The relevance of the treatment of dementia will increase significantly in the coming years. Although studies show that exercise and music produces positive effects on motor function and cognition in people with dementia, the preferred treatment for dementia is medication. Therefore, research into non-pharmacological treatment is important. There are first indications that the combination of music and physical exercise positively influence cognitive and motor skills. Our aim was to examine the effects of music-based physical training with innovative devices in seniors with dementia and the acceptance of this exercise programms.
11 Participants (81.82 ± 4.51 years, 11 women) with dementia performed a dance intervention twice weekly for 60 minutes over 12 weeks and a music-based strength endurance intervention after an eight-week wash-out period. Participants executed a strength-endurance training (SET) using the Body-Spider® and a dance training (DT) by a Sports and Dance Walker. Information processing speed and memory performances (CERAD-NP), motor reaction (Drop bar test), grip strength (hand dynamometer), mobility (Chair-Rising Test) and Quality of life (NOSGERII) were tested. Music has been used to control for movement frequency and intensity.
After the respective 3-month interventions, some significant improvements in the selected cognitive and motor functions were observed. After the dance intervention, verbal fluency (p = 0.014), recognition recalls (discriminability) (p = 0.04), and processing speed (p = 0.02) enhanced significantly. After the music-based strength intervention, hand strength on the right (p = 0.043) and motor responsiveness (p = 0.03) improved significantly. Quality of life decreased slightly but was not significant.
Both dance-based (DT) and music-based strength-endurance training (SET) can stabilize and positively influence selected cognitive and motor skills in dementia patients. Mainly the stabilization of skills can be considered positive in dementia patients over such a period. Furthermore, the applicability of two music-based exercise programs could be demonstrated. In addition, the two exercise programs were shown to have different modes of action. A dance program influenced selected cognitive abilities, whereas a music-based strength endurance program stimulated selected motor abilities. The modes of action should be further investigated in subsequent studies.
Trial registration Number: DRKS00016651, 05.03.2019, retrospectively registered.
Dementia, Cognition, Motor skills, Music-based training
The increasing life expectancy of society means that more and more people are suffering from dementia and the number of people with dementia will tripled by 2050 [1]. The degradation process in dementia manifests itself particularly strongly in the loss of cognitive functions. This also results in deficits in functional daily living and basic motor skills [2], which causes loss of independence [3]. Therefore, people with dementia belong to the group of patients who need nursing and care. This, in turn, requires high statements from the health care system for care and support [4]. Dementia is a clinical syndrome with a number of different causes characterized by deterioration in not only cognitive, but also behavioral, social, and emotional attributes [5]. In progressed stages of dementia patients exhibit comprised motor deficits, like gait disorders and a higher risk of falls [6], which preclude them to participate in therapeutic offers and activities of daily life and causes tremendous consequences in the quality of life. Currently there is no pharmacological treatment with effectively proven benefit. The preferred treatment for dementia is medication. However, drug therapies for dementia are limited and are always associated with side effects [7]. Therefore, non-drug interventions are of high importance [7]. There are already some studies that show that various non-drug forms of intervention have a positive impact on people with dementia [8]. Promising therapeutic approaches in demented people seem to be music and physical activity. In music therapy, seven capacities of music have been proposed to be valuable: music is persuasive, engaging, emotional, personal, physical, social and affords synchronization [9]. It can address many symptoms of dementia, such as memory decline, decreased language fluency and altered sense of self [10]. Mostly musical functions, such