In this study, we describe our experience in the treatment of malignant rhinosinusal tumors and establish factors related to their prognosis.
To determine the local control and the survival rates in patients with malignant tumors of the paranasal sinuses and nasal cavity treated by endonasal endoscopic surgery.
Descriptive and prospective.
All patients who had malignant tumors of the nasal cavity and paranasal sinuses who were treated by an endonasal, cranionasal or combined endonasal an external approach in the ENT Department of the Italian Hospital of Buenos Aires from March 2003 to August 2019 were selected. Patient data were collected prospectively and updated by reviewing electronic medical records.
Thirty patients were treated, 10 had tumors located in the nasal cavity. No patient had local recurrence.
Twenty had malignant tumors originated in the paranasal sinuses. Twelve endonasal approaches were performed with endoscopes only, 9 had adjuvant treatment with radiotherapy and chemoradiotherapy. The local control rate was 50% (6/12).
Six cranionasal approaches were made: All had adjuvant treatment with radiotherapy or chemoradiotherapy and two others were treated by an endonasal and external approach, and postoperative radiation therapy.
The local control rate in patients treated with cranionasal and combined approaches was 75%.
The rate of local control and survival that we obtained in patients treated for rhinosinusal malignant tumors by endonasal endoscopic surgery was 73.33%. Tumors with greater extension and infiltration, with higher T staging, localization in the paranasal sinuses and unfavorable histologies such as undifferentiated carcinoma, had a greater need for neoadjuvant or adjuvant treatment and worse prognosis than those small, T1-2, and localized neoplasms in the nasal cavity.
Endoscopic, Endonasal surgery, Malignant tumors, Paranasal sinuses, Nasal cavity, Cranionasal approach
Malignant rhinosinusal tumors are rare and the histologies can be diverse.
Some histological types imply a biological behavior that affects the prognosis, in addition to other factors such as the extension and location of the neoplasms.
According to the factors mentioned above, the treatments may be different, and include surgery, radiotherapy and chemotherapy as the only modality or in combination, and with different sequences.
The first reports on the possibility of resecting rhinosinusal neoplasms using an endonasal approach with endoscopes alone [1] or combined with a craniotomy [2,3] occurred in the late 1990.
Surgery for malignant tumors has evolved in the last 20 years and the endonasal approach with endoscopes alone or combined with a craniotomy in cases of extensive dural infiltration and intracranial involvement has demonstrated its efficacy [4,5] and its lower morbidity when indicated in selected patients.
To determine the local control and survival rates in malignant tumors of the paranasal sinuses and nasal cavity treated by endoscopic endonasal surgery.
All patients who had malignant tumors of the nasal cavity and paranasal sinuses, and who were treated by an endonasal approach with endoscopes alone, or combined with an external approach with intention to cure in the Otorhinolaryngology service of the Hospital Italiano de Buenos Aires from March 2003 to August 2019 were selected.
The study was approved by the ethics committee of the Hospital Italiano de Buenos Aires.
Patient data were collected prospectively since 2003 and updated by reviewing electronic medical records.
The patients were evaluated by nasal endoscopy, computed tomography (CT) and magnetic resonance imaging (MRI).
In some, a brain, neck, chest, abdomen and pelvic tomography or a positron emission tomography (PET) scan was requested.
A preoperative biopsy was performed or in some patients with tumors located in the nasal cavity or in small ethmoids tumors an intraoperative endonasal biopsy was performed to diagnose malignancyand in the same surgical time, the oncological resection was carried out.
Malignant tumors originating from the epithelium of the paranasal sinus mucosa and nasal cavity were staged or re-staged according to the TNM classification of the AJCC, 8th edition, as well as mucosal melanomas, and esthesioneuroblastomas according to the Kadish classification.
The indicated treatments emerged from the discussion in the tumor committee Surgical approaches were endonasal or combined: Cranionasal and endonasal plus an external approach.
0° and 30° endoscopes, with full HD endocamera, conventional instruments for endoscopic sinus surgery, microdebrider, and in some neuronavigation systems were used.
