Vitamin D deficiency in Crohn's disease (CD) patients has been extensively stressed by experimental studies, systematic reviews and meta-analyzes. Recently the hypothesis that low levels of vitamin D are responsible for a higher incidence of this pathology has been advanced.
Analyzing the data of the scientific literature to evaluate the hypothesis of a likely correlation between the Vitamin D deficiency and the incidence of Crohn's disease.
By referring to the PubMed database, a review on 16 clinical studies that analyzed the correlation between serum levels of Vitamin D and the incidence of Crohn's disease has been evaluated.
The studies show a high relation between low circulating Vitamin D levels and the active phase of Crohn's disease and strongly suggest that a likely supplementation of Vitamin D would have a strong immunomodulatory effect for this pathology.
Crohn's disease, Vitamin D, Chronic inflammatory bowel disease
Crohn's disease (Cd) falls within the group of nosological entities that take the name of Chronic Intestinal Inflammatory Diseases.
In this group we also find ulcerative rectocolitis (UR) [1-3], undetermined colitis (UC) and, to a minor extent, lymphocytic colitis, ischemic colitis, diversion colitis and Behçet's syndrome.
The etiopathogenic characteristic of IBD is the presence of a chronic inflammatory state in the absence of an infectious cause. Unlike U,R which selectively involves the mucous membrane of the rectum and/or colon, CD can affect any area of the gastrointestinal tract, from the mouth to the anus, although its main clinical manifestations are present at the gastrointestinal level, and its classification is based on the region of the intestine that is specifically affected (Graph 1).
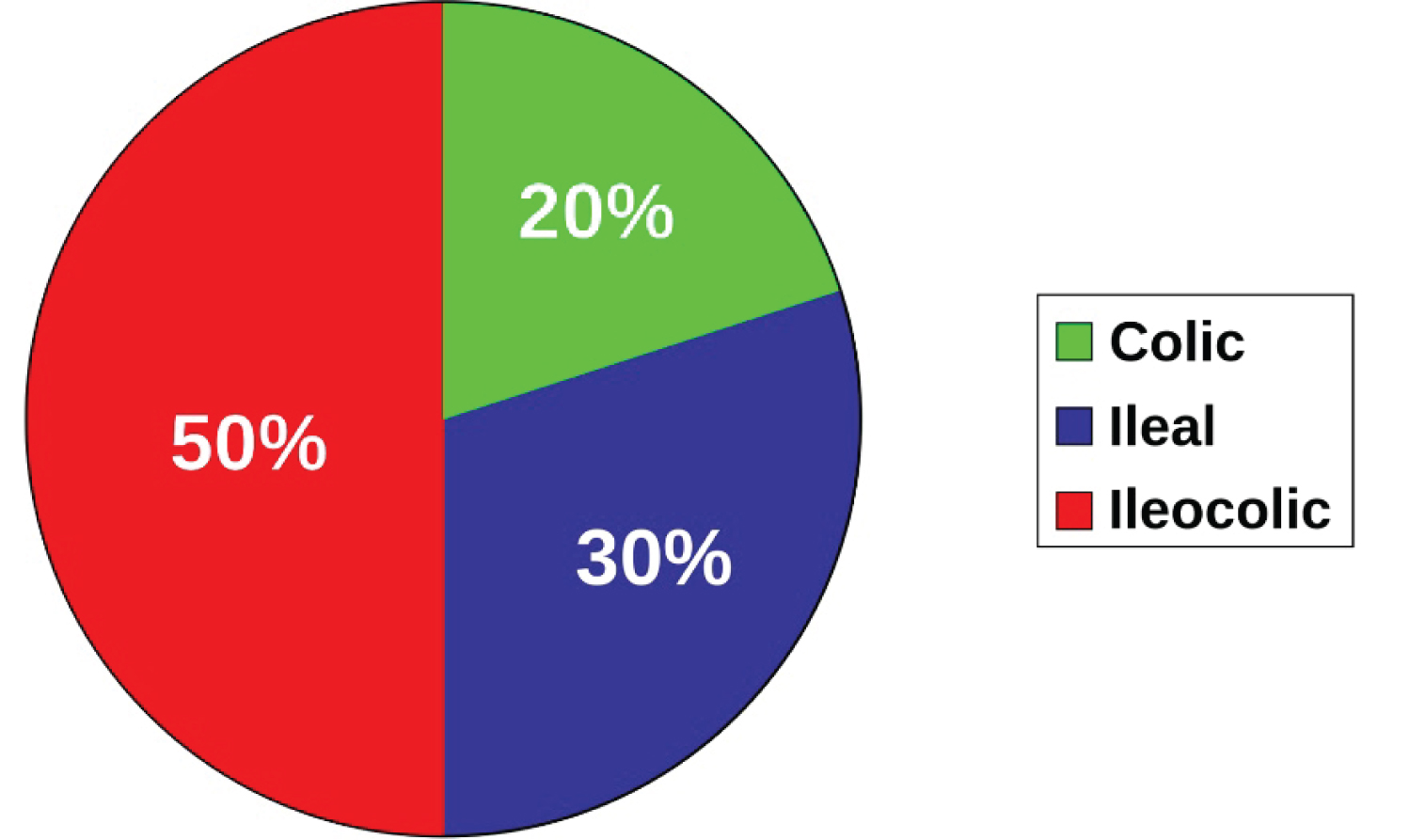 Graph 1: Gastrointestinal distribution of Crohn's disease.
View Graph 1
Graph 1: Gastrointestinal distribution of Crohn's disease.
View Graph 1
50% of cases are classified as Crohn's ileocolic selectively involving the ileum and large intestine. 30% are classified as Crohn's ileite, just affecting the ileum. 20% only involve the large intestine, and are known as Crohn's colitis.
