Background: Deconditioning of the core muscles, including the abdominal and pelvic floor muscles (PFM), increases the predisposition to injury, incontinence, and sexual dysfunction and diminishes the quality of life. As a monotherapy, HIFEM effectively strengthens the PFM and, in synergy with radiofrequency (RF), fortifies abdominal muscles. Thus this study aimed to investigate the effectiveness of abdominal and pelvic HIFEM treatments on the improvement of core muscle strength and quality of life.
Methods: Thirty-nine subjects (60-75 years, 19.7-33.9 kg/m2, skin type I-V) were studied. The treatment consisted of four abdominal HIFEM+RF and six pelvic floor HIFEM treatments over 6 weeks. Changes in the core strength were measured by a biofeedback device at baseline and follow-up. In addition, changes in waist circumference and QoL were assessed.
Results: 3-months following treatment, biofeedback demonstrated an increase in core muscle strength by 33.7% (p-value < 0.001) with a reduction in waist circumference of -3.1 ± 4.7 cm (p-value < 0.001). Several functional improvements were seen after 3 months with 89% of patients being able to get up from a seated position more easily, 76% with enhanced performance of daily activities, and 92% recommending treatment to family and friends. No serious adverse events or side effects of therapy occurred.
Conclusion: HIFEM and RF safely and effectively strengthen core muscles after consecutive treatments to the abdomen and pelvis in those over 65. This improvement enhances movement and positively impacts the quality of life.
HIFEM, Radiofrequency, Quality of life, Core strength, Elderly
HIFEM: High-Intensity Focused Electromagnetic Field; RF: Radiofrequency; QOL: Quality of Life; HSP: Heat Shock Proteins; PFM: Pelvic Floor Muscles; SC: Satellite Cells; IRB: Institutional Review Board; BMI: Body Mass Index; mmHg: millimeter of Mercury; VAS: Visual Analog Scale; ANOVA: Analysis of Variance; Tukey HSD: Tukey’s Honest Significant Difference; MRI: Magnetic Resonance Imagining; LH-AD: Anteroposterior Diameter; LH-LD: Laterolateral Diameter; and HA: Hiatal Area
As the population over 65 years of age continues to grow, the goal of quality living in our ‘golden years’ requires maintaining health, functional capacity and emotional well-being [1].
As we age, exercise and physical activity are major influences on maintaining the quality of life (QOL) as they may reduce the risk of age-related disease and enhances cognitive ability [2]. Core strength and stability are paramount, as they support coordination and function of the upper and lower body [3]. However, despite these known benefits, nearly 1/3 of adults over 65 lead sedentary lives as both external (such as lack of time) and internal (such as tiredness or lack of motivation) barriers prevent regular participation in physical activities [4,5]. As a supplement to prescribed routine exercise, technologies such as non-invasive high-intensity focused electromagnetic field (HIFEM) have been available to assist in maintaining strength and mobility for individuals with challenges to scheduling and/or accomplishing routine exercise. HIFEM technology uses an alternating magnetic field to depolarize the motor neurons in skeletal muscle tissue, thus leading to brain-independent supramaximal contractions. In these contractions, muscle fibers are stretched and relaxed, resembling resistance exercises of higher intensity. The muscle workload leads to micro-ruptures in the muscle fibers, releasing the signaling molecules responsible for regeneration and muscle growth [6,7]. The signaling molecules involved in muscle growth are heat shock proteins (HSP), inducing hypertrophy by promotion of muscle protein synthesis [8,9]. HIFEM has been shown to be effective for strengthening and toning the abdominal [10], gluteal [11], arm muscle groups [12], and rehabilitation of pelvic floor muscles (PFM) for treating urinary incontinence [13,14]. More recently, HIFEM technology has been combined with synchronized radiofrequency (RF) to enhance its effectiveness by RF heat. The combination of mechanical and thermal stress leads to the higher recruitment of satellite cells (SC) that boost muscle regeneration as they activate the differentiation of muscle fibers [15]. The favorable effects of HIFEM+RF have been shown for the abdomen [16], glutes [17], inner [18] and outer [19] thighs.
