Background: Nephrotic syndrome is defined as proteinuria 3 grams or more in 24 hours or urine protein/creatinine ratio greater than 2, usually with associated hypoalbuminemia. Diabetes Mellitus is known to cause diabetic nephropathy.
Case presentation: A patient in his 70s with history of chronic myelogenous leukemia, hypertension, type 2 Diabetes Mellitus, hyperlipidemia, and recent Coronavirus-19 (COVID-19), presents for 1 week of difficulty urinating. In addition, he has been having significant testicular swelling, bilateral lower extremity swelling, and mild shortness of breath. On exam, patient had bibasilar crackles and decreased breath sounds, and 3+ bilateral edema to the mid-thighs. Patient was noted to be euvolemic on his exam two weeks prior. Serum albumin was 2.2 g/dL and Urine protein/creatine ratio was 4.2, consistent with nephrotic syndrome. He also had an acute kidney injury with a creatinine of 1.77 mg/dL (1.13 two weeks prior). Hemoglobin A1C was 9.6. Surgical pathology from a kidney biopsy showed advanced diffuse nodular diabetic glomerulosclerosis, and global glomerulosclerosis. Electron microscopy showed segmental effacement of foot processes. Echocardiography showed an ejection fraction of 67%. Vascular duplex showed no deep venous thrombosis. He was treated with intravenous diuresis, albumin infusions, and diabetes management.
Conclusions: Nephrotic syndrome from advanced diabetic nephropathy may present initially in an elderly individual following COVID-19 insult. Patients may present with massive volume overload and acute kidney injury, even if not present two weeks prior. Diuretics are effective in treating volume overload. Diabetes education and management are essential to prevent further kidney damage.
COVID-19, Nephrotic syndrome, Diabetes mellitus, Diuresis
COVID-19: Coronavirus 19 Virus; CKD: Chronic Kidney Disease; SGLT2i: Sodium-Glucose Co-transporter 2 inhibitors; LDL: Low Density Lipoprotein; CML: Chronic Myelogenous Leukemia
Nephrotic syndrome is defined as proteinuria 3 grams or more in 24 hours or urine protein/creatinine ratio greater than 2, usually with associated hypoalbuminemia. Nephrotic syndrome can affect children and adults, though typically does not present initially in an elderly patient. Diabetes Mellitus is known to cause diabetic nephropathy, especially among those with uncontrolled blood sugars. However, a new presentation of nephrotic syndrome in an older patient is uncommon, especially after 25 years of diabetic disease. This case highlights the importance of diabetes education and medication compliance due to renal and extra renal consequences that may result when diabetes is left unchecked.
A patient in his 70s with history of chronic myelogenous leukemia on Imatinib (since 2006 with no complication), hypertension, type 2 Diabetes Mellitus (for over 25 years with no documented retinopathy or neuropathy), hyperlipidemia, recent Coronavirus-19 (COVID-19), Bell’s palsy, presents for 1 week of difficulty urinating. He states he is only dribbling urine and his last normal urination was about 1 week ago. He also has been having constipation for over one week. Patient denied recent non-steroidal anti-inflammatory drug (NSAID) use. In addition, over the past few days, he has been having significant testicular swelling, bilateral lower leg swelling and bilateral upper extremity swelling, with mild shortness of breath. On admission, patient was a febrile, not tachycardic, saturating well on room air, but hypertensive to a blood pressure of 154/77 mmHg. On exam, patient had crackles and decreased breath sounds over bilateral bases, and 3+ pitting edema up to the mid-thighs. Patient was noted to be euvolemic on his exam two weeks prior by multiple providers, and this was his first presentation of volume overload. On further investigation, patient was unsure of his diabetes medications at home, and may have not been taking them as prescribed.