In some cases the latter, due to the affected portion and to the overlap of the clinical picture (Table 1), can make the real distinction between CD and ulcerative colitis inaudible. Hence, when the clinical picture is particularly complex, the diagnosis of undetermined colitis is made [2,4]. In CD, the immune system involves the intestine causing an inflammatory reaction. It can engender a wide variety of symptoms ranging from abdominal pain, diarrhea, vomiting and weight loss. Further complications may also affect other sites and be related to skin rashes, arthritis, eye inflammation, fatigue, and concentration difficulties [2].
Table 1: Symptoms of Crohn's disease compared to ulcerative rectocolitis.3 View Table 1
CD is widespread all over the world, reaching a high degree of prevalence in western nations, with a female/male ratio of 1.35:1. It can occur at any age [2], with a peak between the second and third decade and another one between the sixth and seventh decade.
The etiology is not clear yet, but the hypothesis that the association between environmental and genetic factors is decisive in the development of this disease is prevalent [5].
Having defined the role of genetic factors, and having estimated that the relative risk of developing the disease due to a mutation of the genes is very low (about 1:200), the greatest interest has shifted to environmental factors, currently considered decisive in the manifestation of the CD.
For example, smokers are twice as likely to develop CD than non-smokers [6].
Furthermore, its greater incidence in industrialized countries directs attention to the diet, which according to most authors, is one of the causes of the disease. For example, there is a positive correlation between CD and animal protein consumption and an increase in the omega-6/omega-3 ratio [7], while the relationship with milk proteins is still under debate [8,9]. On the other hand, when the consumption of vegetable proteins resulted greater than that of animal proteins, a reduction in the incidence of the disease was highlighted [8], placing the vegetarian diet among the potential protective factors in the onset of CD.
CD can induce nutritional deficiencies of varying magnitude in acute states, generating the risk of malnutrition due to malabsorption or decreased food intake.