Endonasal surgery for nasal cavity neoplasms consisted in a bloc orparts resection, and intraoperative histopathological confirmation that the resection margins were tumor free.
In paranasal sinus tumors, a wide maxillary antrostomy, anterior and posterior ethmoidectomy, sphenoidotomy and a Draf III frontal drainage were performed by the endonasal approach, depending on the extent of the neoplasm. In some, the inferior turbinate and part of the nasal septum were resected.
The cranionasal approach was performed in conjunction with the neurosurgery team when tumors invaded the skull base and consisted of performing a bicoronal incision and an anterior craniotomy together with the endonasal approach with endoscopes (described above) in the same surgical time. Repair of the skull base was performed with flaps.
The combined approaches (endonasal and external) were used in patients with facial skin invasion and in patients with tumors that compromised the external table of the frontal sinus.
In some patients with tumors that eroded the lamina papyracea of the orbita resection of this and the periorbita was made to obtain a greater margin without disease.
In all of them after oncological resection the margins were controlled by freezing biopsies.
Hospitalization was in an intensive or medium care unit (cranial surgery or patients with comorbidities) or in a common room.
The controls were carried out by means of a clinical otolaryngological examination, nasal endoscopy, CT, MRI, and PET.
They were done in conjunction with clinical oncology (Table 1, Table 2 and Table 3).
Table 1: Malignant tumors of the nasal cavity: Endonasal approach with endoscopes. View Table 1
Table 2: Malignant tumors of the paranasal sinus: Endonasal approach with endoscopes. View Table 2
Table 3: Malignant tumors of the paranasal sinuses: Cranio-Nasal surgery and combined approach (Endonasal and External). View Table 3
Thirty patients were treated for malignant tumors of the nasal cavity and paranasal sinuses by endonasal endoscopic surgery, cranionasal approach with endoscopes and combined: Endonasal and external approach.
23 patients were men and 7 women, the youngest was 5-years-old and the oldest 90-years-old, and the average age was 55 years.
Ten had tumors located in the nasal cavity, six originated in the nasal septum, three in the inferior turbinate and one in the floor of the nostril. The histologies were heterogeneous: Angiosarcomas (2/10), squamous cell carcinoma (2/10), melanoma (2/10), adenocarcinomas (2/10), clear cell renal adenocarcinoma metastases (2/10).
The two nasal septum carcinomas were staged T1N0M0.
All patients were men and the mean age was 57.5 years.
The most frequent reasons for consultation were unilateral nasal obstruction and epistaxis. All were treated by an endonasal approach with endoscopes with intraoperative control of the resection margins.
Free margins at resection were obtained in all patients and were confirmed by the delayed histopathological study.
There were no intra or postoperative complications.
Neo-adjuvant or adjuvant with chemo and/or radiotherapy was not indicated in any patient.
The local control and specific survival rate were 100%.
Two patients with metastases from a clear cell renal adenocarcinoma had distant disease (lung and abdomen) and another with melanoma had a single metachronous brain metastasis that was treated with surgery and then systemic metastases during the 8-year follow-up.
The mean follow-up time was 8 years, with three patients controlled for 1 year (Figure 1).
