Primaryexternal auditory canal cholesteatoma (EACC) is a rare entity. Its association with keratosis obturans (KO) was not documented. I report a rare case with co-existence of ipsilateral EACC and contralateral KO. From clinical presentation, radiological investigation, and operative finding; I conclude to describe this case with simultaneous external canal cholesteatoma and keratosis obturans.
External auditory canal cholesteatoma, Keratosis obturans, Co-existence
External auditory canal cholesteatoma (EACC) and keratosis obturans (KO) are diseases that primarily affect the external auditory canal. The primary EACC incidence is 0.3/ 100,000 population [1] while there is no available data for incidence or prevalence of KO demonstrating the rarity nature. Toynbee in 1850 was the first to describe KO with his case report under the name of molluscum contagiosum [2]. Then in 1874, Wreden presented 12 cases with KO [3]. While in 1893, Schofield introduced the term EACC in the literature [4]. Both conditions with different pathology and inflammatory sequence, but a case with the co-existence of both condition is documented and will be discussed.
A 17-year-old female presented to me with a history of bilateral diminution of hearing of 4-month duration with gradual onset and slowly progressive course. The patient also complained of right aural discharge which is scanty, offensive, purulent, intermittent, partial improvement on medical treatment in the form of topical and systemic antibiotics, and duration of 4-months. There was no pain, facial palsy, or other otorhinolaryngologic manifestations. On examination, the right ear showed purulent, offensive, scanty discharge with aural polyp (Figure 1). Suction and packing with a topical cream containing antibiotic and anti-inflammatory were inserted. Left ear examination was revealed wax with the trial for ear wash after the patient use local softeners but the procedure was 'painful wash'. A second visit, the right ear revealed