as the emotional meaning of music, the detection of familiar songs and emotional responses to music such as joy are preserved in demented people, also in severe stages [11,12]. Non-musical functions such as autobiographical memory can be stimulated by music [12]. Gómez Gallego and Gómez Garcia showed significant improvements in memory, orientation, depression and anxiety in patients with mild and moderate dementia compared to inactive counterparts, when listening to music [13]. A meaningful function of music is highlighted by Brancatisano, et al. [10]. Music engages individuals in new learning in respect to exercise and cognitive training, because it evokes emotional and motor responses [14,15]. Blankevoort, et al. suggested that multicomponent interventions can improve physical functioning and basic activities of daily life in elderly demented subjects regardless of the stage of the disease [16]. Mathews, Clair and Kosloski (2001) observed an increased level of participation, when exercises were accompanied by rhythmic music in demented people [17]. The Mihama-Kiho Project Part II of Satoh, et al. combined physical training and music therapy [18]. They indicated that physical exercises in combination with music, resulted in greater positive effects on cognitive function and activities of daily life (ADL) in patients with mild to moderate dementia in comparison to cognitive stimulation without music [18]. In most physical exercise programs music is used as accompanying instrument during the training process. But studies have shown a greater effect in motor and emotional responses when motor performance has been synchronized to the music [19,20]. Dancing for instance, synchronizes the bodily movement according to music, fosters emotions and set demands on different motor skills and abilities and cognitive function [21,22]. Hence, it seems to be a promising intervention for demented patients. However, as the study situation is not uniform with regard to individual procedures and the results of studies do not have sufficient evidence, there is a need for further research in this regard [7]. Due to insufficient evidence and limited research in the area of combined physical training and music intervention, this study aims to investigate the effects of dance training and music-based strength-endurance training on cognitive and motor skills and quality of life in people with dementia. It also aimed to compare whether music-based strength endurance training or dance training can more effectively influence the selected motor and cognitive skills. To ensure a safety execution of dance-combinations, we used a self- designed constructed walker, called Sport and Dance Walker. Furthermore, to control for the movement quality of strength-endurance exercises we used a fitness-device called Body-Spider® (Co. Koopera), where participants exercise together in standing or seated position. As secondary outcome, we were interested if our specialized musical-guided physical training programs had an impact on training load parameters, compliance and overall acceptance by demented people.
An Intervention study in a pre- post-test design has been chosen, which was split into two phases: Intervention phase I = Dance Training (DT) and Intervention phase II = Strength-Endurance Training (SET) (Figure 1). Eleven dementia patients (81.82 ± 4.51 years) participated in the intervention study. The demented patients, selected by the cooperating care station (VITANAS in Magdeburg, Germany) attend both intervention phases, each lasting twice a week, 60 minutes for 12 weeks. Before each intervention started, pre-test data was collected. The post-test assessments were conducted before the wash-out period (eight weeks inactivity) and after intervention phase II. The wash-out phase served to ensure that any training effect from the first intervention did not influence the impact of the second intervention. All participants have been hospitalized for more than one year and have had different forms of the disease. The Mini-Mental-State Examination was used to determine the severity of dementia. The results showed that one subject had mild dementia and nine had moderate dementia and one subject had severe dementia. Participants had to be physically and cognitively able to perform an exercise program and follow the instructions of the exercise instructor.
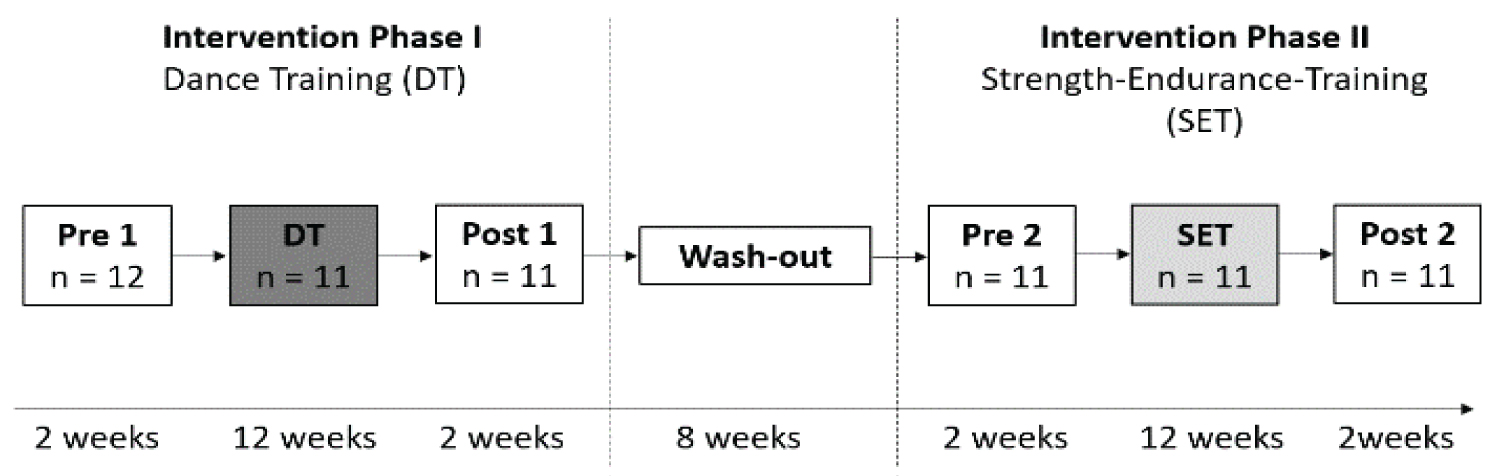 Figure 1: Study design.