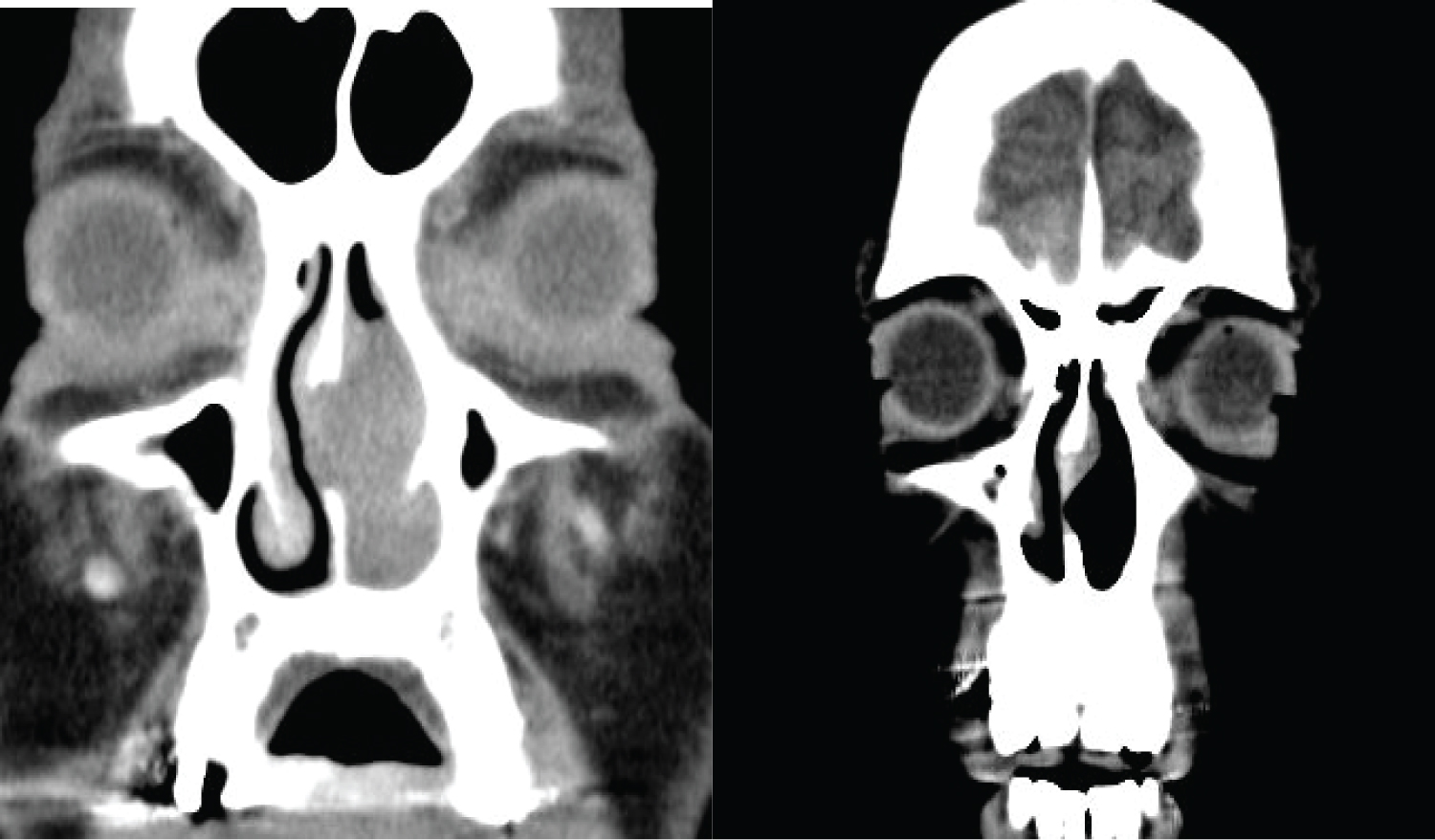 Figure 1: Melanoma of nasal cavity: Endonasal endoscopic resection (A) Preoperative CT; (B) Postoperative CT.
View Figure 1
Figure 1: Melanoma of nasal cavity: Endonasal endoscopic resection (A) Preoperative CT; (B) Postoperative CT.
View Figure 1
Twenty patients had malignant tumors originating from or involving the paranasal sinuses. Twelve mainly affected the ethmoid, four the sphenoid, two the frontal sinus, one the maxilla, and one maxilla and ethmoid.
The most frequent histologies were: Undifferentiated carcinoma (5/20), esthesioneuroblastoma (4/20), squamous cell carcinoma (3/20), melanoma (2/20), low and moderate grade adenocarcinoma (2/20), spindle cell sarcoma (1/20), hemangiopericytoma (1/20), medulloblastoma (1/20), and single abdominal neuroblastoma metastasis (1/20).
Paranasal sinus carcinomas were staged T4a (6/8), T3 (1/8), T2 (1/8) and all were N0 and M0. Three esthesioneuroblastomas were classified Kadish C and one Kadish A.
Fourteen were men and six women, the average age was 52.04 years.
