Objectives: Treatment-seeking behaviour, evaluation and management approach, as well as responsiveness to management by individuals with knee osteoarthritis (OA) could be hampered by variations of common confounding (constant) factors of knee OA; age and sex. Studies that integrate age and sex variations in clinical factors such as pain intensity and physical function are limited. The aim of this study was to determine age and sex variations in pain intensity and physical function among individuals with knee OA in Nigeria.
Design/setting/participants/outcome measures: Eighty-nine consecutively sampled patients diagnosed with knee OA from three selected public (secondary and tertiary) hospitals in Enugu, South-East Nigeria, participated in this cross-sectional survey. Instruments used were Visual Analogue Scale (VAS) and Ibadan Knee or Hip Osteoarthritis Measure (IKHOAM). Data were analysed using Analysis of Variance (ANOVA) and Students'-test with Bonferroni correction. The level of significance was set at 0.05.
Results: Significant variations of age in pain intensity between age groups of 20-39 and each of 40-59 years (MD = -3.68, p = 0.01) and 60-79 years (MD = -3.23, p = 0.04) as well as physical function between age groups of 60-79 and each of 20-39 years (MD = 20.85, p = 0.02) and 40-59 years (MD = 10.70, p = 0.03) were observed. There was a significant sex variation in physical function, (F = 9.57, p < 0.05) but not in pain intensity (F = 2.91, p = 0.09) on one-way ANOVA, with females reporting higher scores on pain intensity (5.29 ± 2.97) and lower scores on physical function (64.06 ± 17.26) than males (3.94 ± 2.29 and 78.77 ± 17.08 respectively).
Conclusions: Age and sex should be considered by clinicians in management programs for knee OA to address the specific needs of each individual patient.
Age, Sex, Pain intensity, Physical function, Knee osteoarthritis
• Confounding (constant) factors of knee OA (age and sex) could affect response to treatment. Increased chronic pain intensity and decreased physical function with increased age especially among Nigerian women was proposed.
• Middle-aged individuals (40-59 years) with knee OA reported higher pain intensity especially among women and higher physical function among men. Low pain intensity and better physical function existed among younger adults (20-39 years) compared to others.
• Highly effective pain management as well as interventions to improve physical functions needful for women with knee OA at 40-59 years of age in Nigeria.
Osteoarthritis (OA) is a classic debilitating age-related disorder characterized by slow progressive articular cartilage destruction, ultimately leading to disabling pain and joint dysfunction [1-3]. The knee, a weight bearing joint has been reported to be the most commonly affected joint especially among Africans [3]. Osteoarthritis of the knee tends to cause the greatest burden to the adult population as joint pain and stiffness leads to significant disability requiring surgical intervention [3], especially total knee replacement [4]. Common endogenous predisposing factors of knee OA include age and sex. While stress is associated with age-related loss in the ability of body cells and tissues to maintain homeostasis [5], the prevalence and incidence of knee OA is higher in women than in men, and in women, it increases dramatically around the time of menopause due to loss of oestrogen with resultant lower cartilage turnover [6-8].
Age and sex differences in the clinical status of individuals with chronic pain are likely to affect their treatment-seeking behaviour, the evaluation and treatment approach, and the responsiveness to treatment [9]. Previous studies on the relationship between age and the intensity of chronic pain revealed direct, inverse or no relationship [10]. Variability of the pain assessment tools had been suggested to be the reason for the inconsistencies. However, there was no age difference in the intensity of chronic pain measured with uni-dimensional scales (Visual Analogue scale and so on) [10]. Sex differences have been observed in pain intensity and self-reported functional ability but not in actual functional performance [11]. Published studies that simultaneously integrate both domains of age and sex among knee OA patients are limited particularly in Nigeria. Developing countries have seen that cultural factors affect the degree of pain, which also invariably affects physical function in such population. It was hypothesized that there would be increased chronic pain intensity and decreased physical function with increased age especially among women. As such, this study aimed to describe the variations of age and sex in chronic pain intensity and physical function in a sample of Nigerians with osteoarthritis (OA) of the knee.
The sample size for this cross-sectional exploratory survey was 99, calculated using the formula by Sullivan [12] (using prevalence of knee OA from a hospital-based study in Nigeria to be 6.9% [13].