View Figure 1
Figure 1: Study design.
View Figure 1
In addition, they had to be able to move around independently or with a walker and had to have no severe cardiovascular diseases or cardiac arrhythmias. Anthropometric data were collected utilizing a questionnaire. A detailed sample characterization can be found in electronic Supplement 1 (Sample charactertic).
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of University Magdeburg (No. 193/18). Written informed consent was also obtained from each participant or legal representative for participation in the study (Figure 1).
Twelve participants have been assigned into two groups of six persons to ensure the best support in both programs. A fixed instructor was appointed as expert for the DT and SET and got supported by research assistants. Both training programs were carried out in their familiar surrounding (VITANAS). The music was chosen according to the preferences of the seniors. Special characteristics of music like the articulation, melody and dynamic have been considered in the choice of music. Time components of the music like beat per minute (bpm) were considered to control the movement intensity and frequency. Both programs were structured into three parts: A ten-minute warm-up, a 40-minute main part (dance routines/strength-endurance exercises), a five-minute cool down. At the beginning and end of each unit participants were provided with the same music songs to create a ritual and a recognition factor for the participants.
Intervention phase-I dance training (DT): The DT was divided into three units, each lasting four weeks. The intensity of movement execution has been increased by increasing the bpm from unit one (100 bpm) to unit two (110 bpm) to unit three (120 bpm). Additionally, the taught dance routines in each of the three units have been increased, by increasing the number of steps. To ensure a safe execution of dance steps, all participants received a device-Dance and Sport Walker, which was individually adjusted to the user (Figure 2a). The Dance and Sport Walker was constructed for the special needs of person who have motor impairments [23]. For a better stability, but also barrier-free movement in all directions the user is located inside the Walker. With this walker, participants were able to execute common dance patterns in space (forwards, backwards, sideways, turns, chassée) in a regular dynamic way to music. After a ten-minute warm-up, both standing and sitting, the main part began with the Dance and Sport Walker, teaching dance steps (e.g. turns, chassée). The main part lasted about 40 minutes. After this, a cool-down phase with stretching and relaxation exercises was carried out.
 Figure 2: Intervention Devices ((a) Sports and Dance Walker/ (b) Body-Spider).
View Figure 2
Figure 2: Intervention Devices ((a) Sports and Dance Walker/ (b) Body-Spider).
View Figure 2
Intervention phase II-strength-endurance training (SET): The SET was executed on a multifunctional fitness station called Body Spider® (Co. Koopera). It focused on strengthening the upper and lower extremities in a fixed sequence and rhythm with the existing rope pulls for arms and legs, as shown on Figure 2b. As part of the intervention, muscle groups should be trained that are necessary for maintaining and securing everyday movements (e.g. leg muscles, back muscles). There are drawstrings in two different thicknesses, light and heavy ones. The participants were placed on fixed places according to their abilities. Training sessions took place while sitting or in standing positions with two intensity levels over the time of three months. Music has been applied to control and adjust training intensity and frequency. During the first unit (four weeks) music consisting of 110 bpm to 120 bpm has been chosen and participants executed a whole-body training. The number of bpm has been increased from 120 bpm to 165 bpm to increase the movement frequency during the second unit (week five to twelve). To increase the intensity, music was selected with 64 bpm to 100 bpm to foster slower, but more intense movements. The second unit was only focusing on the upper body strengthening (Arms and upper torso) or consisted only of lower body training (Legs and lower torso). Each session was basically designed similarly to dance training. In the beginning, there was an approximately ten-minute warm-up in a seated position for mental and physiological activation. The program then began on the body spider, which constituted the main part. Each of the movement units comprised six exercises, with each exercise performed for three times 45 seconds. The break was one minute between sets and three minutes between each exercise. At the end of each unit, there was a ten-minute cool-down for stretching and relaxation (Figure 2).