With the increasing average life expectancy for those > 65 is now 18.5 years, the growing elderly population and healthcare system will face challenges to maintaining health as functional status and the ability to exercise on a regular basis remain a challenge. As the number one reported disability for people 65 and older is difficulty with mobility, and 30% of older people having limitations in performing daily activities, the quality of life in elderly patients is in jeopardy [20]. Complementary techniques beyond exercise to maintain strength, balance, and QOL, are therefore desirable. HIFEM and HIFEM+RF technologies are promising to this end as they have established their role in muscle strengthening and toning.
This study aims to investigate the effectiveness and safety of the combined use of standalone HIFEM and synchronized application of HIFEM+RF for the strengthening of PFM and rectus abdominis and to improve functional status and quality of life.
This prospective, multicenter, open-label, one-arm study was approved by the Institutional Review Board (IRB) Advarra, was registered at ClinicalTrials.gov (NCT05537181), and followed the 1975 Declaration of Helsinki guidelines. The study was initiated in January 2022 and completed in November 2022. Eligible subjects (≥ 60 years, BMI < 35 kg/m 2 ) were screened for possible exclusion criteria such as electronic or metal implants, and other medical conditions contraindicating the application of electromagnetic fields and radiofrequency. Thirty-nine subjects (26 females, 13 males, 60-79 years-old, BMI of 19.7-33.9 kg/m 2 , skin type I-V) who did not meet any exclusion criteria were enrolled. All study participants were informed about the study protocol and signed the written informed concert form.
In this study, two devices were used consecutively. The first device utilizes HIFEM and RF energies simultaneously (Emsculpt Neo, BTL Industries, Boston, MA) through the large applicator. During the 30-minute procedure, patients lay in the supine position with a velcro belt fixing the applicator to the abdominal area. The treatment area is not covered by clothes, especially metal buttons or zippers. The four HIFEM+RF procedures are planned 5-10 days apart. The second device utilized a standalone HIFEM energy (Emsella, BTL Industries Inc., Boston, MA) through the chair applicator. During the 28-minute procedure, subjects sit upright on the chair applicator, fully clothed. The six standalone HIFEM procedures are scheduled twice weekly, spaced 2-4 days apart. In both devices, the intensities of emitted energies are set according to the patient’s feedback to maximally tolerated levels (0-100%). The treatment protocol included seven (n = 7) treatment sessions. Both procedures were used consecutively at the first, third, and fifth treatment visits, starting with HIFEM+RF (Table 1). Two follow-up visits were scheduled 1 month and 3 months after the treatments.
Table 1: The schedule of treatments. View Table 1
The primary endpoints included measuring core strength with the pressure biofeedback device and evaluating changes in subjects’ quality of life through the Subject Satisfaction and Experience Questionnaire.
The biofeedback pressure device (Stabilizer, Chattanooga Group, Hixson, TN) is a tool for detecting the movement in the lumbar spine linked to contractions of core muscles and provides information about the functionality of deep abdominal muscles [21]. The changes in the pressure (mmHg) are detected by an air-filled pressure cell. During the measurement, the patient is in the supine position, with their legs bent at a 90° angle in the knees and feet on the flat surface. The pressure cell is placed under the area of the lumbar spine (Figure 1). The initial pressure level in the pressure cell is set to 40 mmHg, and the change in pressure generated by squeezing the core muscles is visible on the pressure gauge. During the measurement, subjects were instructed to avoid squeezing gluteal muscles and lifting their shoulders or neck. The biofeedback data were collected at baseline, after the last treatment, and at 1-month and 3-month follow-up visits.
 Figure 1: The visualization of the position during the biofeedback pressure measurement.
View Figure 1
Figure 1: The visualization of the position during the biofeedback pressure measurement.
View Figure 1
The Subject Satisfaction and Experience Questionnaire consisted of 21 questions regarding changes in daily life, such as improvement in body movement and flexibility, balance, back pains, stability, and activeness in daily life (Table 2). The answers were based on the 5-point Likert scale, where 1 means strongly disagree, and 5 means strongly agree. The questionnaire was filled after the treatments and at 1-month and 3-month follow-up visits. The three recorded scores obtained were averaged. The percentage (%) of satisfied patients was calculated as the number of patients who scored > 3 and divided by the number of subjects who answered the question.