Urinalysis showed 10 Red Blood Cells/high power field (hpf), 2 white blood cells/hpf, and 300 mg/dL of protein. Serum albumin was 2.2 g/dL and Urine protein/creatine ratio was 4.2, consistent with a diagnosis of nephrotic syndrome. Serum albumin two weeks prior was 2.8 with no documented proteinuria. In addition, liver enzymes were within normal limits. Complete Blood count on admission was remarkable for anemia with hemoglobin of 9.5 g/dL (baseline 10.3). Lipid panel showed Total cholesterol of 162 mg/dL, Triglycerides of 123 mg/dL, High-density Lipoprotein (HDL) of 66 mg/dL, non-HDL cholesterol of 132 mg/dL, and Low Density Lipoprotein (LDL) of 116 mg/dL. Patient did have an acute kidney injury with a creatinine of 1.77 mg/dL, whereas two weeks prior it was 1.13 mg/dL. These laboratory findings were not present two weeks prior (Table 1). Extensive workup including Antinuclear antibody (ANA), p-antineutrophil cytoplasmic antibodies (p-ANCA), c-ANCA, anti-Glomerular Basement Membrane (anti-GBM), hepatitis panel, Human Immunodeficiency Virus (HIV), C3, C4, Parvovirus IgM, Serum protein electrophoresis, immunofixation, kappa/lambda, Bence Jones protein, and Phospholipase A2-Receptor antibody (PLA2-R) were all negative. Hemoglobin A1C was 9.6, and glucose range was 120-274 mg/dL. Surgical pathology from a kidney biopsy under light microscopy showed advanced diffuse nodular diabetic glomerulosclerosis, global glomerulosclerosis (26% of glomeruli), moderate tubular atrophy and interstitial fibrosis (30% of sampled cortex), severe arterial and hyaline arteriolar sclerosis, 1+ mesangial IgA deposition, no active interstitial inflammation, and micro-aneurysmal glomeruli changes suggestive of superimposed glomerular endothelial cell injury. Electron microscopy showed glomerular visceral epithelial cells with segmental effacement of their foot processes, irregular thickening of the glomerular basement membrane, endothelial cells with no capillary wall dense deposits, and mesangial matrix nodular expansion, with irregular densities, deposition of cellular debris, and rare small dense deposits. Echocardiography showed a normal ejection fraction of 67% with normal left and right ventricular function. Vascular duplex ultrasound of both lower extremities and upper extremities showed no evidence of deep venous thrombosis. CT chest showed moderate Right pleural effusion and small left pleural effusion (Figure 1). CT abdomen showed no hydronephrosis or nephrolithiasis (Figure 2), but did demonstrate as cites, anasarca and scrotal edema.
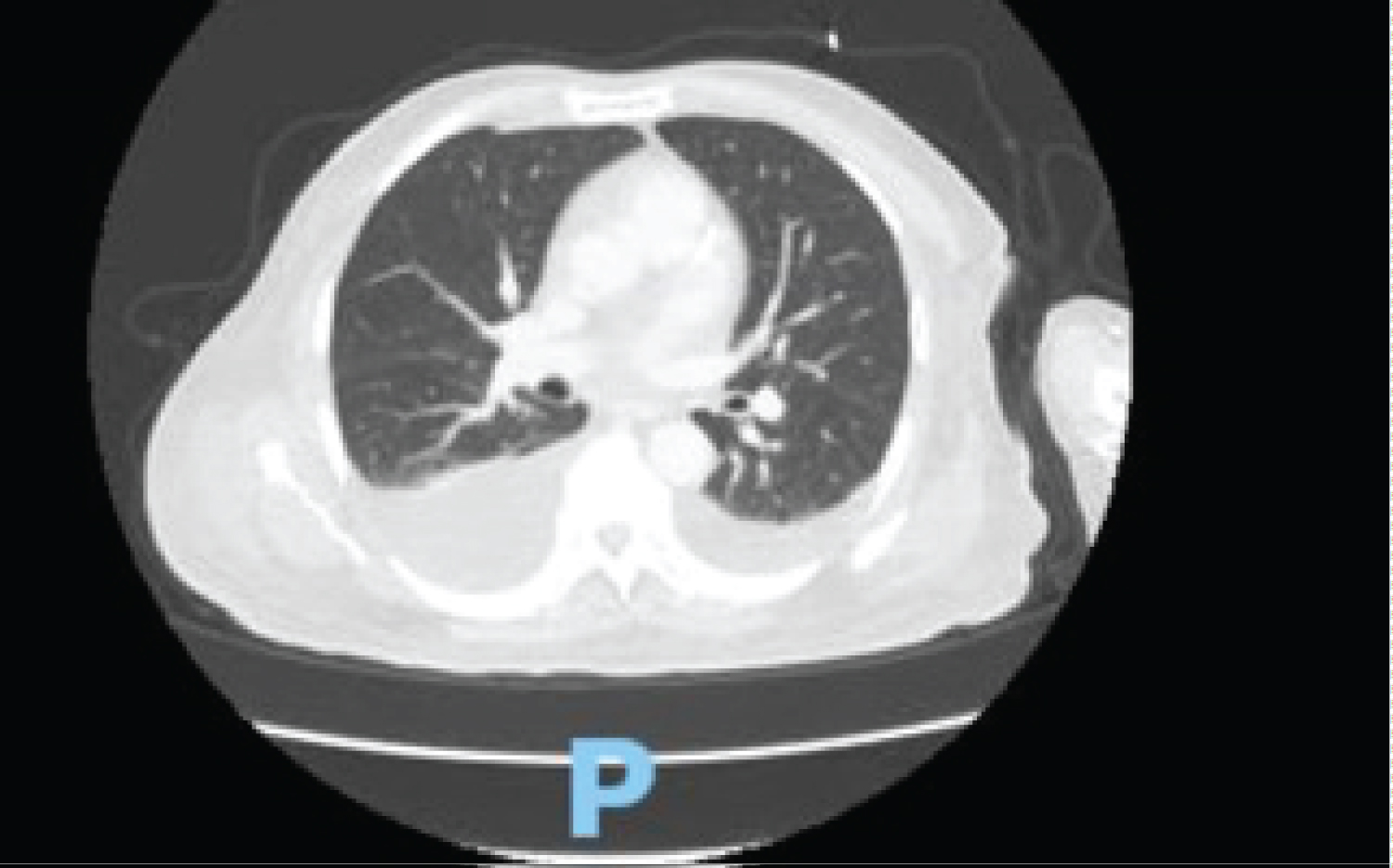 Figure 1: Computer Tomography (CT) Scan of the Chest showing a Moderate Right pleural effusion and a small left pleural effusion.