Cognitive and motor tests as well as a questionnaire for quality of life have been selected to determine the level of performance before and after the interventions and will be explained briefly in the next subsections. Within the interventions, a narrative log was created to record the feasibility of the exercises. A detailed description of the test procedures can be found in electronic Supplement 2 (Test Procedure).
Cognitive test-consortium to establish a registry for alzheimer's disease (cerad np plus): The CERAD NP Plus is a test battery by Morris, Mohs, Rogers, Fillenbaum and Heyman (1988) containing eleven tests to cover central cognitive areas like orientation, memory, attention, numeracy and language skills [24]. Due to reasons of organization, eight tests have been selected for this investigation to assess executive function (verbal fluency task), general cognitive functioning (mini mental-status), verbal memory (immediate and delayed word list learning task), visuo-constructive abilities (immediate and delayed constructional praxis task) and visuomotor processing speed (Trail-Making-Test A).
Motor tests: Three motor tests have been implemented into this study to assess motor reaction time, grip strength and mobility. To determine the reaction time, the drop bar test by Fetz and Kornexl (1978) has been used [25]. Participants have to grasp a falling bar with the dominant hand. The second measurement is called hand dynamometer tests by Richards and Palmiter-Thomas (1996) and records grip strength in Newton in both hands [26]. The test enables a statement to be made about the current muscle strength [27]. The Chair Rising Test by McCarty (1985) evaluates strength and coordination of the leg muscles [28].
Questionnaire for quality of life (QoL): The quality of life status was screened using NOSGER II by Brunner and Spiegel (1990) [29]. This questionnaire consists of six dimensions: Memory, instrumental Activities of Daily Life, personal hygienics, mood, social and disruptive behavior and is completed by the nursing staff. High values are to be interpreted as clear disturbances in the behavioral areas concerned.
Statistical data analysis was performed in SPSS, version 25 (IBM). All quantitative variables were reported as mean ± SD (standard deviation). At the beginning of the statistical analysis, a one-way MANOVA was performed. If this revealed a significant difference, individual ANOVAs were performed with post-hoc analyses. It was also performed in the case of a violation of the normal distribution since the analysis of variance is robust to the violation of the normal distribution [30]. In case of a significant difference, post hoc analyses were performed with a Dunn-Bonfeneroni correction. The classification, according to Cohen [31], was used to assess the effect size.
All results (mean value, standard deviation and p-value) for cognitive and motor performances as well as quality of life are displayed in Table 1. Again, the same subjects exercised a DT (Intervention Phase I) and after an eight week of rest (wash-out phase) a SET (Intervention Phase II). Since the focus was on the individual forms of intervention, the significant values of the pre-post comparison of each intervention were indicated in Table 1. In the baseline (pre-test 1-pre-test 2), the values do not differ significantly. Thus, it can be assumed that the wash-out phase was long enough and that the effects of the first intervention had no influence on the second intervention.
Table 1: Mean value and Standard Deviation of cognitive and motor performances in pre- and posttests for Dance Training (DT) and for Strength-endurance Training (SET) and quality of life (QoL). View Table 1
For verbal fluency task, significant alterations have been found after the Dance Training (p = 0.014). No significant change in verbal fluency was observed after the strength endurance training. The performance of the MMSE did not change significantly after both the dance program and the strength endurance program (p = 0.87) but remained stable. Verbal memory has been tested using a word list, consisting of 10 words, which were presented three times. Regarding the sum of immediate recall of three-word lists, no significant results were found after both the dance program and the strength endurance interval. After a brief filled interval (5 to 8 minutes), subjects had to recall the words. Here, too, no significant results could be found after the respective interventions. The recognition recalls were composed of the yes-no identification of the 10-word list items interspersed with ten distractor items (discriminability). The results showed that subjects improved significantly with a medium effect after the dance program (p = 0.04). No significant effects could be shown after the strength endurance program.