Table 2: The list of questions in the Subject Satisfaction and Experience Questionnaire with an average (%) of patients who agreed or strongly agreed with the question. Two questions, number 7 and 12, were answered by 23 and 24 patients, respectively. The rest of the questions were answered by 38 patients. View Table 2
The secondary endpoints included waist circumference, assessment of comfort during the therapy through the Therapy Comfort questionnaire, the aesthetic improvement of the abdomen based on digital photographs, and monitoring of adverse events and side effects.
During the waist circumference measurement, subjects were asked to stand straight with both feet firmly on the ground, and exhale, with the waist area covered with a non-stretch tape and measured at the level of the navel. The measurements were taken at baseline, after the last treatment, and at 1-month and 3-month follow-up visits.
The Therapy comfort questionnaire consisted of “I found the treatment procedure comfortable” question assessed by a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree) and a 10-point visual analog scale (VAS) serving as an assessment of pain during the treatments, with 0 meaning no pain and 10 means worst pain possible. The questionnaire was filled out after the last treatment session.
The digital photographs were taken at baseline, after the last treatment, and at 1-month and 3-month follow-up visits.
The descriptive analysis (such as average and standard deviation) and statistical analysis of the collected data were completed. The statistical significance was tested by One Factor ANOVA Repeated Measures with Tukey HSD post-hoc test with a significance level ɑ set at 5%.
Out of 39 enrolled subjects, 38 (26 females, 12 males, 60-79 years-old, BMI of 19.7-33.9 kg/m 2 , skin type I-V) received the treatments and underwent 1-month and 3-month follow-up visits. One patient was withdrawn (due to reasons unrelated to the study) before receiving any treatment. Subjects did not report any discomfort even during the consecutive application of both devices and resumed their daily activities right after the treatments without any issues. There were no side effects observed, with no serious adverse events. However, one patient had developed a small blister on the abdomen. The blister had healed normally without leaving scar tissue or needing additional medical care.