Vitamin D deficiency in DC patients has been widely described by clinical studies [10,11] systematic reviews and meta-analysis [12-14] and recently the hypothesis that low levels of vitamin D may favor the increased incidence of DC onset has been put forward. This review has worked the scientific literature out in order to verify the hypothesis of a pathogenetic relationship between Vitamin D deficiency and incidence of CD. It must be remembered here that an individual's vitamin D patrimony is habitually assessed by determining the plasma concentrations of 25-OH-vitamin D3 (25 (OH) D), i.e. the metabolite of vitamin D3 that is generated in the liver by the 25 hydroxylase.
"PubMed" search engine was used as database for this review. "Vitamin D" and "Crohn's Disease" were used as search keywords, analyzing the works published from 2014 to 2019. Additional sources have been selected from the bibliography of the works obtained.
Trials have been conducted in the last 5 years (from 2014 to 2019), on patients aged 18 or over who had inflammatory and chronic intestinal diseases. The inclusion in the criteria of some studies where there were also Ulcerative Rectocolitis and Indeterminate Colitis has been made to evaluate any differences between the incidence among the various pathologies and the levels of Vitamin D. Both observational studies and those that provided for the administration of Vitamin D have been considered.
The data have been extrapolated from each article and include: Author, date of publication, type of study, place of study, sample analyzed divided by type of pathology (UR, CD, CI) and insertion in the control group. The diagnostic values of hypovitaminosis D, if present, have been reported in ng/mL, to allow accurate comparisons in all studies.
At the end of the data analysis, the most significant conclusions of the various authors have been reported.
Out of the several studies analyzed concerning the correlation between serum levels of Vitamin D and CD 17 the most significant ones have been extrapolated from the database for this review, after a full text analysis and one study has been excluded because it did not fall within the inclusion criteria. The main data of the included studies are shown in Table 2.
Table 2: Inclusion features in the current review. View Table 2
All studies included the impact of Vitamin D serum levels on IBD. In one study, the role of the Vitamin D dosage in improving the clinical picture has also been analyzed in detail.
Inside a transversal study, run between September 2011 and January 2013, Basson, et al. [15] have compared the 25-hydroxyvitamin D 25 (OH)D serum levels of 186 Crohn's disease patients with 199 healthy subjects and have assessed disease activity using the Harvey Bradshaw (HBI) index, which evaluates on a scale the progress of the disease by collecting five exclusively clinical parameters. The various threshold concentrations of 25 (OH)D have also been studied to predict a higher HBI score. The study has found that, if compared to patients with HBI < 5, the cases with HBI ≥ 8 were 2.5 times more likely to have concentrations of 25 (OH) D ≤ 21 ng/mL and that low levels of 25 (OH) D were associated with an increase in CTM activity in a South African cohort.
Branco, et al. [16] have assessed the prevalence and predictive factors of vitamin D deficiency and the possible association with CD activity. The study lasted from January to July 2016. The following Endocrine Society guidelines were considered to define serum 25-hydroxyvitamin D levels: Deficient (< 20 ng/mL, < 10 ng/mL with severe deficiency), insufficient (21-29 ng/mL) and adequate (> 30 ng/mL). In this study 152 patients were enrolled out of which 106 were affected by CD, 44 by RU, and 2 by CI. Average vitamin D levels were 17.1 ± 8 ng/mL, slightly higher in subjects with RU (17.6 ± 7 ng/mL) than in those with CD (16.7 ± 8 ng/mL), but this difference was not statistically significant. Globally, the prevalence of vitamin D deficiency was 68.4% and higher in CD (72%) than in UR (65%), but this difference was not statistically significant. Taking all patients into account, 17.7% had a severe vitamin D deficiency and this prevalence tended to be significantly higher in CD (24%) than in UR (11%, p = 0.06). Inadequate vitamin D levels were present in 90.8% of patients, a very similar percentage in between the two diseases (91 versus 93%, respectively, p = 1). Also in this study it was shown that vitamin D deficiency is widespread in patients with IBD.