N = p (1-p) (z/E)2
Where:
N = Sample size
p = Prevalence (Prevalence of knee OA from a hospital-based study in Nigeria = 6.9% [13]
z = 1.96 {that is, 95% confidence interval (alpha level = 0.05)}
E = Margin of error (1%)
Thus N (sample size) = 0.069 (1 - 0.069) (1.96/0.01)2 = 82.17
Consecutive sampling technique was used to recruit one hundred and four patients who fulfilled all the inclusion criteria from Parklane, National Orthopaedic and University of Nigeria Teaching hospitals, Enugu, South-East Nigeria. After recruitment, patients who consented to participate in the study completed demographic/clinical data forms and the selected instruments. Participants were free to drop out of the study at any point without providing a reason.
Participants eligible for the study were patients with (i) The ability to read and write Igbo or English, (ii) Having chronic clinical features of only knee OA according to the Clinical Classification Criteria for knee OA of the American College of Rheumatology (ACR). The ACR clinical classification criteria for diagnosing osteoarthritis of knee joint (2012) involves using history and physical examination (pain in the knee and at least any 3 of the following- over 50 years of age, less than 30 minutes of morning stiffness, crepitus on active movement, bony tenderness, bony enlargement or no palpable warmth of the synovium) or using history, physical examination and radiographic findings (pain in the knee and at least any 1 of the following- over 50 years of age, less than 30 minutes of morning stiffness, crepitus on active movement or presence of osteophytes) [14].
Participants were excluded according to the following criteria; (i) Prior knee surgery (ii) Acute knee trauma (iii) Any other form of arthritis (iv) Intra-articular corticosteroid injection to the knee(s) 3 weeks prior recruitment for the study (v) Previous knee arthroscopic or arthroplasty. Each participant performed the physical performance tests on IKHOAM as the researcher or a trained research assistant (physiotherapists) rated.
Pain Visual Analogue Scale (PVAS): English and Igbo versions [15,16]: It is a continuous scale comprising of a horizontal (HVAS) or vertical (VVAS) line which measures from 0 to 10 m and is anchored by 2 verbal descriptors, one for each symptom extreme [15,17] with 0m indicating 'no pain', 5 m indicating 'moderate pain' and 10 m indicating 'worst imaginable pain' [17-19]. Using a ruler, the score is determined by measuring the distance (m) on the 10 m line between the “no pain” anchor and the patient's mark, providing a range of scores from 0-10 [17]. A higher score indicates greater pain intensity and vice versa. The pain VAS has been shown to possess adequate reliability and validity [20]. Test-retest reliability has been shown to be good, but higher among literate than illiterate patients [18]. In patients with pain associated with knee OA, the scale has demonstrated sensitivity to changes in pain assessed hourly for a maximum of 4 hours and weekly for up to 4 weeks following analgesic therapy [21].
Ibadan Knee or Hip Osteoarthritis Measure (IKHOAM): English and Igbo versions [13,22]: The scale is a 3-domain/part, 33- item instrument with domains consisting of activity limitations, participation restrictions and physical performance tests (250m walk test, one leg stance test, stairs climbing test, squat test, and balance test on a balance board). The IKHOAM has been tested for validity [13], responsiveness [13], reliability [23] and minimal clinical important difference [22]. The maximum obtainable score on IKHOAM is 232. The score for a subject was calculated as the percentage of the total possible score. Low score on IKHOAM implies low level of physical functioning ability and vice versa [24].
Ethical approval (UI/EC/15/0059) was sought and obtained from the University of Ibadan/University College Hospital Health Research Ethics Committee before the commencement of the study. Permission to conduct the study was obtained from the various Heads of Physiotherapy department; General, Medical and Surgical units of the selected public hospitals before the commencement of the study. Informed consent was sought and obtained from each participants using an informed consent form before the participants were screened for eligibility.
After recruitment, patients who consented to participate in the study completed demographic/clinical data forms and the various instruments. Each participant performed the physical performance tests on IKHOAM as the researcher or an assistant rated.