The results of 38 subjects demonstrated an average baseline biofeedback pressure value (representing the baseline core muscle strength) was 84.1 ± 47.2 mmHg. The biofeedback pressure value showed continuous improvement during the study while peaking at a 3-month follow-up at 112.4 ± 47.2 mmHg (+33.7%, p-value < 0.001). In the study, twelve subjects (n = 12) showed an increase in biofeedback pressure greater than 50%, with four (n = 4) exceeding a 100% increase (Figure 2).
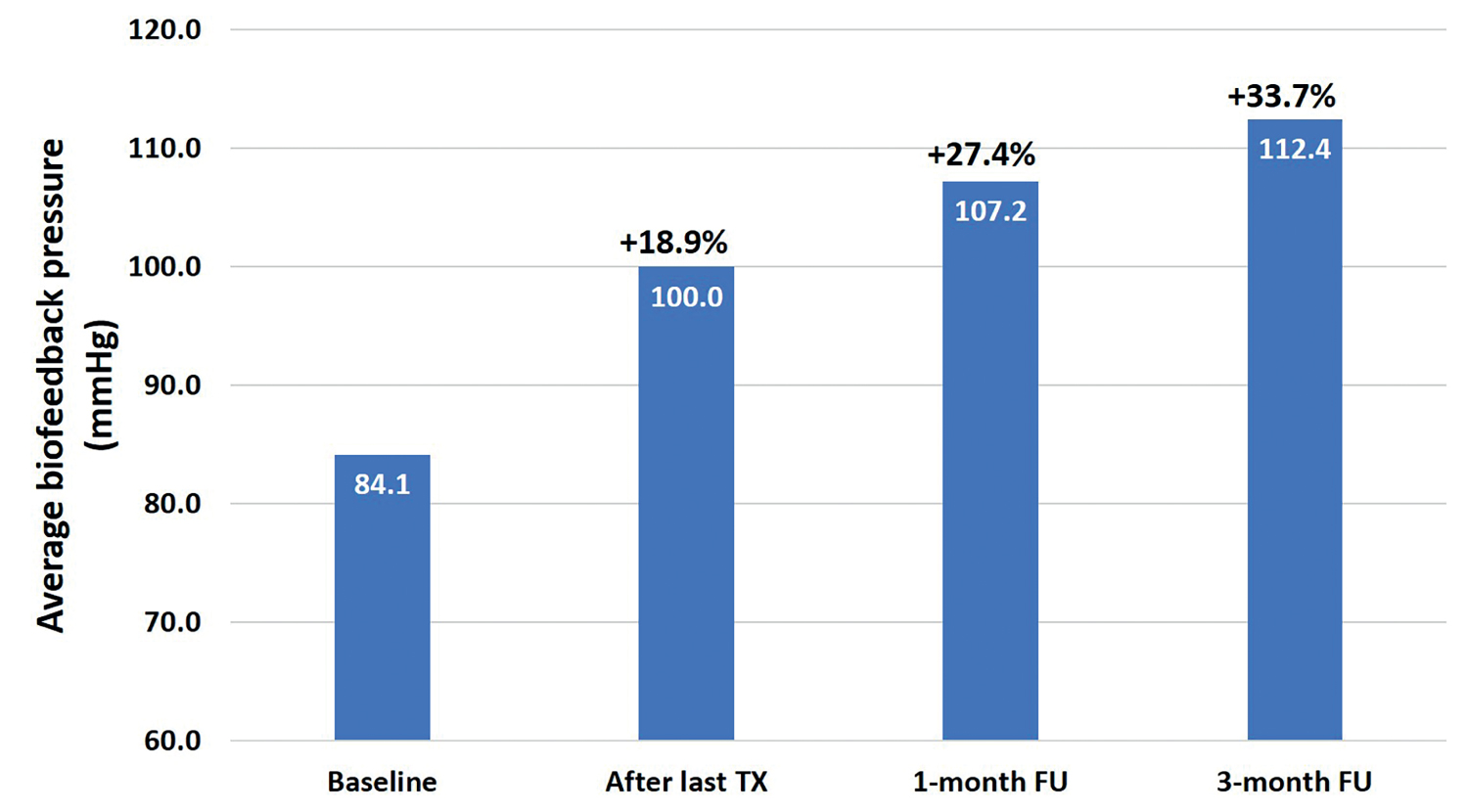 Figure 2: A bar graph showing the average value of biofeedback pressure and an increase in percentage (%).
Figure 2: A bar graph showing the average value of biofeedback pressure and an increase in percentage (%).
Tx: Treatment; FU: Follow-Up.
View Figure 2
The Subject Satisfaction and Experience Questionnaire revealed an overall satisfaction of 74.2%. A more detailed inspection showed that 92.1% of subjects were satisfied with treatment outcomes and would recommend this treatment to family and friends. More than 85% of patients felt improved overall body movement, urinary incontinence, a stronger core, and could get up more easily from a sedentary position. More than 75% of patients felt improved flexibility and back discomfort, with the ability to perform their daily activities better. More than 70% of patients have better posture and stability, felt more active, and their workout performance improved. More than 65% of patients reported improved balance, felt more stable on their feet, and enjoyed their leisure activities more. More than 60% reported less discomfort while carrying things, could walk longer distances, and could stand for long periods of time. And lastly, more than 50% of patients reported improvement in sexual performance and could take better care of themselves (Table 2).
Waist circumference exhibited a gradual and significant reduction while peaking at the 3-month follow-up visit with a -3.1 cm (p-value < 0.001) from a baseline average of 90.4 cm, with four (n = 4) patients exceeding a waist circumference reduction of -10 cm. The improvement in abdominal contour is visible in Figure 3 and Figure 4.