The constructional praxis task tested the visuo-constructive abilities. First, subjects had to copy four geometrical figures. In mean they achieved six points out of 11 points to each time-point of measure. There were no significant differences in the program. Similar results were found after recall performance. The TMT-A data revealed significant differences by dance program. Here, a significant improvement (p = 0.02) with a medium effect was found. After the strength endurance program, no significant results could be determined.
The Chair-Rising Test assesses muscle strength of the lower extremities. The time was measured for a five-time chair rise. In general, the level of performance was low within all timepoints of measurement. No significant differences could be determined after the interventions.
Performance of the drop bar test for simple motor response showed a significant difference after the strength endurance intervention (p = 0.033). The significant effect occurs with a medium effect. A descriptive improvement was also found after the dance intervention, but it was not significant.
Grip strength was determined for both hands using a hand dynamometer. Here, after the strength endurance intervention, a significant improvement with a medium effect in the hand dynamometer test on the right could be shown (p = 0.03). The hand dynamometer test on the left after the strength endurance intervention and the hand dynamometer tests on the left and right after the dance intervention showed improvements, but these were not significant.
The quality of life was examined using the NOSGER II. High values indicate a low quality of life. The maximum score is 150 points, expressing a very poor quality of life. The score of the subjects has been rated on medium range of the scale. No significant differences were found after the interventions.
Although no quantitative measure has been included to evaluate the trainings load, based on the narrative log, it was observable that the number of recreational breaks reduced within the training sessions. In the first month of dance training subjects needed to make a break every seven minutes. In the last month of training, the 60-minute intervention could be completed without any breaks. The situation was similar for the strength endurance intervention. Here, the subjects had to take more breaks during the exercises initially than at the end of the intervention. Furthermore, it was observed in the strength endurance program that the execution of the movements deteriorated with music with singing, since the test subjects concentrated more on the music than on the movement. Besides, the observation protocol showed that the exercises were easy to perform and the test subjects always looked forward to the sport and had fun during the sessions. This is also shown by the frequency of the test subjects attendance. On average, the test subjects were present for 94 percent of the exercise sessions.
Receptivity to music can be maintained even in very late stages of dementia and can evoke essential functions to slow down the progression of the severe disease. The combination of music and physical activity positively affects cognitive and motor functions in patients with dementia. Therefore, the pilot study aimed to investigate whether music-based training focusing on strength-Endurance and dance affects motor and cognitive abilities in seniors affected by dementia. Music was used to synchronize body movements to music, control movement frequency, and intensity, motivate, persuade, and engage participants in physical activity. Results showed that cognitive performance (visual-constructive skills, memory) remained stable after each intervention, except verbal fluency, recall, and scores on the Trail-Making Test. Significant improvement was observed in them after the dance program. This is consistent with the findings of Brancatisano, Baired & Thompson (2019), who tested a "music, mind, and movement" intervention in ten subjects with mild to moderate dementia [10]. They showed significant improvements in verbal fluency in their intervention group. Van de Winckel, et al. (2004) found significant improvements in performance on the MMSE and on a fluency task in a group of 15 demented subjects who received music-assisted movement training [32]. The intervention group exercised 30 minutes daily for three months. No significant improvement in cognition was seen after the strength endurance intervention. The vital component for the improvement, especially after the dance intervention in this study, was the combination of music and exercise, but the underlying mechanism concerning our results remains unclear. It can be hypothesized that music increases arousal and, in combination with exercise, improves processing speed and verbal fluency, especially during dancing.
An increase in arousal could also be the explanation for the improved motor response in the drop bar test. A significant improvement was found after the SET with a mean effect size (f = 0.3). Participants also showed a faster response after DT, but this result was not significant. This could be due to the fact that dancing in the sport and dance walker does not involve arm movements. The arms are fixed firmly on the armrest. In the SET, the whole body was involved by pulling the rubber cords and performing various movements for the upper body. Another motor performance, grip strength, increased after both forms of intervention, suggesting that physical activity generally leads to better muscle strength. However, significant improvements were only found in the hand dynamometer test on the right after the strength endurance interval. That grip strength improves after physical activity is consistent with other studies, such as Chen, et al. (2016), who measured handgrip strength in older adults with cognitive impairment (MMSE 11.41 + 4.32 points) after elastic band training (three times per week, 40 minutes for six months) [33]. They found significant improvements, but the effect size was small (d = 0.13). The effect size of our study showed a medium effect (f = 0.4). The fact that only the right-hand strength improved significantly after the strength endurance program may be due to the small number of subjects. Overall, the subjects improved by about 25 N after the interventions here; we can speak of clinical relevance, which, however, was not significant. Further studies would have to be conducted on this.