Obtained data was cleaned, entered into and analysed using SPSS (Statistical Package for the Social Sciences) software, version 15.0 for Windows 7. Descriptive statistics (mean, standard deviation (S.D.), range, and frequency) was used to summarize the demographic (age, sex, occupation, religion, marital status and so on) as well as clinical variable (affected knee). According to World Health Organisation (WHO), the standard age categorization is the five-year age group: 0-4, 5-9 and so on [25]. To increase power and minimize the number of comparisons made, the originally 13 age categories were collapsed into 4 age groups (20-39, 40-59, 60-79, and 80+) when testing for differences due to sex and age. Two-way analysis of variance (ANOVA) and Students'-test with Bonferroni correction was used because of multiple comparisons. The level of significance was set at 0.05.
One hundred and four patients (18 males, 86 females) with knee osteoarthritis ranging between 20 and 84 years participated in this study but only eighty-nine of them (16 males, 73 females) completed the study. With the exception of bilateral knee joint affectation (40.0%), participants with affectation of the right knee joint only were more in distribution (39.1%).
In general, participants of 20-39 years reported least and highest scores on pain intensity and physical function respectively as shown in Table 1. The highest score on pain intensity was observed among subjects of 40-59 years of age whereas those beyond 80 years reported the least score on physical function. Female participants reported highest scores on pain intensity especially at 40-59 years (5.88 ± 2.59) whereas their male counterparts reported highest scores on physical function (91.55 ± 2.67) at same age range as shown in Table 1.
Table 1: Mean scores (age, PI, PF, number of joints affected) and SD in different age groups among male and female participants. View Table 1
The one-way ANOVA (Table 2) showed a significant sex variation on physical function only (p < 0.05) but not on pain intensity (p = 0.09). Females reported higher scores on pain intensity (3.94 ± 2.29) and lower physical function (64.06 ± 17.26) than males (5.29 ± 2.97 and 78.77 ± 17.08 respectively). On a general note, participants of age group 40 to 59 years reported highest pain intensity whereas those of age group 20 to 39 years reported highest scores on physical function. The two-way analysis of variance (Table 3) showed significant main variations of age on pain intensity (F = 2.87, p = 0.04), age on physical function (F = 4.74, p < 0.001) and sex on physical function of the participants (F = 5.84, p = 0.02). However, there was a non-significant effect of sex on pain intensity of the participants (F = 0.38, p = 0.54). This means that both pain intensity and physical function vary according to age whereas only physical function varies according to sex. In other words, when sex is ignored, pain intensity and physical function vary with age but when age is ignored, physical function varies with sex, which was not the case for pain intensity.
Table 2: One-way ANOVA comparing gender differences in pain intensity, and physical function (N = 87). View Table 2
Also, there was no statistically significant combined effect or interaction between age and sex on both pain intensity (F = 0.06, p = 0.98), and physical function of the participants (F = 1.27, p = 0.29) as also shown in Table 3. This non-significant interactive effect of age and sex on both pain intensity and physical function was also demonstrated in the line graphs of Figure 1 and Figure 2 respectively where the lines were parallel and did not cross each other. In other words, there is an ordinal interaction between age as well as sex and pain intensity and physical function - in part, because there is a consistent order to the levels. This implies that age and sex variations on pain intensity and physical function were different for male participants than it was for females, though not statistically significant.