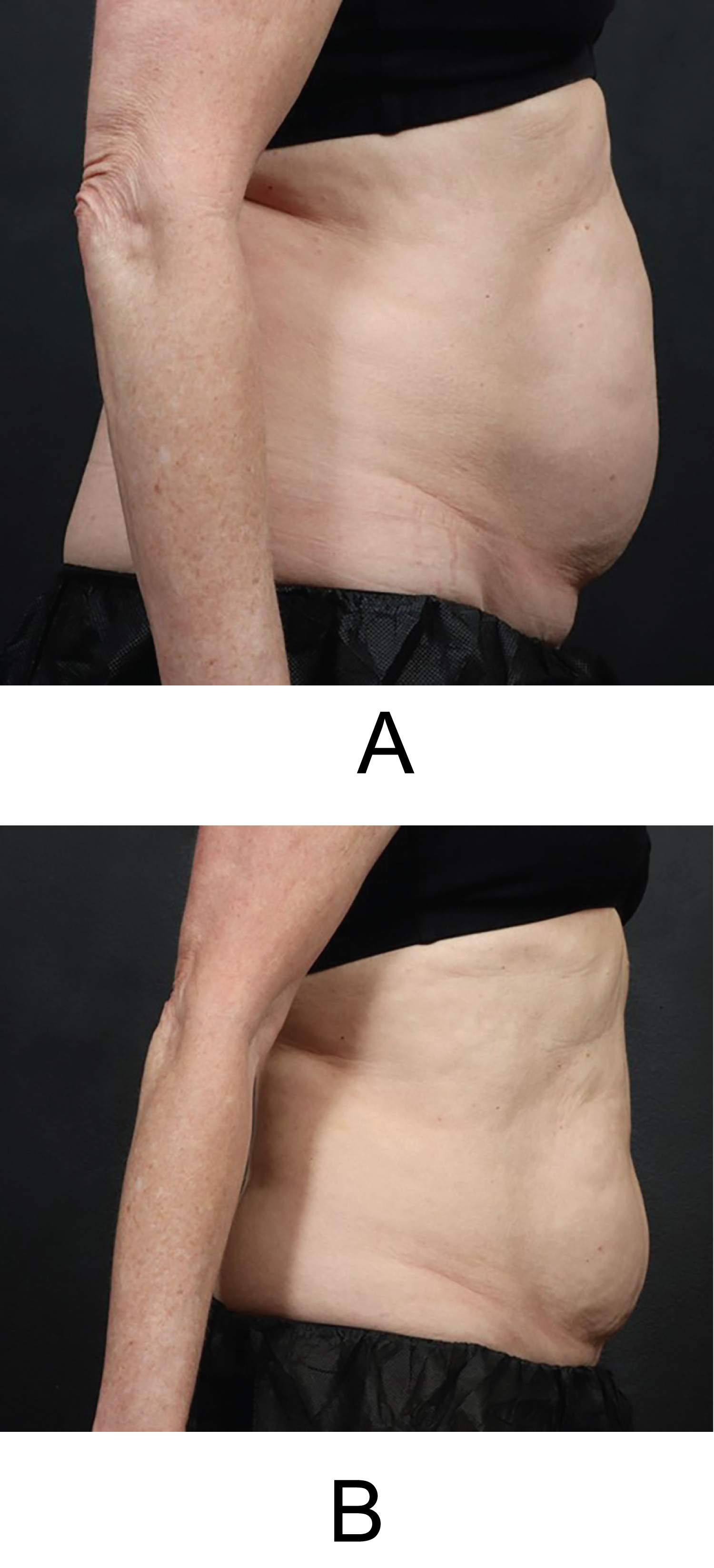 Figure 3: Digital photographs of a 65-years-old female (BMI of 21.1 kg/m2). The patient showed an average of 17.3% increase in biofeedback pressure measurements at the 3-month follow-up, with -2.1 cm in waist circumference, and high overall satisfaction with the treatments of 4.9 Baseline = A, 3-month follow-up = (B).
View Figure 3
Figure 3: Digital photographs of a 65-years-old female (BMI of 21.1 kg/m2). The patient showed an average of 17.3% increase in biofeedback pressure measurements at the 3-month follow-up, with -2.1 cm in waist circumference, and high overall satisfaction with the treatments of 4.9 Baseline = A, 3-month follow-up = (B).