The most frequent reason for consultation was nasal obstruction.
Twelve endonasal approaches were made with endoscopes.
In patients with neoplasms originating in the sphenoid sinus, it was uncommon to obtain free margins at resection and they received adjuvant therapy.
One patient with an epidermoid carcinoma located in the posterior wall of the maxillary sinus and another with a low-grade ethmoid adenocarcinoma underwent surgery on two occasions. The first one underwent postoperative radiotherapy. In both, local control of the disease was obtained.
Of the ten remaining patients in this group, three underwent radiotherapy, three underwent chemoradiotherapy, and one postoperative chemotherapy. One had a previous surgery and preoperative chemoradiotherapy and in another two, only surgery was used.
Two patients died while undergoing adjuvant chemoradiotherapy.
Local control was obtained in 6 patients (50%), the average follow-up was 4.16 years (two had a follow-up of 1 year). The specific survival was 50%.
There were no intra or postoperative complications (Figure 2).
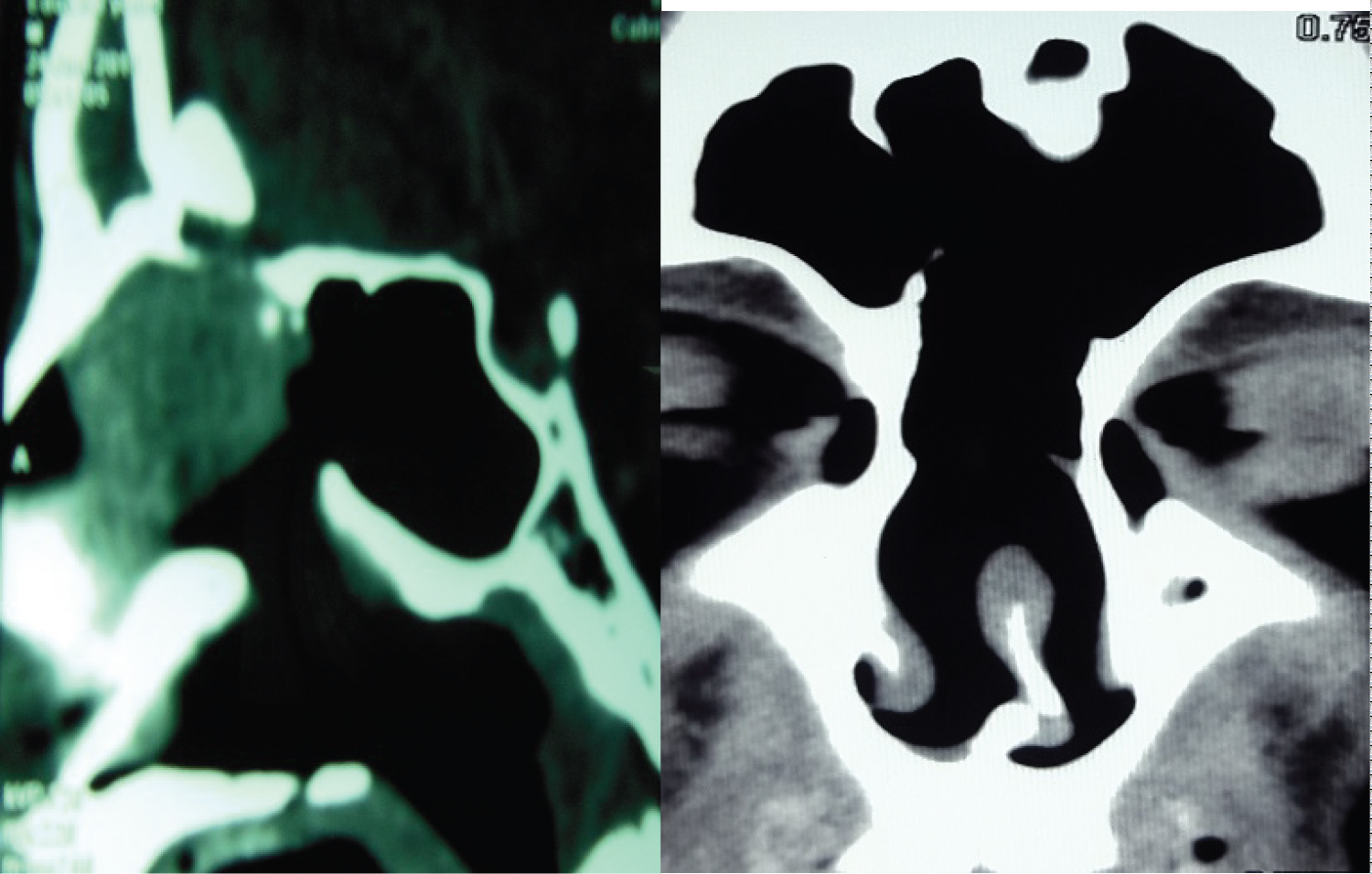 Figure 2: Ethmoid undifferentiated carcinoma: Endonasal endoscopic approach (Lothrop modified, ethmoidectomy and sphenoidotomy) (A) Preoperative CT; B) Postoperative CT.