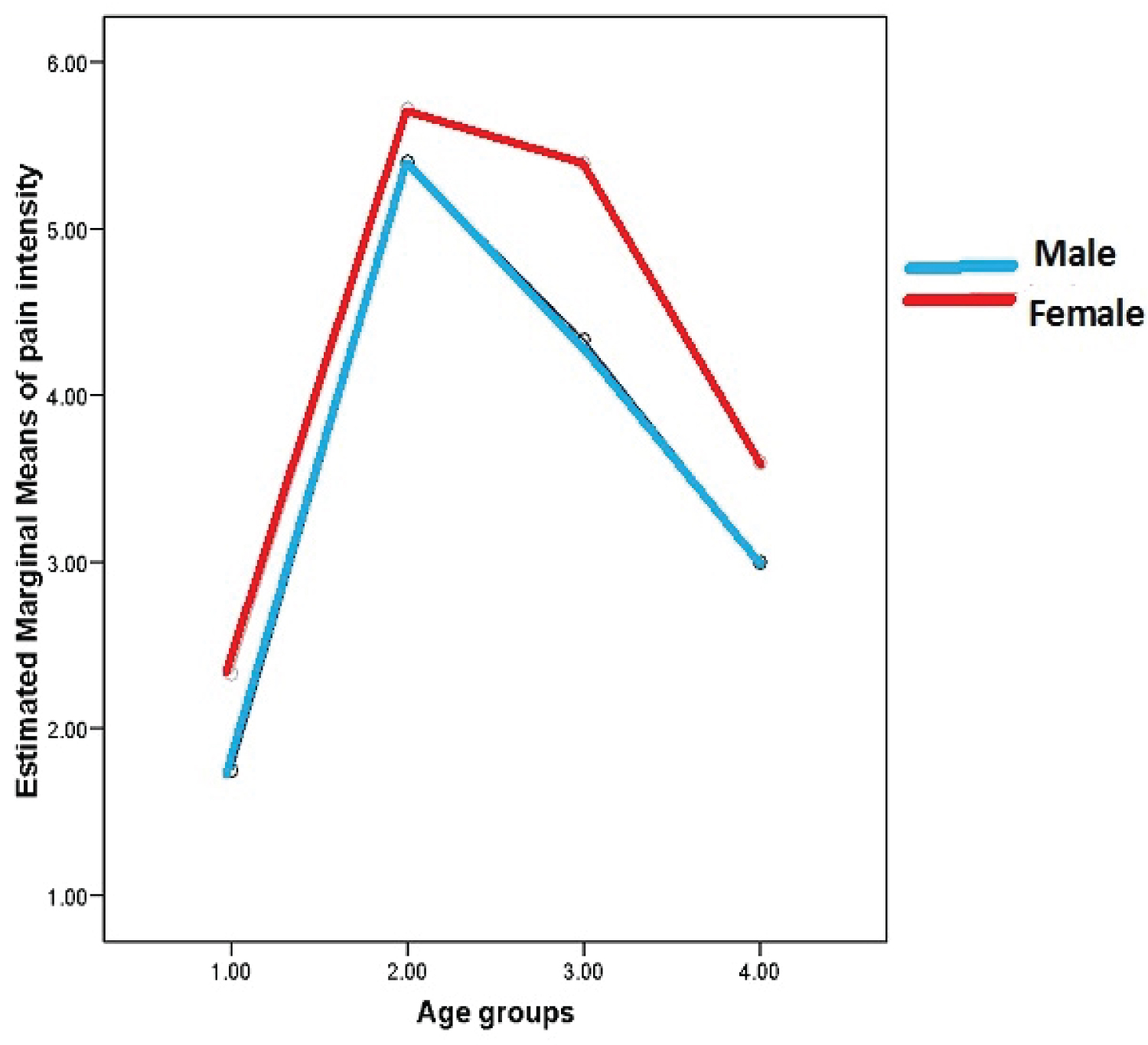 Figure 1: Graph of the interaction effect of age and sex on pain intensity of the participants.
Figure 1: Graph of the interaction effect of age and sex on pain intensity of the participants.
Key: Age groups: 1 = 20-39 years, 2 = 40-59 years, 3 = 60-79 years, 4 = 80+ years
View Figure 1
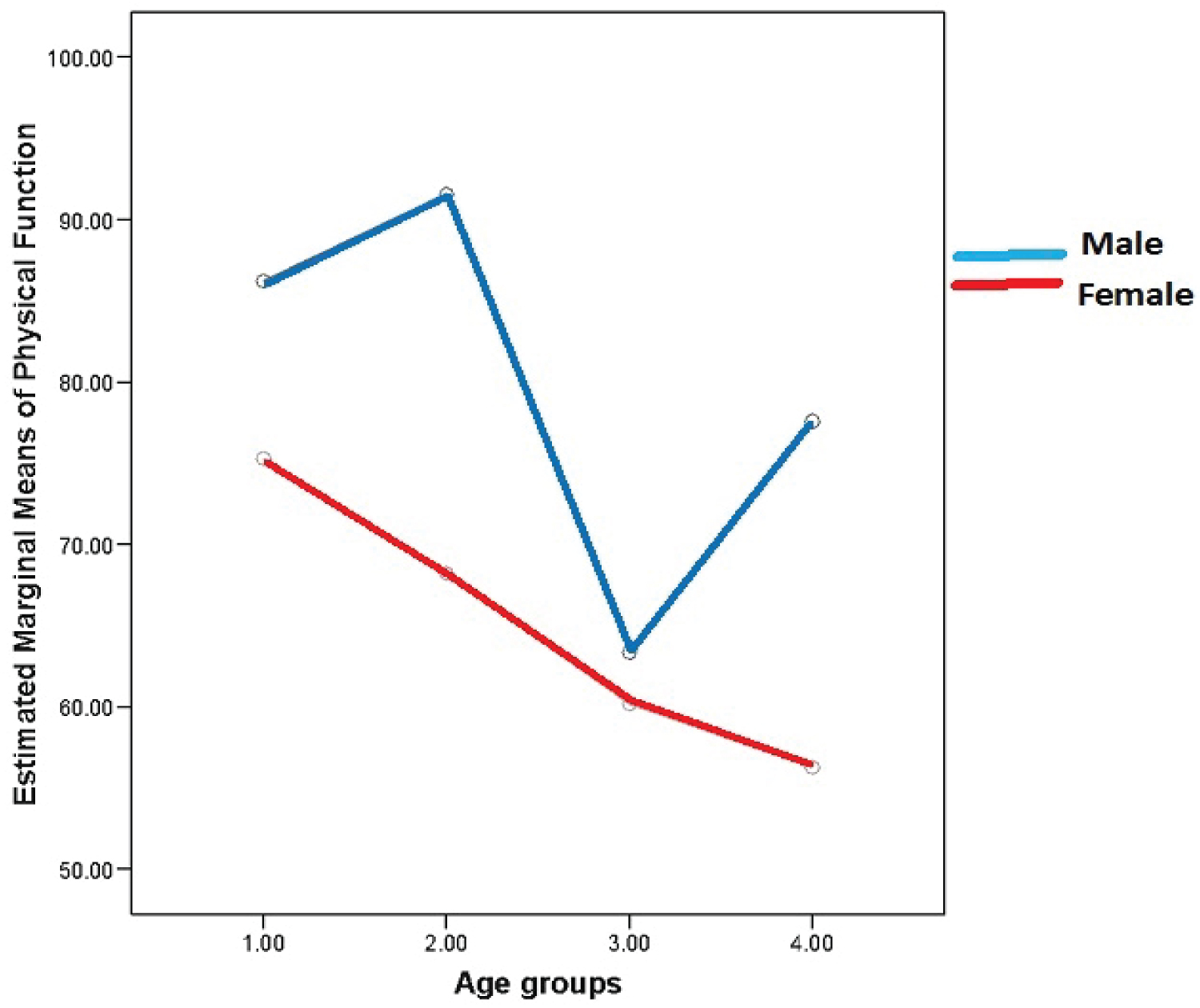 Figure 2: Graph of the interaction effect of age and sex on physical function of the participants.
Figure 2: Graph of the interaction effect of age and sex on physical function of the participants.
Key: Age groups: 1 = 20-39 years, 2 = 40-59 years, 3 = 60-79 years, 4 = 80+ years
View Figure 2
Table 3: Two-way ANOVA showing the interactive effects of age and sex on each of pain intensity and physical function. View Table 3
The Bonferroni post-hoc test (Table 4) revealed that the significant variations in pain intensity was only between age groups 20-39 years and 40-59 years (p = 0.01), and age groups 20-39 years and 60-79 years (p = 0.04). There was no significant difference between age groups 40-59 years and 60-79 years (p = 1.00), 40-59 years and ≥ 80 years (p = 0.49), 60-79 years and ≥ 80 years (p = 0.98) as well as between ≥ 80 years and 20-39 years (p = 1.00). It is interesting to note that age groups 40-59 years and 60-79 years as well as ≥ 80 years and 20-39 years report equally pain intensities (p = 1.00) indicating that the pain intensity of participants in such groups were identical. On physical function, the recorded significant difference in ANOVA was only between age groups 20-39 years and 60-79 years (p = 0.02) as well as 40-59 years and 60-79 years (p = 0.03). There was however no significant differences between age groups 20-39 years and 40-59 years (p = 0.81), 20-39 years and ≥ 80 years (p = 0.11), 40-59 years and ≥ 80 years (p = 0.67), 60-79 years and ≥ 80 years (p = 1.00). Age groups 60-79 years and ≥ 80 years appear to report equal physical function as shown in Table 4.