View Figure 3
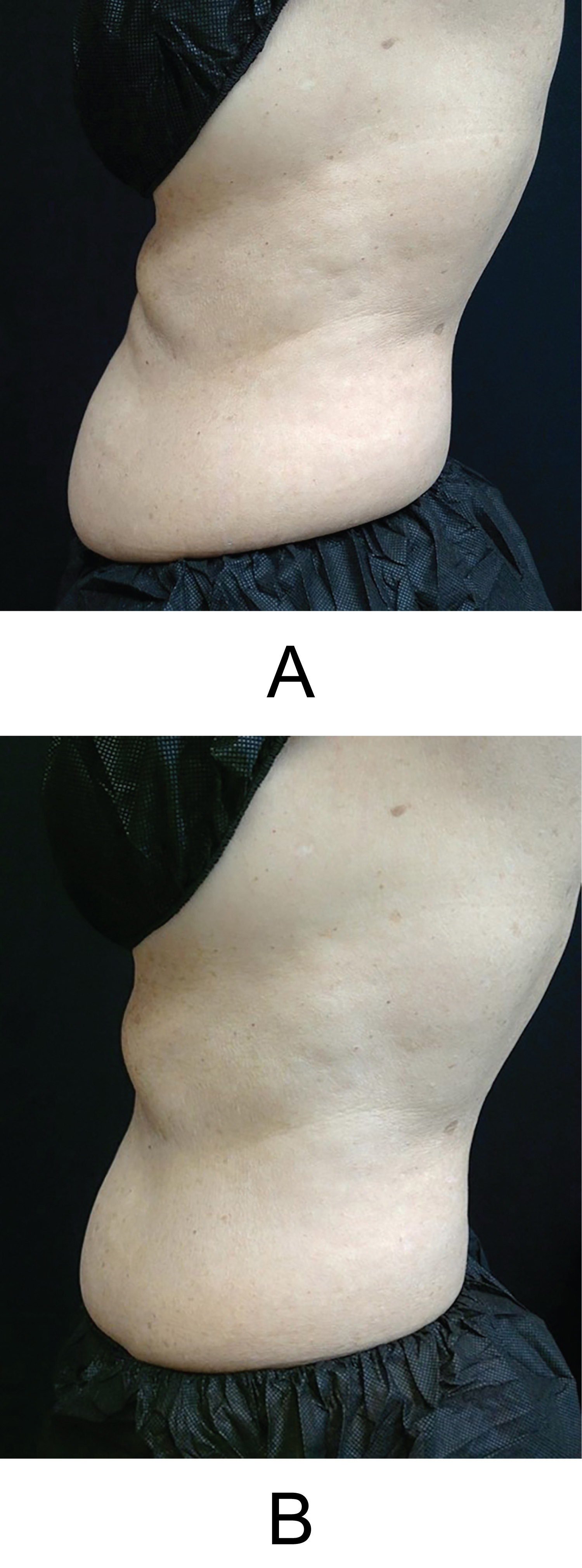 Figure 4: Digital photographs of a 60-years-old female (BMI of 22.0 kg/m2). The patient showed an average of 55.6% increase in biofeedback pressure measurements at the 3-month follow-up, with -2.5 cm in waist circumference, and high overall satisfaction with the treatments of 4.2. Baseline = A, 3-month follow-up = (B).
View Figure 4
Figure 4: Digital photographs of a 60-years-old female (BMI of 22.0 kg/m2). The patient showed an average of 55.6% increase in biofeedback pressure measurements at the 3-month follow-up, with -2.5 cm in waist circumference, and high overall satisfaction with the treatments of 4.2. Baseline = A, 3-month follow-up = (B).
View Figure 4
The procedure was accompanied by high comfort rates during the treatments, as 76.3% of subjects agreed or strongly agreed with the question. The average VAS score was 2.5 ± 2.1 points, indicating only mild procedural discomfort.
Our study demonstrated that consecutive use of standalone HIFEM and simultaneous application of the HIFEM+RF strengthened core muscles and improved quality of life. The evaluation showed highly significant results in increasing the core muscle strength with high satisfaction of the subjects, demonstrating the potential of the utilized technologies to improve quality of life. Patients reported mild pain during the treatments, which may be due to an age-related increased susceptibility to pain [22] as the previous studies on the individual devices reported no pain [14,18]. There were no treatments discontinued due to discomfort or pain, and subjects could resume their daily activities without downtime. Only one mild adverse event occurred, which was resolved without any issues.