In a 3-year retrospective cohort study that included 201 Canadian patients, Alrefai, et al. [17] have assessed the possible association between hydroxyvitamin D [25 (OH) D] levels and DC activity. The clinical data extrapolated from the medical records were: Sex, disease status, any drugs and vitamin D supplementation, previous surgical interventions, Harvey-Bradshaw (HBI) index score and blood test results (c-reactive protein to high sensitivity (Hs-CRP) and 25 hydroxyvitamin D (25 (OH) D)). The HBI score was used as an indicator of disease and patients with a score equal to or greater than 5 were considered to have active disease. The severity of the disease was defined as mild if the HBI score was greater than 5 and less than 7, moderate with an HBI score between 8 and 16 and severe with an HBI score greater than 16.
The study showed that a large number of patients with CD are deficient in vitamin D and have an inflammatory state corresponding to an active phase of the CD.
In patients who received vitamin D supplementation, an association was found between improving the state of vitamin D, and reducing inflammation and DC activity and this allows us to hypothesize that the vitamin has a potent anti-inflammatory and immunomodulating effect. Ye Lingna, et al. [18] retrospectively have reviewed Vitamin D deficiency and disease activity by endoscopy in hospitalized patients from 2014 to 2016. The clinical activity of the disease was assessed by the DC activity index and circulating levels of C-reactive protein. DC activity was determined by a combination of clinical, biochemical and endoscopic evaluation (with an endoscopic score for CD). The CD activity index (CDAI) was calculated for each patient and the severity of the disease was classified into four categories according to CDAI scores, with CDAI < 150 patients in the remission phase, CDAI between 150 and 220 as slightly active, CDAI between 220 and 450 as moderately active ones and CDAI over 450 seriously as active ones. Circulating levels of CRP were defined pathological when they had a level above 5 mg/L. Albumin was considered as an additional index to evaluate disease activity and levels < 35 g/L were considered pathological. Colonoscopy was performed by a gastroenterologist and endoscopic scores were evaluated by an IBD specialist. 25OHD levels were compared in DC patients and 40 control subjects but the two groups were not matched by age, gender and timing of the test. The mean 25OHD serum levels belonging to 131 patients were lower than those in the control group [21.1 nmol/L (11.8-32.3) versus 49.9 nmol/L (44.9-57.4), P = 0007]. 125 (95%) DC patients had vitamin D deficiency and the high (5%) had vitamin deficiency. The results of the study show that the severity of the disease, assessed by CRP systemic inflammation, CDAI and albumin, was strongly and inversely related to 25OHD levels.
The 17-year study by Ho Ko, et al. [19] was also aimed at determining the correlation between vitamin D serum levels and disease activity in patients with IBD. The diagnosis of RU or DC was formulated on the basis of the diagnostic guidelines suggested by the IBD study group of the Korean Association for the study of intestinal diseases [19]. Clinical information on patients, including duration, location and course of disease and any IBD-related and surgical procedures, was obtained by consulting the medical records. Anthropometric data were collected and circulating levels of 25-OH-vitamin D, hemoglobin, white blood cells (WBC), C-reactive protein (CRP), albumin and cholesterol were simultaneously defined as indicators of inflammation and disease severity. The medical history of the drugs used since the time of diagnosis was taken into accounts. Disease activity was assessed using the partial Mayo score (which uses the three non-invasive components of the full Mayo Score: Evacuation frequency, rectal bleeding, and specialist's overall judgment) for HR and the Harvey-Bradshaw index (HBI) for CD. Vitamin D deficiency was defined according to vitamin D levels < 20 ng/mL and was found in 73.6% of patients with IBD (UR, 73.3%; CD, 73.8%).
IBD patients showed lower average vitamin D levels (16.3 ± 9.0 ng/mL) than the control group (20.4 ± 7.0 ng/mL), with no statistically significant differences (P = 0.136). The average vitamin D level of CD patients was lower than that of RU patients, but not statistically significantly (15.4 ± 8.2 ng/mL versus 17.1 ± 9.7 ng/mL, P = 0.640). IBD patients had a higher incidence of vitamin D deficiency than the general population. Patients with CD and low levels of vitamin D were observed to have significantly higher disease activity, measured by HBI. However, this association has not been observed in patients with UR.