Blankevoort, et al. (2010) demonstrated that lower limb strength improved equally with a multicomponent intervention and progressive resistance training [16]. They concluded that the best results were obtained in interventions with the largest training volume. In our study, overall lower limb strength (chair-rising test) remained stable after both forms of intervention, which could be due to low training volume. Long, et al. (2019) noted that the quality of evidence for strength was low [34]. There was no conclusive evidence regarding the effect on strength in people with moderate to severe dementia.
According to the results, quality of life did not change within the study period, which is consistent with a systematic review by Ojagbemi & Ojagbemi (2017), which concluded that the positive effects of exercise on quality of life are minor. Most results suggest small to non-significant improvements [35]. Quality of life (QoL) in patients with dementia is a complex phenomenon to measure. It is still unclear whether it is best to measure QoL in this population according to the judgment of a representative (caregiver) or according to the person whose QoL is determined [36]. It is known that proxy ratings of patients' QoL are influenced by the rater's level of distress or state of emotional well-being [37].
Although we found only sporadic effects following our music-based intervention, we would like to highlight that participants could reduce the number of recovery breaks within training periods, which could be due to the motivational, engaging, and persuasive nature of the music. However, this study suffered from some limitations. It should be noted that the actual effects of music were not considered separately. Focusing once again on the study by Gómez Gallego and Gómez Garcia (2017), music is perceived very individually and can have adverse effects on the individual with dementia if it is interpreted in a disruptive manner [13]. Cevasco & Grant (2003) compared responses to vocal versus instrumental music during exercise [38]. They showed that participation in exercises to instrumental music was significantly greater than exercises to vocal music. Thus, the type of music certainly seems to have an advantage over exercise tasks' outcome [39-41]. Other limitations of this pilot study are the small sample size and a lack of a control group. A more specific classification of dementia types in a randomized controlled trial could provide more accurate information. To ensure external validity, it is recommended that a larger participant group with appropriate gender distribution, disease severity, and performance homogeneity be conducted in the future. Additionally, training intensity should be adjusted [16]. Likewise, clinical relevance should be considered in upcoming studies in addition to statistical significances [42]. Since clinically, these give more information about the influence of a training program. These adjustments need to be considered in further studies.
Music-based exercise programs could represent a future non-pharmaceutical treatment or accompany drug therapy for dementia patients. It was shown that training in small groups with at least one permanently employed, the trained trainer makes sense. The use of innovative exercise equipment such as the Body-Spider® and the self-developed and patented Sports and Dance Walker has proven effective against the progression of dementia. Seniors with dementia have embraced both pieces of equipment. A 3-month music-based strength-endurance training and dance training program has shown that motor and cognitive skills tested did not deteriorate compared to studies without training [43]. Additionally, dance training and music-based strength endurance training have been shown to have different effects on dementia patients. Thus, dance training could influence the selected cognitive abilities, whereas music-based strength endurance training positively influenced motor abilities. It can be concluded that a combination of both forms of intervention may work more efficiently. This should be investigated in subsequent studies. In addition, an adaptation of the intensity and intervals of the training would be conceivable, taking into account current international guidelines [44].
The authors would like to thank the participating partner VITANAS.
No funding was received for conducting this study.
The authors declare that they have no competing interests.
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of University Magdeburg (No. 193/18).
Informed consent was obtained from all individual participants included in the study.
All authors agree with the publication process.
Yes, the datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Yes.
A.P, K.R., K.W., and A.H. conceived and planned the study and experiments. A.P, C.L took the lead for intervention and M.P. was included in pre/post- testing, A.P., C.L., K.R. derived the models and analyzed the data. C.L., A.P, K.R., K.W., A.H., M.P. contributed to the interpretation of the results. A.P., C.L., K.R. took the lead in writing the manuscript.