decrease discharge with shrinkage of aural polyp while the left ear still with wax with the second trial which was again a 'painful wash' that also failed to clean the external canal. Tuning fork test with bilateral Rinne negative and Weber shifted to left ear determined bilateral conductive hearing loss. Pure tone audiometry, routine preoperative laboratory investigation, and CT temporal bone recommended assessing middle ear and extension of the lesion. The audiological result revealed bilateral conductive hearing loss with an air-bone gap of 9 dB in the right ear and 23 dB in the left ear (Figure 2). CT temporal bone surprised me with bilateral external canal opacity with clear middle ear cleft and localized bony destruction in the posterior meatal wall (Figure 3). Chest X-ray assessment don't explain any pathological changes. The patient was prepared for an operation where the right postauricular incision and canaloplasty were done (Figure 4) then graft with temporalis fascia beneath the posterior meatal wall (Figure 5) [5]. While KO in the left ear was removed by hooks and suction under microscopy. I conclude to diagnose this patient with right EACC and left KO after recruiting these characteristics from history, clinical examination, and intraoperative findings. Repeated follow-up of the patient revealed early right meatal stenosis with polyp after 1 month that improved with repeated packing and topical antibiotic anti-inflammatory cream.
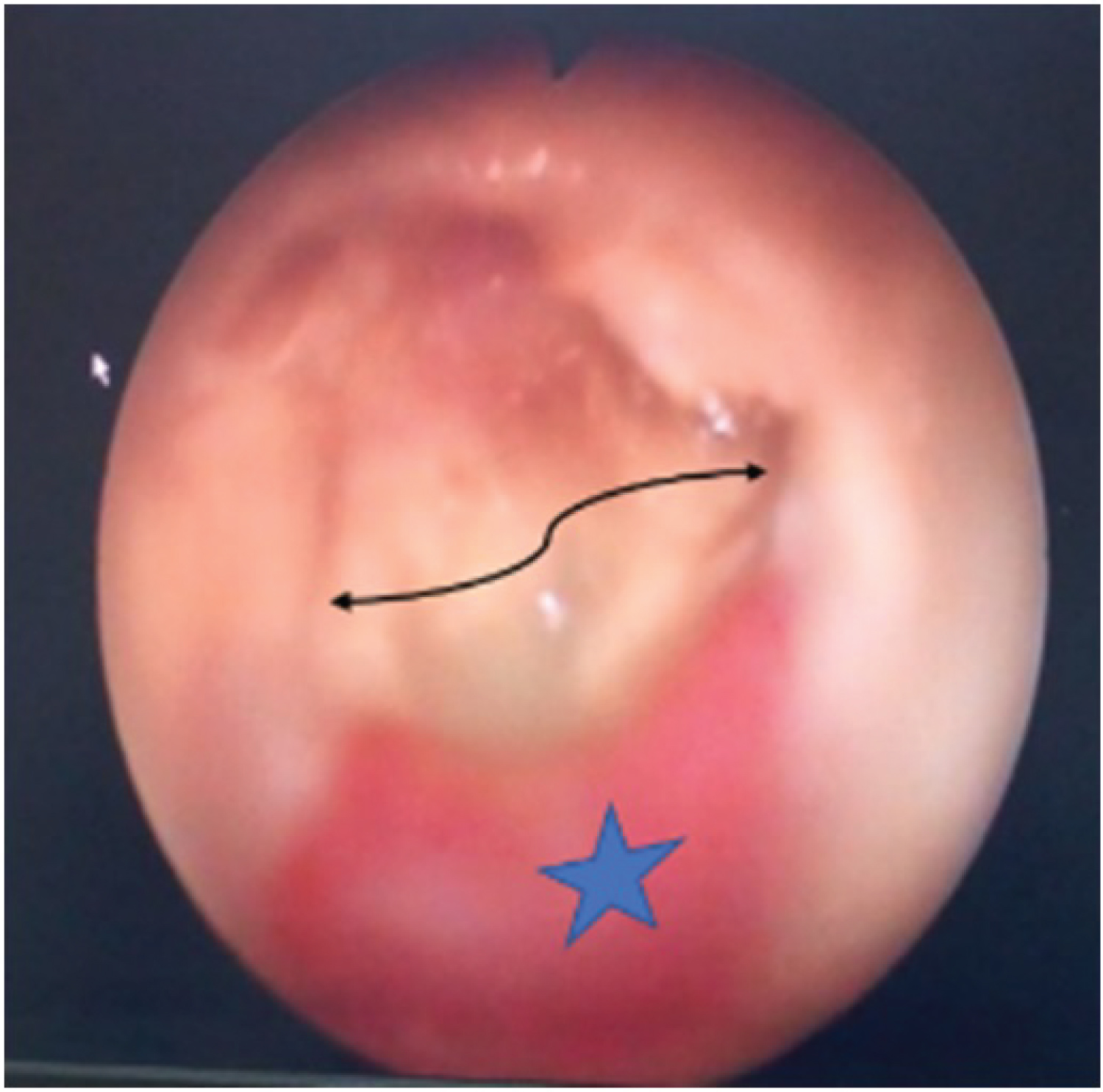 Figure 1: Right ear otoendoscopy showing aural polyp at the floor of EAC (star) and purulent discharge of the EACC (curved arrow).
View Figure 1
Figure 1: Right ear otoendoscopy showing aural polyp at the floor of EAC (star) and purulent discharge of the EACC (curved arrow).
View Figure 1
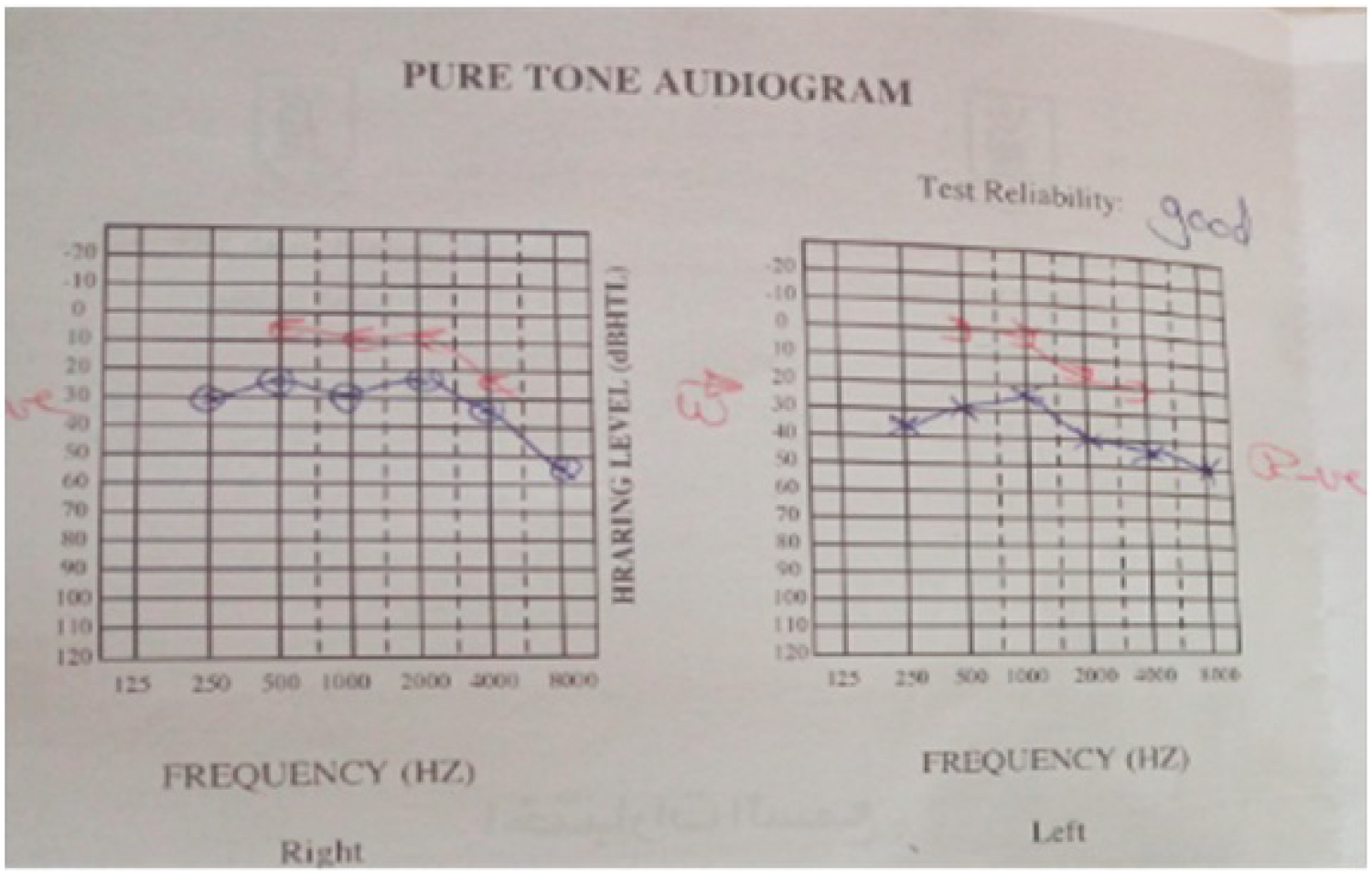 Figure 2: Pure tone audiometry for the patient with right EACC and left KO shows; bilateral conductive hearing loss with air-bone gap is 9 dB and 23 dB respectively.