View Figure 2
Figure 2: Ethmoid undifferentiated carcinoma: Endonasal endoscopic approach (Lothrop modified, ethmoidectomy and sphenoidotomy) (A) Preoperative CT; B) Postoperative CT.
View Figure 2
Six cranionasal approaches were performed: Three for Kadish C esthesioneuroblastomas, one of them recurred to craniofacial surgery and chemoradiotherapy, two for undifferentiated T4- carcinomas, and one for meningoblastoma recurred to surgery and chemoradiotherapy.
All had neoadjuvant or adjuvant treatment with radiotherapy or chemoradiotherapy. Four had local control of the disease (66.66%) with an average follow-up of 5.75 years. Two of the esthesioneuroblastomas had regional disease without local persistence, 4 and 9 years after initial treatment.
Two died with local persistence and systemic metastases.
Three had complications: Pneumocephalus, postoperative cerebrospinal fluid fistula that was repaired with a nasoseptal flap (history of craniotomy and adjuvant treatment for meningoblastoma), and infection of the bone plate of the craniotomy that required its extraction (Figure 3).
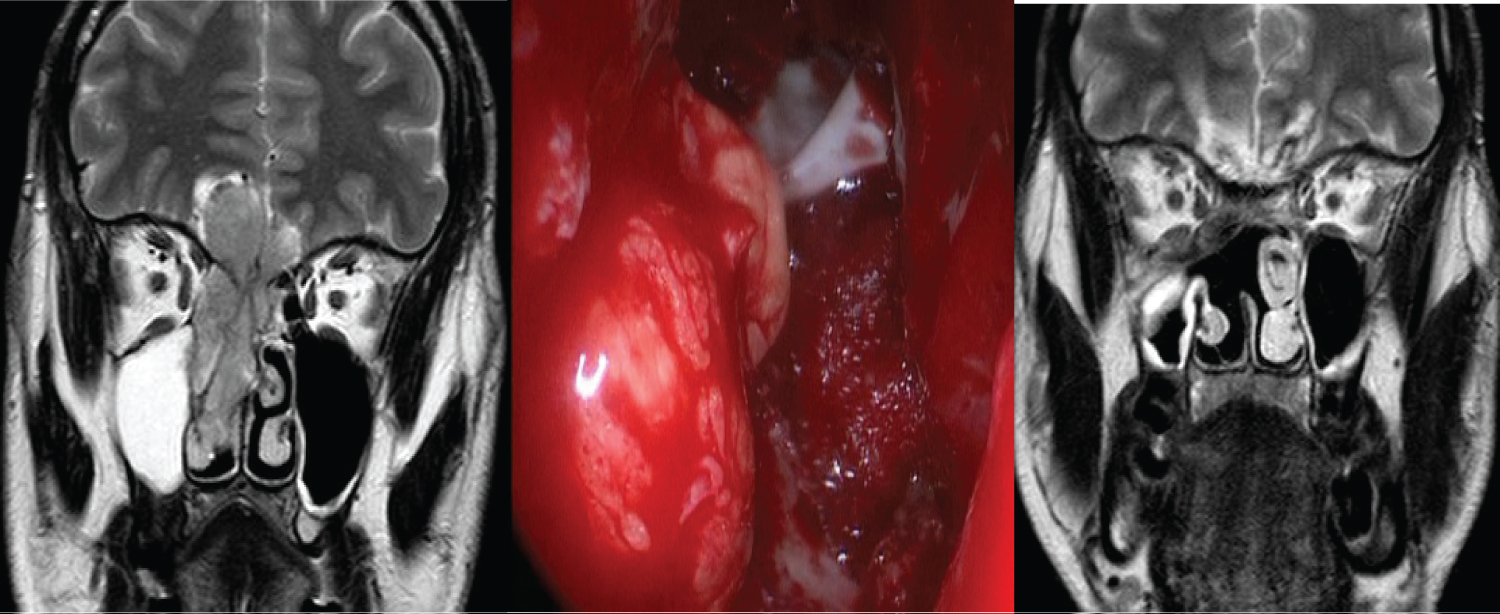 Figure 3: Esthesioneuroblastoma Kadish C: Cranionasal approach (A) Preoperative MRI; (B) Endoscopic vision of skull base and periorbit resection with orbital fat extrusion; (C) Postoperative MRI.
View Figure 3
Figure 3: Esthesioneuroblastoma Kadish C: Cranionasal approach (A) Preoperative MRI; (B) Endoscopic vision of skull base and periorbit resection with orbital fat extrusion; (C) Postoperative MRI.
View Figure 3
Two patients were treated with combined approaches: Bicoronal and frontal drainage type Draf III and ethmoidectomy for a squamous cell carcinoma of the frontal sinus and another through an endonasal approach with endoscopes (resection of the skull base and periorbit) plus a resection of the infiltrated facial skin by melanoma and reconstruction of the defect with regional flaps.
They both received postoperative radiotherapy.
There was a late complication of the surgery: Extrusion of the titanium plate used to reconstruct the anterior table of the frontal sinus 3 years after the operation, which required its removal.