Table 4: Post-Hoc (Bonferroni) paired-multiple comparisons of pain intensity and physical function between age categories. View Table 4
The patients assessed in this study were predominantly female (82%), suggesting that females had greater odds of developing knee OA and generally at a higher risk of it, particularly after menopausal age. This therefore, is consistent with the result of previous studies [6-8] in which the higher prevalence and incidence of knee OA in women increases dramatically around the time of menopause due to loss of oestrogen associated with lower cartilage turnover. Other possible contributory factors to high proportion of females with OA may include molecular changes and lifestyle adaptations (reduced physical activity, diet, obesity and so on) [26].
The results of the present study showed that there are age-and sex variations in chronic pain intensity and physical function of individuals with knee OA as measured by VAS and IKHOAM respectively. It has been previously reported that among patients with chronic pain, there are age and sex differences; and that females presented greater number of distinct chronic pain [27]. Therefore, findings from this present study are consistent with the reports of Cook and Chastain [27]. The findings show that among male and female participants, pain intensity increased with age below 40 years but decreased beyond that. One would think that pain intensity would increase with age since knee OA is a chronic progressive degenerative joint disease which most often affects middle-aged to elderly people [27], ultimately leading to disabling pain and joint dysfunction [2,3,28], but on the contrary, older adults appear to have developed effective pain coping strategies. As such, factors such as cohort differences, and/or physiological or psychological adjustment processes are reflected by distinct clinical profiles, which older patients do present with [27]. Additionally, results of few other studies have revealed that when compared with younger patients, older patients report good or better quality of life, mood as well as marital and social satisfaction, notwithstanding experiencing higher chronic pain intensity [29,30].
On physical function, it was not surprising that there was an initial increase among male and female participants between 20 and 39 years, which preceded a decline from 40 years and above but among men, in particular, it increased above 79 years of age. This could possibly be that men appear to have better pain coping strategies than women that invariably helped them to function better physically [31]. This current study therefore, suggests that older adults (both males and females) with knee OA manage their pain effectively better than the younger ones and among male participants specifically (beyond 80 years), but does not interfere with their physical function.
A drawback of this study is its cross-sectional design, which gives less helpful information about the possible causative factors to the conclusions drawn from this study. In addition, the sample for male individuals was small; therefore, there should be equal-number of sex replication of this present study to enable a better assessment of age and sex variations on the independent variables. The absence of data on the use and the number of analgesic/anti-inflammatory drugs as well as their diabetic/hypertensive status of the patients are some of the limitations of this study given that these drugs may have interfered with the quality and intensity of the pain. More so, the generalizability of these results to a larger population with knee OA pain may be limited because only individuals with chronic knee OA pain were included in this study.
Significant variations of pain intensity, physical function with age and physical function with sex of the participants seem to exist but there was an insignificant sex variation on pain intensity. When sex is ignored, pain intensity and physical function varies with age but when age is ignored, pain intensity did not vary with sex on the contrary of physical function.
There seems to be significant variations in pain intensity between age groups of 20-39 years and 40-59 years, as well as 60-79 years respectively while on physical function, there are significant variations between age groups of 20-39 years and 60-79 years respectively as well as 40-59 years and 60-79 years. Low pain intensity and better physical function existed among younger adults (20-39 years) compared to others.
A significant sex variation was observed on physical function but not on pain intensity with females reporting higher scores on pain intensity and lower scores on physical function. Women with knee OA experienced higher level of pain at 40-59 years compared to men. At 40-59 years, male individuals with knee OA encountered higher level of physical function than their female counterpart using IKHOAM.
Thus, highly effective pain management and interventions to improve physical function are important for Nigerian women with knee OA at 40-59 years of age. Given that age and sex are confounding demographics of knee OA, treatment should therefore be modified in addressing the specific needs of individuals with knee OA.
The authors thank all patients with knee OA in the selected public hospitals in Enugu, South East Nigeria for their kind participation in this study. The authors' sincere thanks are due to the research assistants (physiotherapists), orthopaedic surgeons and nurses for their co-operation with the recruitment.
University of Ibadan/University College Hospital Health Research Ethics Committee (UI/EC/15/0059).
The study was self-funded.
None declared.