76 patients were enrolled in the Dias De Castro, et al. [20] study, 19 with UR (25%) and 57 with CD (75%). All withdrawals were made during the summer months (July and August 2013). The status of vitamin D was determined by measuring serum 25 (OH) D. Demographic data, duration and degree of disease, established according to the Montreal Classification, which divides patients according to disease diagnosis age (A1 with onset under 16 years; A2 with onset between 17 and 40 years; A3 with onset over 40 years), the location of lesions (ileal L1, colic L2, ileocolic L3, L4 in the upper part of the intestine; L4 in association or not with other locations, e.g. L1-L4, L2-L4 etc), the course of disease (inflammatory B1; B2 stenosing; B3 fistulizing and the presence of perianal disease, both for CD than for UR) and IBD-related surgery. Circulating levels of CRP, ferritin, albumin, ESR and hemoglobin were also measured as markers of inflammation and disease severity. Overall, 68% of all patients had insufficient vitamin D levels (58% of patients with HR and 72% of patients with CD) and 30% were deficient in vitamin D (< 20 ng/mL). In all patients the mean 25 (OH) D serum level was 26.0 ± 10.0 ng/mL, and patients with CD had significantly lower levels than patients with RU (24.6 ± 8.0 vs. 30.0 ± 12.5 ng/mL, P = 0.032). However, there was no significant difference in the prevalence of vitamin D deficiency between patients with CD and those with UR (P = 0.313). The results of this study show that vitamin D deficiency is common in patients with IBD even when the disease is managed on an outpatient basis and remains high even in the summer. In this study all samples were collected in the summer to reduce the influence of lack of UV exposure in our data, suggesting that the observed low levels of vitamin D were not the result of low levels of sunlight.
Venkata, et al. [21] have analyzed data from 880 CD patients observed in an IBD center recruited from 2000 to 2014 and followed for at least one year. Enrolled subjects were 19+ and had data on vitamin D levels that were measured in 196 of the 880 patients with CD observed in this study. Of these, 115 had a low vitamin D level and 81 had an adequate vitamin D level. Among patients with CD, the incidence of hospitalization for CD-related exacerbation was 30.18% among those who had levels average low in vitamin D and 14.19% among people with appropriate average levels of vitamin D. In particular, patients with CD and low average levels of vitamin D (< 30 ng/mL) were 1.5 times more likely to be hospitalized than those with adequate vitamin D levels. Overall, the probability of hospitalization in hospital related to CD decreased by about 3% due to the increase of one unit (ng/mL) of the average levels of vitamin D. The results could have some plausible interpretations: Firstly that vitamin D can serve as a marker of the severity of CD in terms of general status and, second, that patients with CD may have a higher chance of being hospitalized if they have low levels of vitamin D, despite the same degree of activity of CD as those with adequate levels of vitamin D.
In the retrospective study of Pallav, et al. [22], 237 patients with IBD (139 CD, 98 UR) and 98 patients admitted as a control group were identified. Patients were recruited between July 2012 and July 2015 by sing various diagnostic codes for UR, CD and IBD. Demographic, biometric and clinical information was collected through the review of electronic medical records. IBD diagnosis was based on endoscopic, clinical and histological data. Only patients with IBD who had plasma 25 (OH) D data were enrolled. Bivariate analysis identified the following risk factors for vitamin D deficiency: (1) DC; (2) BMI > 30 kg/m2; (3) Age < 35 years. However, regression analysis showed that only subjects with BMI > 30 kg/m2 had a significant association with vitamin D deficiency. This is a modifiable risk factor due to lifestyle change (diet and exercise), yet it can influence the severity of the disease in IBD patients owing to a pro-inflammatory effect of obesity itself and to vitamin D seizure by adipose tissue [23,24].
