiânia, Goiás, Brazil.
View Figure 3
Figure 3: Distribution of the answers YES or NO of the questions related to the clinical group directed to institutionalized elderly with onychomycosis in Goiânia, Goiás, Brazil.
View Figure 3
Onychomycosis is a common dermatological problem, and the frequency varies according to the characteristics of the studied population and the environment to which they are exposed. The confirmed diagnosis of onychomycosis in 58.3% of the elderly patients attending at two gerontological complexes of Goiânia, Goiás corroborates other studies carried out in the same region. Souza, et al. [9] reported the frequency of onychomycosis in 56.4% of clinically suspected patients attended in a clinical laboratory, while Ataides, et al. [10] demonstrated 75% of confirmed cases in individuals at the dermatology center of a tertiary hospital.
Age is a factor that influences the frequency of this superficial infection. The frequency of onychomycosis increases according to the highest age group in different studies. It is estimated that approximately 40% of the elderly population has onychomycosis [2]. The present study verified the highest prevalence of onychomycosis in individuals between 76-85 years old due to reduced growth of the nail plate, which facilitates greater possibility of contact with fungi agents that cause this infection [11]. Orhan, et al. [12] reported the occurrence of onychomycosis in people over 40 years of age; Martínez-Herrera, et al. [13] observed similar results where the most affected age group was between 41-65 years, while Araceli, et al. [14] reported that the most affected age group was above 30 years and the number of cases increased in people 40 to 60-years-old.
In addition to the factors already mentioned, other conditions are related to the development of onychomycosis in the elderly. These conditions include immunological deficiency, chronic diseases such as diabetes and hypertension, reduced nail care due to the inability to take care of themselves, which is associated with ease of transmission in the home environment or among institutionalized individuals [11].
Our study found that female patients had greater frequency of onychomycosis [13-15]. The factors predisposing women to this superficial infection are greater contact with moisture in domestic service and recurrent traumas due to the use of closed-toe shoes in the beauty salon. Moreover, women are more likely seek medical attention when subungual lesions appear, which may influence the indices when comparing the frequency of fungal nail infections between men and women [16].
According to the results of the mycological analyzes, the direct examination (DE) with 20% KOH found a higher positivity than the growth of the fungus in culture medium. The difference in these results can be due to the uneven distribution of fungi in the lesions and difficulties in collecting the material. Direct examination also has limitations, such as nail keratinization that hinders microscopic observation and viability of fungal microorganisms. In addition, the service provided during the analysis of the DE with 20% KOH was important for a greater frequency of positive results than the growth of the culture, because the analyses was carrie d out in a center that specialized in the mycological diagnosis. The culture can be easily contaminated by environmental fungi and/or bacteria, preventing the growth of the pathogen, making the identification of the cause of onychomycosis more complicated [22].
The distribution of the etiological agents of onychomycosis indicated that yeasts of the genus Candida were dominant, as found in other studies [14,23,24]. Candida parapsilosis was the most common yeast agent of subungual infections in the studied individuals. The frequency of this isolate may be related to occupational factors of the studied population, such as domestic services, which are more predisposed to develop nail fungal infections due to high exposure to moisture, chemicals, and microtraumas [25-27]. Other yeast species, such as Trichosporon sp. were identified in this and other studies as onychomycosis agentes [9,10].
Among the filamentous fungi, Fusarium sp. was the most frequent agent of onychomycosis, representing in 26.7% of the positive samples. An acceptable justification for the occurrence of this species in onychomycosis is its ability to degrade keratin, due to the secretion of keratinases, producing lesions clinically similar to those caused by dermatophytes. Studies have found a varied frequency of this fungus in cases of onychomycosis. Escobar & Carmona-Fonseca [28] reported a frequency of 50%; Meireles, et al. [29] 18.6%; and Pontes, et al. [30] 33.3%. This varied presence of Fusarium sp. as an onychomycosis agent is because this environmental fungus has more capacity to infect the nails through contact with soil during framing and gardening, use of swimming pools, contact with domestic animals, and use of public showers [28,31-33]. The participants of the present study practiced gardening, landscaping, swimming classes, and group water aerobics, which may justify the presence of this NDFF in the studied population.
Dermatophytes are fungi with keratinolytic capacity and are commonly reported as etiologic agents of onychomycosis [9]. Dermatophytes were the third cause of onychomycosis characterized as T. rubrum and T. tonsurans species. In their study, Meireles, et al. [29] reported that dermatophytes were less frequent, as they only isolated one case of T. tonsurans and three of T. rubrum. However, Rocha, et al. [34] found the presence of dermatophytes in 66% of their samples with T. rubrum the most isolated species. Several cases report anthropophilic dermatophytes as the main etiological agents of onychomycosis, especially in areas with a tropical climate, of which T. rubrum and T. mentagrophytes are the main causes [34-36]. The encounter with anthropophilic fungi may be related to the greater ease of spreading in the crowded locations, since these fungi are well adapted to the keratinized tissue of the human host, which cause a chronic inflammatory process, and the transmission easily occurs between humans.
Several studies have found that onychomycosis, although not life-threatening, significantly changes the routine of its patients, and is not considered just an aesthetic problem. This mycosis has a strong impact on social relationships, with most participants reporting that people find it unpleasant to look at their nails and note the problem. These results support a study carried out by Szepietowski, et al. [4] who verified social problems more frequently, as reported in their study, and that the surveyed individuals were worried about the possibility of transmitting the infection to others. A pioneering study on quality of life in patients with onychomycosis found significant decrease in both the general mental health of the participants, social interaction, and a concern with physical appearance. In addition, they have a growing concern with their general health status and a greater sensation of generalized discomfort [37].
When questioned about emotional questions, these participants stated that they are uncomfortable with the appearance of the lesion and that it directly interferes with their choice of footwear. In clinical question, the participants also notice the change in the characteristics of their nails, difficulty in cutting and complaints of nail and finger/toe pain. The painful process in the nail plate due to the onychomycosis was reported in more than 50% of the patients questioned. This clinical characteristic is a factor that could be related to their inability to walk causing sedentary periods during their daily routine of individuals, such as the prac [37]. Questions about social, emotional, and clinical issues demonstrate the negative interference of onychomycosis in the routine tice of physical activities, leading to inferiority disorders and low self-esteem, as well as contributing significantly to the social isolation [38].
The morphological modifications of the nails are usually not specific for the different causes of nail disorders, but they are useful to suspect fungal involvement. The confirmatory mycological diagnosis is done by the identifying the genus and species; and this may also be directly related to the best therapies. Thus, this study demonstrated a higher frequency of onychomycosis in female participants 76-85 years old and that the most frequent clinical manifestation was distal lateral subungual onychomycosis, with more frequent toenail involvement.
Among the etiological agents identified, C. parapsilosis and Fusarium spp. were the main causes of onychomycosis. The isolates of anthropophilic dermatophytes, T. rubrum and T. tonsurans, may have greater ease in transmission among the studied population because they are institutionalized. Based on all data presented here on onychomycosis, more attention should be paid to the patients with this pathology, since it can interfere directly in their daily activities, in clinical, as well as social and psychological ways.