In one, local control of the neoplasm was obtained with a 4-year follow-up, and in another, no local disease was evidenced for 1 year and no return to control.
The local control and specific survival rate in patients treated with cranionasal surgery or combined approaches plus adjuvant or neoadjuvant treatment with radiotherapy or chemoradiotherapy was 75%.
The local control that we obtained in the 30 patients treated for rhinosinusal malignancies was 73.33% and the specific survival rate was also 73.33%.
If we group the patients treated in this study according to the extent and T of the neoplasms, the local control and survival rates were different.
In the fourteen patients (46.66%) with tumors of the nasal cavity and paranasal sinuses of little extension and T1-2, the local control rate that we had was 92.86% and in the most extensive, T3-4, and Kadish C it was 56.25%.
Malignant tumors of the nasal cavity and paranasal sinuses are rare, accounting for 3% of malignant head and neck tumors and less than 1% of all cancers [6].
The most common malignancy is squamous cell carcinoma (44-51%), followed by adenocarcinoma (11%). Other malignant tumors such as those originating in the minor salivary glands, undifferentiated carcinoma, esthesioneuroblastoma and sarcomas are very rare [1,8].
The histologies of rhinosinusal malignancies are heterogeneous, and only this factor can determine a particular biological behavior of less or greater aggressiveness.
The most frequent location is in the maxillary sinus (60%), followed by the nasal cavity (20%) and the ethmoid (10-15%) [9]. Tumors originating in the sphenoid sinus represent 1 to 2% and in the frontal sinus they are very rare (0.3%) [10].
In our study, there was no histological predominance in tumors located in the nasal cavity, undifferentiated carcinoma predominated in paranasal sinuses, followed by esthesioneuroblastoma and squamous cell carcinoma. The most frequent origin was the ethmoid.
We had a higher incidence than reported [10] of malignant tumors located in the sphenoid (4/30: 13.33%) and in the frontal sinus (2/30: 6.66%).