In Torella, et al. [25] study, patients with CD and UR were consecutively enrolled from June 2014 to January 2016. Asymptomatic individuals were also enrolled by returning them as a control group. Both cases and controls were subjected to blood sampling to determine serum levels of vitamin D3 and a threshold value of 30 ng/mL was considered as a cut-off below which the vitamin D deficiency was defined. Vitamin D3 levels were compared between the study and control groups and the percentage of patients with IBD and thus, vitamin D deficiency was estimated. In patients with IBD, simultaneously with the determination of vitamin D, the following variables among patients with and without vitamin D deficiency were compared: Age, sex, distribution and duration of disease, smoking, need for biological therapy, steroid therapy, need for hospitalization at diagnosis, and clinical severity. For clinical severity, the CD index (CDAI) or the Mayo score were used: Moderate to severe disease was defined as a CDAI > 220 and a Mayo score > 6. From June 2014 to January 2016 59 patients diagnosed with CD or UR and 56 healthy controls were consecutively enrolled. The average age was 41 years (19-79) and 56% (n = 33) were male. Overall, 76.27% (n = 45) had a diagnosis of UR and 23.73% (n = 14) of CD. Vitamin D deficiency was observed in 66.1% (n = 39) of IBD patients compared to 21.42% (n = 12) of healthy controls (OR 7.15 (3, 116.48), p 0.001). The mean vitamin D values were 23.5 ± 9.3 IU/mL and 38.5 ± 7.6 IU/mL, respectively (P < 0.05). The study confirmed the increased prevalence of vitamin D deficiency among IBD patients and its association with some features that show disease activity and severity.
Kojecky, et al. [26] collected data from 167 vitamin D deficiencies between January 2013 and April 2015. Some had been taking vitamin D supplements for 3 months before determining vitD, while others had not taking vitD and were considered as a control group. Exclusion criteria included conditions that could influence serum vitD levels such as kidney failure, liver and cholestatic disease, malabsorption, celiac disease, anticonvulsant treatment, pregnancy, gastrointestinal surgery and/or any other serious disease. Disease activity for Rectocolitis was determined using a partial Mayo score, where the score ≥ 3 was considered to define clinically active disease. In the case of CD, activity was assessed using the CD activity index (CDAI), and the disease was defined clinically active with a score of ≥ 150. At the patient's visit, blood samples were taken to determine CRP, alkaline phosphatase (ALP) and vitamin D. Blood samples were obtained in late summer (September-December) and late winter (January-April). This prospective cohort study showed that varying degrees of vitamin D deficiency were common in patients with IBD.
The study could suggest that vitamin D has a protective effect and that low levels of vitamin D are likely to be a risk factor for surgery and hospitalization in patients with IBD.
Zhao, et al. evaluated the vitamin D serum levels of 65 patients with UR, 50 patients with CD and 120 healthy patients (control group) in one study [27] conducted between January 2015 and December 2016. The data emerged show that the Vitamin D serum levels in patients with UR and CD were significantly lower than those in the control group. (P < 0.05); moreover, in both study groups, vitamin D levels were significantly lower in the acute and moderate stages of the disease. These data are in line with studies carried out in other populations affected by IBD and confirm that vitamin D plays a key role also in the management of the disease, indicating, however, that the reduction of vitamin D levels may aggravate the symptomatology of the disease [17].
Also in a prospective study, conducted in Romania by Dumitrescu, et al. [28] from March 2011 and June 2012 in 47 IBD patients, it was shown that only 24% of patients with UR and 21% of patients with CD had sufficient levels of vitamin D (> 30 ng/mL). Levels of this vitamin were significantly low in the percentage of patients who had moderate to severe disease symptoms.