View Figure 1
Figure 1: Computer Tomography (CT) Scan of the Chest showing a Moderate Right pleural effusion and a small left pleural effusion.
View Figure 1
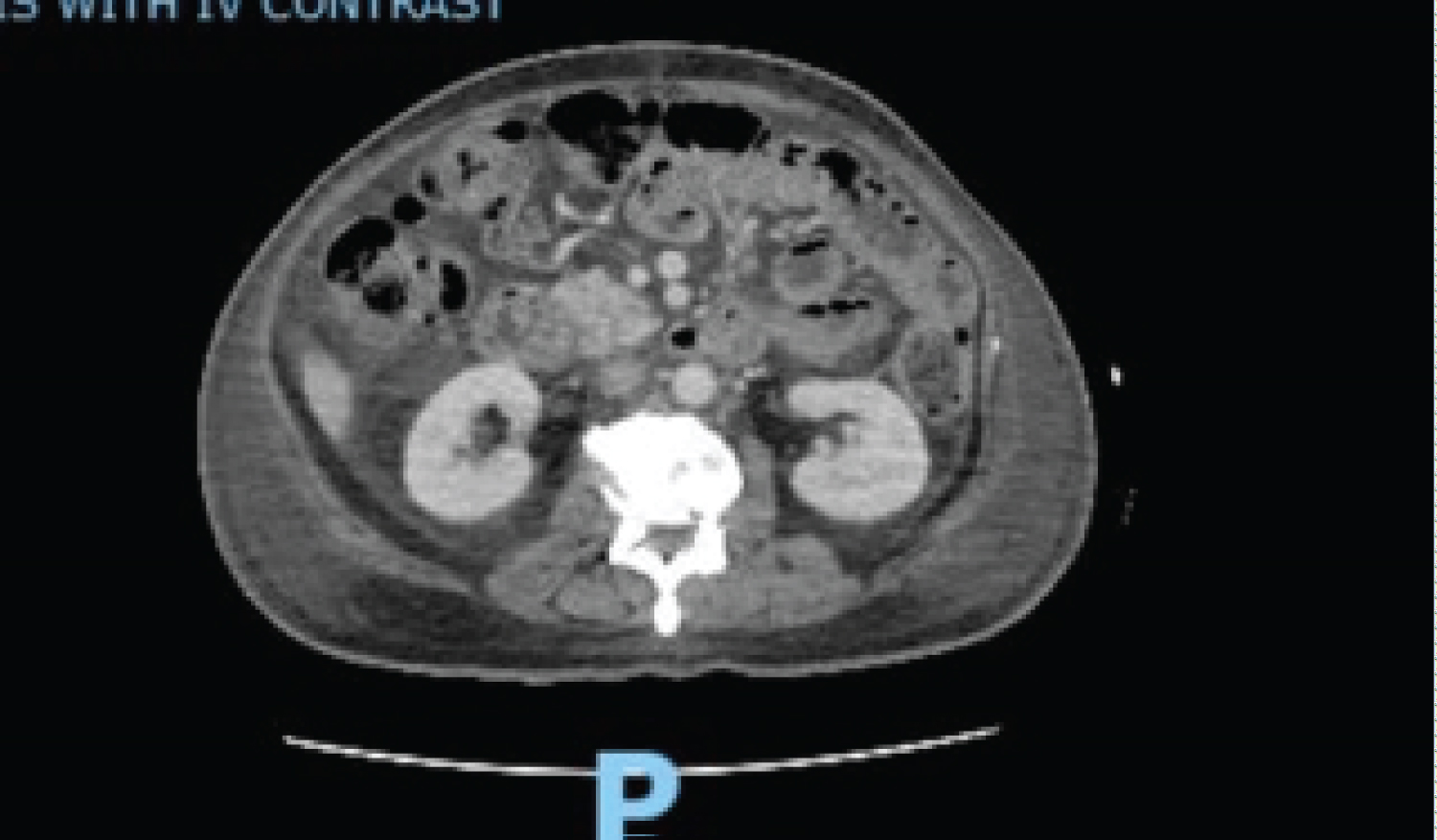 Figure 2: CT scan of abdomen and pelvis showing no hydronephrosis or nephrolithiasis.