Nasal cavity tumors were diagnosed early and had little extension, possibly due to the early appearance of signs and symptoms such as nasal obstruction and epistaxis that made the patients consult quickly, in contrast to paranasal sinus neoplasms, which were diagnosed at a more advanced stage and involved several subsites.
The low frequency of these tumors and the histological diversity make it difficult to find homogeneous series in the literature to establish therapeutic consensus.
The treatment of these neoplasms usually includes surgery, but it is more frequent that in advanced tumors the treatment is multimodal, with neoadjuvant or adjuvant radiotherapy or chemoradiotherapy.
Surgical treatment has evolved and appropriate cancer resections can be performed in selected patients using endonasal approaches with endoscopes or in combination with craniotomies or other external approaches.
Changes in some concepts such as the fact that it is not essential to perform bloc resections, but rather that the tumor can be excised in parts, the need to identify the implantation site of the neoplasm to be oncologically aggressive in that sector, and the possibility of obtaining margins free after removal of the tumor by the endonasal approach, have made it possible to perform oncological resections with the assistance of endoscopes.
Regarding to bloc resections, Mc Cutcheon, et al. [11] from the Anderson Cancer Center in a study where they compared the results of patients with malignant paranasal sinus tumors treated with a craniofacial approach to the anterior skull base and those treated only with a transcranial resection, mentioned "that as the tumor was resected in parts, the possibility of persisting microscopic residual disease was significant, and the ideal of a wide and en bloc resection was rarely achieved".
More important than achieving an en bloc resection is obtaining negative surgical margins. Wellman, et al. [12] treated 30 patients with craniofacial surgery for malignant tumors of the paranasal sinuses.
In 16 patients they performed an en bloc resection and in 14 the resection was in parts. They did not report differences in survival between the two groups, this was related to the presence or not of positive margins.
In another study, the state of the surgical margin was an independent prognostic factor in the multivariate analysis, as was the histology of the tumor and the presence of intracranial extension [13].
Torabi, et al. [14] reported the factors that were associated with positive margins after oncological resections for T1 to T4 staged rhinosinusal squamous cell carcinomas. They retrospectively studied 2968 cases, of which 807 (27.2%) had positive margins.
In the multivariate analysis, the factors associated with a positive margin were: advanced T (T4 vs. T1), less differentiated tumors (poorly differentiated vs. well differentiated carcinoma) and tumors located in the ethmoid (ethmoid vs. nasal cavity).
There was no association between positive margin and external or endonasal approach with endoscopes.
Few studies report the results of the treatment of malignant nasal cavity tumors. Most series include them together with paranasal sinus tumors.
In one study [14], nasal cavity tumors were considered a factor associated with obtaining negative margins after resection, as was T1 staging.
Hanna [15] reported the results of 120 patients treated for rhinosinusal malignancies of different histologies with endonasal endoscopic surgery only (93: 77.5%) and cranionasal approach with endoscopes (27: 22.5%).
52% of the tumors originated in the nasal cavity and 28% in the ethmoid. 63% of the patients were treated with endonasal surgery with endoscopes for T1-T2 tumors and only surgery was used in 50%.
The local, regional and distant recurrence they had was 15%, 6% and 5% respectively, and the specific survival at 5 and 10 years was 87% and 80%.
52% of the tumors located in the nasal cavity and the low T stage could explain the high rates of specific survival obtained.
In our study, malignant tumors of the nasal cavity represented 33.33% of the total.
There was no predominant histological type and all tumors had a limited extension to a single site of the nasal cavity without compromising paranasal sinuses, skull base or orbit.
Tumor-free margins were obtained in all resections and no adjuvant treatment was used.
We had 100% local control although 3 patients had a 1-year follow-up.
The location, the limited extension and the obtaining of free margins in all the resections, would explain the excellent local control rate that we obtained in tumors of the nasal cavity.
Different studies report the rates of global and specific survival and local control after endonasal treatment with endoscopes [16-18].
The series described include diverse histologies and combined treatments of endonasal surgery plus chemo and/or radiotherapy.
Nicolai, et al. [19] treated 184 patients with rhinosinusal malignancies.
134 were operated transnasally with endoscopes and 50 through a cranioendoscopic approach.