In the longitudinal retrospective study of Lopez-Munoz, et al. [29] the association between vitamin D levels and inflammatory markers and clinical disorders in a Spanish population suffering from IBD were sought. Participants in this study were divided into three groups based on their measured vitamin D serum levels: 1) Severe deficit (SD) corresponding to vitamin D levels < 15 ng/mL; 2) Moderate deficit (DM) corresponding to vitamin D levels between 15 and 30 ng/mL; 3) Sufficient (S) corresponding to vitamin D levels greater than 30 ng/mL. The clinical activity of the disease was also assessed (exacerbations, hospitalizations, visit times to the IBD clinic, increasing treatment, use of steroids) in the six months preceding and in the six months following monitoring, and inflammatory markers were determined (CRP, FC and fi brinogen (FBG)). Study results revealed that low serum vitamin D levels are associated with intestinal and systemic inflammation in patients with IBD. In these patients, vitamin D deficiency was associated with a higher incidence of hospitalizations, exacerbations of the disease and the need to resort to steroid drugs for the treatment of symptoms.
Hausmann, et al. assessed the correlation between low Vitamin D levels and disease activity in a retrospective study [30]. The 2-year study (January 2017 to December 2018) recruited a total of 470 patients with IBD (including 272 with CD and 198 with UR). At the time of enrollment, serum levels of vitamin D were determined. The study showed that 60.2% (equal to 283) of the patients appeared to have insufficient levels of vitamin D (10 to 29 ng/mL). In addition, other clinical and laboratory variables that measured disease activity were measured using the Harvey-Bradshaw Index (HBI) and the Simple Clinical Colitis Activity Index (SCAAI), a questionnaire used to assess the severity of symptoms in patients, with a score ranging from 0 to 19, obtained by analyzing the frequency and urgency of defecation, the presence of blood in the stool, the general health of the patient and extra-colon manifestations; the diagnosis of disease activity is formulated with a score of 5 or higher. The vitamin D supplementation regimen and patient characteristics were also evaluated. Patients were visited at the discretion of the attending physician, but at least every six months in order to monitor IBD treatment. Vitamin D serum levels were subsequently monitored every 12 months. 256 patients (53.6%) received vitamin D supplementation (mainly 20000 IU of cholecalciferol once a week and in some cases 1000 IU of cholecalciferol per day), and in 112 (45.7%) patients a relative deficiency of vitamin D was still found, despite the supplement. Overall, in patients treated with supplementation, the serum vitamin D concentration was significantly higher (31 ng/mL) than in patients without integration (22 ng/mL (p < 0.0001). Interestingly, the average serum levels of 25 (OH) D3 were significantly lower in patients with active disease than in subjects in remission (23 ng/mL (4-75) versus 29 ng/mL (3-100), p = 0.04) suggesting that the Vitamin D supplementation should be proposed in patients with IBD who experience a deficiency.
Olmedo-Martí, et al. [31] assessed the relationships of the 25-hydroxyvitamin D deficiency in a cross-sectional study carried out in a cohort of 224 Spanish patients (74 in total with UR and 150 CD), aged 18+ and with a positive diagnosis of IBD; the subjects were enrolled after completing a clinical questionnaire (quality of life and symptoms) and taking a blood sample. At the time of inclusion of the study, clinical activity indices were calculated according to the Montreal classification. Laboratory measurements included parameters routinely used for outpatient follow-ups in addition to the determination of 25OHD. Patients with 25OHD levels < 20 ng/ml were considered deficient, those with 20-29.9 ng/ml levels as insufficient and those ≥ 30 ng/ml sufficient. The season in which the withdrawal was made was also noted; the winter period was considered from November to April and the summer period from May to October. Clinical activity was assessed using the Harvey-Bradshaw (HBI) index for patients with CD, and the partial Mayo score for patients with UR. The prevalence of vitamin D deficiency in CD and HR was 33.3% and 20.3% respectively. In Crohn's disease, vitamin D deficiency was associated with increased clinical activity (p < 0.001) and a higher concentration of faecal calprotectin (p = 0.01), which indicates the presence of ongoing inflammation. In ulcerative colitis, the deficiency was associated with the clinical activity of the disease (p < 0.001), the need to resort to drug therapy in the past six months (p = 0.001) and hospitalization in the previous year (p = 0.003).