View Figure 2
Figure 2: CT scan of abdomen and pelvis showing no hydronephrosis or nephrolithiasis.
View Figure 2
Table 1: Showing lab and exam findings of our patient on admission and two weeks prior. View Table 1
Given the above findings, and surgical pathology results, the most likely diagnosis was nephrotic syndrome presenting in an elderly individual secondary to advanced diabetic glomerulosclerosis following a recent COVID-19 infection.
Although there are case reports stating edema secondary to Imatinib usage, our patient was on Gleevec for CML since 2006, with no complication or reported documentation of an edematous state. It is unlikely that this sudden volume overload would be from a medication that he was on for so long without complication. His private oncologist confirmed that these pleural effusions and peripheral edema are new and is most likely from his diabetic nephropathy. His oncologist stated that is unlikely to be due from his Imatinib usage which he has had for over 16 years without any problem.
Our patient had diabetes for over 25 years (without documented neuropathy or retinopathy), though this was largely uncontrolled. This case is unusual in that the diabetic nephropathy presented after 25 years of having diabetes in the absence of retinopathy or peripheral neuropathy.
In addition, the patient’s Echo showed a normal ejection fraction suggesting that the volume overload is not cardiac related. In addition, the duplex of the upper and lower extremities were negative for deep venous thrombosis as the source of the peripheral edema.
Our patient was given a water enema after which he had a large bowel movement. Our patient was also treated with diuresis with intravenous Lasix 40 every day. He was also on heparin subcutaneous injections for deep venous thrombosis prophylaxis while inpatient. In addition, he received albumin infusions. Finally, his diabetes was managed with a basal-bolus insulin regimen.
Patient was discharged on a Sodium-Glucose Cotransporter -2 inhibitor, Metformin, Januvia, Imatinib, as well as Lasix 40 orally daily. Patient was also instructed on having a high-protein, low-salt diet. Patient was given follow up with nephrology, oncology, pulmonology, podiatry, and ophthalmology.
Nephrotic syndrome is defined as massive proteinuria 3 grams or more in 24 hours or urine protein/creatinine ratio greater than 2, usually in the presence of hypoalbuminemia [1]. Although hematuria is not usually found in cases of diabetic nephropathy, it may be present on urinalysis. In fact, in a study of 30 patients with diabetic nephropathy, hematuria was found in 30% of cases, and red cell casts in 13% [2].
Children with nephrotic syndrome usually present with facial edema, while adults present with dependent edema. However, the extensive edema observed in our patient with quadrilateral extremity edema, scrotal edema, and bibasilar crackles is unique.
Nephrotic syndrome is caused by increased permeability through a damaged basement membrane allowing the loss of albumin and proteins in the urine. There are two primary hypotheses regarding the development of edema typically seen in nephrotic syndrome. In the under fill hypothesis, the loss of albumin in the urine leads to reduced plasma oncotic pressure resulting in edema as the capillary hydrostatic pressure exceeds the intravascular oncotic pressure. This in turn leads to decreased plasma volume leading to increased sodium and water retention [3]. In the overfill hypothesis, there is an intrinsic defect in the renal tubules to excrete sodium secondary to intraluminal protein, leading to increased sodium and water retention [4].
Type 2 Diabetes is a common secondary cause of nephrotic syndrome. In fact, diabetic nephropathy is the leading cause of end-stage renal disease worldwide. However, it is unusual for diabetic nephropathy to be the initial presentation of diabetic complication without prior documented retinopathy or neuropathy as our case.