The most common histologies were: Adenocarcinoma 37%, squamous cell carcinoma 13.6%, esthesioneuroblastomas 12%, melanoma 9.2% and adenoid cystic carcinoma 7.1%.
They do not specify the origin in the nasal cavity or paranasal sinuses and include 7 lymphoproliferative tumors.
The group of tumors that stage as T1-T2 represented 42.4% and T3-T4 45.6%. 46.7% of the patients received postoperative adjuvant treatment.
According to the histology, the greatest recurrences occurred in melanomas (11/17: 65%) and in undifferentiated carcinomas (2/5: 40%).
The 5-year specific survival reported for the group treated by surgery, through anendonasal and cranio-endoscopic approach was 91.4% and 58.8% respectively, with amean follow-up of 34 months.
In our study, the local control that we obtained in patients treated only by an endonasal approach was 50%, lower than in other series.
Possibly unfavorable histologies such as undifferentiated carcinoma (3/12) and single abdominal neuroblastoma metastasis (1/12) and the death of two patients during the course of adjuvant treatment may have influenced the lower local control that was obtained.
Shah [20] reported an overall 5-year survival of 56% in patients treated with craniofacial surgery for tumors that invaded the skull base.
Patel, et al. [13] in a multicenter study on 1307 patients treated for malignant tumors that invaded the skull base with craniofacial surgery reported an overall survival, specific survival and survival without recurrence of 54%, 60% and 53% respectively.
Eloy Casiano, et al. [21] compared the results of craniofacial surgery using bicoronal and sublabial incisions (n: 48) with the transnasal approach with endoscopes (n: 18) to treat malignant tumors that invaded the skull base.
They reported a shorter hospital stay, decreased blood loss, andfaster recovery in patients treated endonasally with endoscopes.
There were no differences in survival, metastasis, and complications between the two groups.
The lower local recurrence in patients treated by endonasal surgery with endoscopes was attributed to differences in the clinical stage of the neoplasms.
In another study they compared the results of transnasal surgery with endoscopes and traditional craniofacial resection in patients with tumors that compromised the skull base.
Survival and the incidence of recurrences were similar in the two groups [22].
Mattavelli, et al. [23] reported oncological outcomes in 34 patients treated with a cranionasal approach. The 5 year overall, disease-specific, and recurrence-free survival rates were 51.2, 49.3, and 33.6% respectively after a mean follow-up of 65 months.
In our study, we treated 8 patients with combined approaches, 6 were cranionasal.
Despite the small number in the series the local control ratewe hadwas 75% with an average follow-up of 4.62 years (one patient without disease did not return to control with a follow-up of one year).
All had advanced local disease and three unfavorable histologies such as undifferentiated carcinoma and melanoma.
In four patients the lamina papyracea and the periorbit were resected, in two of them bilaterally due to the proximity of the tumor.
Three had neoadjuvant treatment with chemoradiotherapy and 5 adjuvant treatments with radiotherapy or chemoradiotherapy.
The local control and survival rate that we obtained in all treated patients (73.3%) was comparable to those obtained in other studies.
We believe that the percentage of unfavorable histologies, tumors located in the nasal cavity and advanced T (worse prognosis) may influence the results of the local control and survival rates obtained in the different studies.
If we group the patients treated in this study according to the extent and T of the neoplasms, the local control and survival rates were different.
In the fourteen patients (46.66%) with tumors of the nasal cavity and paranasal sinuses of little extension and T1-2, the local control rate that we had was 92.86% and in the most extensive, T3-4, and Kadish C it was 56.25%.
The local control rate and survival that we obtained in patients treated for malignant tumors of the nasal cavity and paranasal sinuses by endonasal surgery with endoscopes alone or combined with craniotomy or an external approach was 73.33%.
Tumors with greater extension and infiltration, with higher T staging, location in the paranasal sinuses, and unfavorable histologies such as undifferentiated carcinoma, had a greater need for neoadjuvant or adjuvant treatment and a worse prognosis than those not very extensive, T1-2 and localized neoplasms in the nasal cavity.
We have no conflicts of interest.