In the study by Limketkai, et al. [32] carried out between 1998 and 2011, the association between vitamin D and CD levels was assessed in an American population represented by 480 patients (240 affected by DC and 240 included in the control group), to whom a sample was collected on in 3 different times: pre-2: 8-3 years; pre-1 from 3 years to 3 months before, pre-0 3 months before up to 21 months after diagnosis. These 3 times served to evaluate the course and correlation of vitamin D levels in CD. Vitamin D levels were classified as sufficient (≥ 30 ng/mL), insufficient (20 to 30 ng/mL) and deficient (≤ 20 ng/mL). Statistical regression analysis revealed that vitamin D levels before diagnosis were not associated with CD in the pre-2 period (P = 0.65) and in the pre-1 period (trend P = 0.84). However, there was an inverse correlation between CD and tertile higher than the vitamin D level in post-diagnosis samples (P = 0.01).
The association between circulating levels of vitamin D and CD in the small intestine is now largely clear, while the possible role of intestinal malabsorption of vitamin D introduced with food and CD has not been defined yet However, it should be remembered that although some dietary models induce an increase in circulating levels of vitamin D, such as the Mediterranean diet [33], the main source of circulating levels of the vitamin is tied to skin production. However, the role exercised by vitamin D in immunomodulation is evident, as hypothesized in the case of autoimmune thyroiditis, and its administration could be useful in a variety of pathologies, including IBD. It is good to remember that seasonal changes significantly affect cholecalciferol production and that vitamin D deficiency is more common during the winter period, because ultraviolet B radiation (UVB) is not intense enough to produce adequate vitamin D. Some Studies show that lack of sunlight exposure can be an important cause of vitamin D deficiency in IBD patients, particularly in northern climates, demonstrating an association between the winter season and vitamin D deficiency due to low light solar and UV-B exposure. The sedentary lifestyle of patients with chronic disease can also be an additional risk factor associated with vitamin D deficiency. It has also been found that intestinal resection is associated with vitamin D deficiency due to the suspension of enterohepatic circulation in the terminal ileum, by stopping the absorption of fat-soluble vitamins such as vitamin D.
The vast majority of studies have been conducted in geographic areas where both vitamin D deficiency and IBD incidence are relatively high; this could lead to a likely miscorrelation, an error that has been overcome by studies conducted in geographic locations where sun exposure - and consequently, vitamin D levels - are higher. Yet there is a relative lack of studies conducted in places with mild temperatures such as South American countries. Vitamin D is known to play a significant role in controlling phosphocalcic metabolism; its deficiency is a key component of osteopenia and osteoporosis - common pathology in patients with IBD.
Eventually recent studies indicate other key functions of vitamin D, such as anti-inflammatory, antiproliferative and anti-apoptotic functions. Vitamin D can modulate the adaptive and innate immune response thanks to its influence on T and B lymphocytes, as well as on the function of dendritic cells and macrophages: these cells can express vitamin D receptors on their surface, which can bind cholecalciferol and 25 (OH) - cholecalciferol and transform them into 1.25 (OH) -colecalciferol, an active metabolite with autocrine and paracrine actions. Vitamin D3 has been shown to suppress the Th1 lymphocyte response, leading to a decrease in the excretion of pro-inflammatory cytokines such as interferon γ, interleukin-2 and tumor necrosis factor α. In addition, vitamin D inhibits the differentiation of dendritic cells; these can induce the conversion of cholecalciferol 25-OH into 1.25 OH-cholecalciferol, which in turn helps to promote monocyte differentiation and CD4 + inhibition. A large number of CD patients are deficient in vitamin D and suffer from degrees of inflammation. Inflammation keeps CD active. All these data are in line with the finding that vitamin D deficiency is associated with increased disease activity in patients with CD. In conclusion, vitamin D deficiency is frequent in patients with IBD and therefore adequate screening and supplementation with adequate amounts of vitamin D in patients with IBD may be helpful. Among subjects with CD, serum levels of vitamin D must be assessed especially in those with long duration of CD (> 15 years) and it must be considered that the active vitamin D provided orally is well absorbed even in the presence of distal resection of the small intestine [34].
The authors declare no conflict of interest.