Given the significant morbidity and mortality associated with diabetic nephropathy, screening is essential. In patients with type 2 diabetes, screening for microalbuminuria should be performed at time of diagnosis and yearly afterwards [5].
In addition, nephrotic syndrome does not usually present as the initial presentation of diabetic complication in an older adult. This makes our case unique in that the volume overload, severe albuminuria, proteinuria, and acute kidney injury presented at once and was not present two weeks prior, even though the patient had longstanding history of diabetes for over 25 years.
Our patient was found to have diabetic glomerulosclerosis on kidney biopsy. Classification for diabetic nephropathy was proposed by Tervaert, et al. [6] Class I is defined as glomerular basement membrane thickening and only mild, nonspecific changes on light microscopy. Class II is defined as mesangial expansion but without nodular sclerosis or global glomerulosclerosis in more than 50% of glomeruli. Class III is defined as nodular sclerosis (Kimmelstiel-Wilson nodule). Class IV is defined as advanced diabetic glomerulosclerosis with more than 50% global glomerulosclerosis, and other clinical or pathological evidence of diabetic nephropathy. By this definition, our patient most likely had Class III diabetic nephropathy [6].
To treat diabetic nephropathy, we attempt to address multiple conditions. We first aim to treat diabetes with a goal A1C less than 7.0 and hypertension with a goal blood pressure goal less than 130/80 mmHg. We also try to use an Angiotensin-Converting Enzyme inhibitors especially in diabetics with microalbuminuria and treat Dyslipidemia with an LDL goal less than 100 mg/dL [5]. In addition, sodium-glucose Co-transporter 2 inhibitors (SGLT2i) have been associated with reduced all-cause mortality in patients with diabetes, especially among those with cardiovascular disease [7].
Treatment for nephrotic syndrome more broadly typically begins with treating the underlying cause. Minimal change nephropathy typically responds well to steroids [1]. Lupus nephropathy typically responds to steroids in combination with cellcept or cyclophosphamide [1]. Diuretics such as Lasix may be needed to decrease edema, as our case did. In patients with diabetes, Angiotensin Converting Enzyme inhibitors or Angiotensin Receptor blockers may be useful in reducing proteinuria [8]. A diet rich in protein and low in salt is also recommended. Steroids are often used in the treatment of nephrotic syndrome, though the evidence is not as convincing [8].
Treating and managing diabetes is quite essential to prevent progression and complications. In our patient, he stated not being compliant on his home regimen because of a lack of proper education and a fear of seeing his blood after a finger stick. Having diabetes without proper management puts patients at great risk for the fast development of complications.
Interestingly, in the DISCOVER 3-year prospective study of 7843 patients from 35 countries with type 2 diabetes, a substantial proportion of patients developed CKD or had CKD progression following the initiation of second-line therapy [9]. Therefore, treating diabetes with first line agents and ensuring adequate glucose and A1C control is essential to preventing diabetes complications or at least slowing down their development.
Therefore, prompt diagnosis and management of patients with diabetic nephropathy is essential.
Nephrotic syndrome from advanced diabetic nephropathy may present initially in an elderly individual following COVID-19 insult. Nephrotic syndrome may present with significant volume overload including diffuse anasarca, scrotal swelling, quadrilateral extremity swelling and pitting edema, ascites, and bilateral pleural effusions, even if no edema was present two weeks prior. Diuretics are effective in treating volume overload, but high doses may be needed in the long-term management of nephrotic syndrome. Diabetic nephropathy may be the initial presentation of diabetic complication even if no prior history of retinopathy or neuropathy is documented, and may indicate need for stricter glycemic control and education. Diabetes education and management are essential to prevent complications including irreversible kidney damage. Given the high prevalence of diabetes, management of diabetic nephropathy in earlier stages is preferred to prevent advanced disease. Furthermore, COVID-19 is an important trigger and can precipitate nephrotic syndrome in susceptible individuals, highlighting the need for COVID vaccination and preventative measures.
The following case report did not require ethics approval. Consent to participate was obtained from the patient.
Written Informed consent was obtained from the patient included in this report, including permission for publication of data and clinical images.
All data generated or analyzed during this study are included in this published article [and its supplementary information files].
The authors declare that they have no competing interests.
There were no sources of financial support for this case report from government or industry.
JJ was responsible for the writing of the report, data acquisition, and analyzation of data included in this report. All authors read and approved the manuscript prior to submission.
All individuals that contributed to this publication are listed in the author’s section. The organization where this research took place is North Shore University Hospital. There were no grants or sources of funding used in the production of this manuscript. There are no other significant contributions to report.