The review by van Leeuwen, et al. [23] identified nine QoL domains, with autonomy (being able to manage on your own, retaining dignity, and not feeling like a burden), role and occupation (spending time doing activities that bring a sense of value, joy, and involvement), attitude and adaptation, health perception (feeling healthy and not limited by your physical condition), and relationships domains being the most important. As the number one reported disability for people 65 and older is difficulty with mobility, and 30% of older people having limitations in performing daily activities, the quality of life in elderly patients is in jeopardy.
Several previous studies have shown morphological changes in muscle tissue after HIFEM and synchronized radiofrequency and provide insight into the mechanism of action [24]. An MRI study by Jacob, et al. [16] showed an increase in rectus abdominis by 26.1% (+2.3 ± 0.8 mm) with a decrease in abdominal separation by 18.8%. Samuels, et al. [25] measured muscle thickness changes by ultrasound and discovered an increase in muscle thickness of +24.2% three months after similar treatment. To observe the dynamics of changes in the pelvic floor muscles, a 3D ultrasound was used in the study by Silantyeva, et al. [26]. The study measured biometric indices of pelvic floor integrity such as anteroposterior diameter (LH-AD) and laterolateral diameter (LH-LD) of levator hiatus and hiatal area (HA). After the treatments, patients showed an average LH-AD reduction of -3.12 mm, -3.04 mm reduction in LH-LD, and -1.38 mm in HA.
A longitudinal study by Trombetti, et al. [27] discovered that the decline in muscle mass and muscle performance contribute to both an increased fear of falling and a decline in the quality of life. Importantly, our study suggests that non-invasive muscle strengthening with HIFEM and RF is feasible, well-tolerated, and may lead to improvements in strength and quality of life. Additionally, the rate of patients who agreed or strongly agreed with the statements in the satisfaction questionnaire ranged from 52.2% (improvement in sexual performance) to 92.1% (satisfaction with the results), averaging 74.2%, demonstrating improvement in several important aspects of patients’ lives.
Hlavinka, et al. [28] showed that the standalone HIFEM procedure improved sexual satisfaction by 76% in patients of an average age of 36-years-old, with Evans, et al. [29] showing a 33% improvement in a female population with an average age of 49-years-old. Taking into consideration the population/age differences and the questionnaires used in these studies, we consider the 54.2% improvement in sexual performance documented in the current study as a sign of effectiveness. Of note, only 24 out of 38 patients answered this question, showing some response bias, as subjects may have been reluctant to discuss their sex life even with healthcare staff due to embarrassment or persisting stigma [30,31].
One strength of this study is the combination of both objective and subjective efficacy measures, demonstrating agreement and this connecting the idea that strength relates to the quality of life. We hope to see other metrics in future studies that might include data on bioelectrical impedance analysis or MRI, enabling further explanation of the relationship between muscle mass, strength, and function in further detail. In addition, the inclusion of physical performance tests could be valuable to fully explore the utility of combined HIFEM+RF and standalone HIFEM treatments. The joint use of quantitative and objective methods is important. Despite the valuable information from questionnaires, they may be more prone to bias. However, being aware of the source of the biases, we believe that the questionnaires provide important information about the subjects’ lives, and their use in this study, together with biofeedback, measurement is valid. Lastly, only one patient dropped out without receiving any treatments. Therefore, a complete analysis of the changes in 38 subjects after the treatments could be performed. However, only 12 male patients participated, and therefore it is a matter of future research to include more male subjects to allow statistical analysis of sufficient power between the genders. Additionally, future studies should include longer follow-up or retrospective analyses to evaluate the long-term outcomes of the treatment regime.
The present study indicates the effectiveness of the combined use of standalone HIFEM technology and simultaneous application of HIFEM+RF to strengthen core and pelvic floor muscles with no side effects. In addition, this approach can lead to better function and quality of life and should be considered as a supplement to regular exercise for those who are unable to reach their goals with activity alone.
All authors conducted the research and equally contributed to the manuscript draft and finalization. All authors are medical advisors for BTL Industries, which was a sponsor of the study and provided the study devices. No funding for authorship and publication of this article was provided.
All authors, Dr. Duncan, Dr. Kent, and Dr. Appelbaum are clinical investigators for BTL, and BTL Industries was the sponsor of this multi-center study and provided the study device. However, no funding for the research, authorship, and publication of this article was provided.
All authors contributed equally to the research and manuscript draft and finalization.