View Figure 2
Figure 2: Pure tone audiometry for the patient with right EACC and left KO shows; bilateral conductive hearing loss with air-bone gap is 9 dB and 23 dB respectively.
View Figure 2
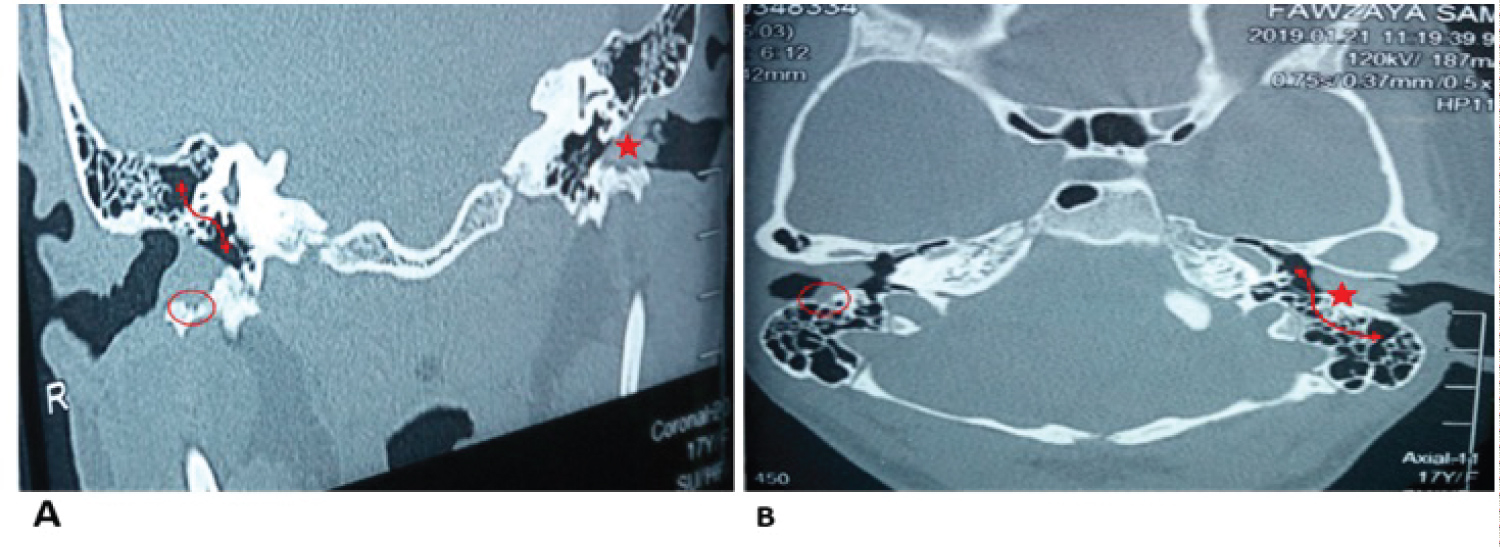 Figure 3: CT temporal bone coronal cut (A) and axial cut (B) of the patient with right EACC and left KO shows;
Bilateral EAC opacity with localized erosion in the right EAC (oval circle), plug of keratin pushing tympanic membrane medial (star), and clear middle ear cleft (curved arrow).
View Figure 3
Figure 3: CT temporal bone coronal cut (A) and axial cut (B) of the patient with right EACC and left KO shows;
Bilateral EAC opacity with localized erosion in the right EAC (oval circle), plug of keratin pushing tympanic membrane medial (star), and clear middle ear cleft (curved arrow).
View Figure 3
 Figure 4: Canaloplasty of right EAC with micromotor drill.
View Figure 4
Figure 4: Canaloplasty of right EAC with micromotor drill.
View Figure 4
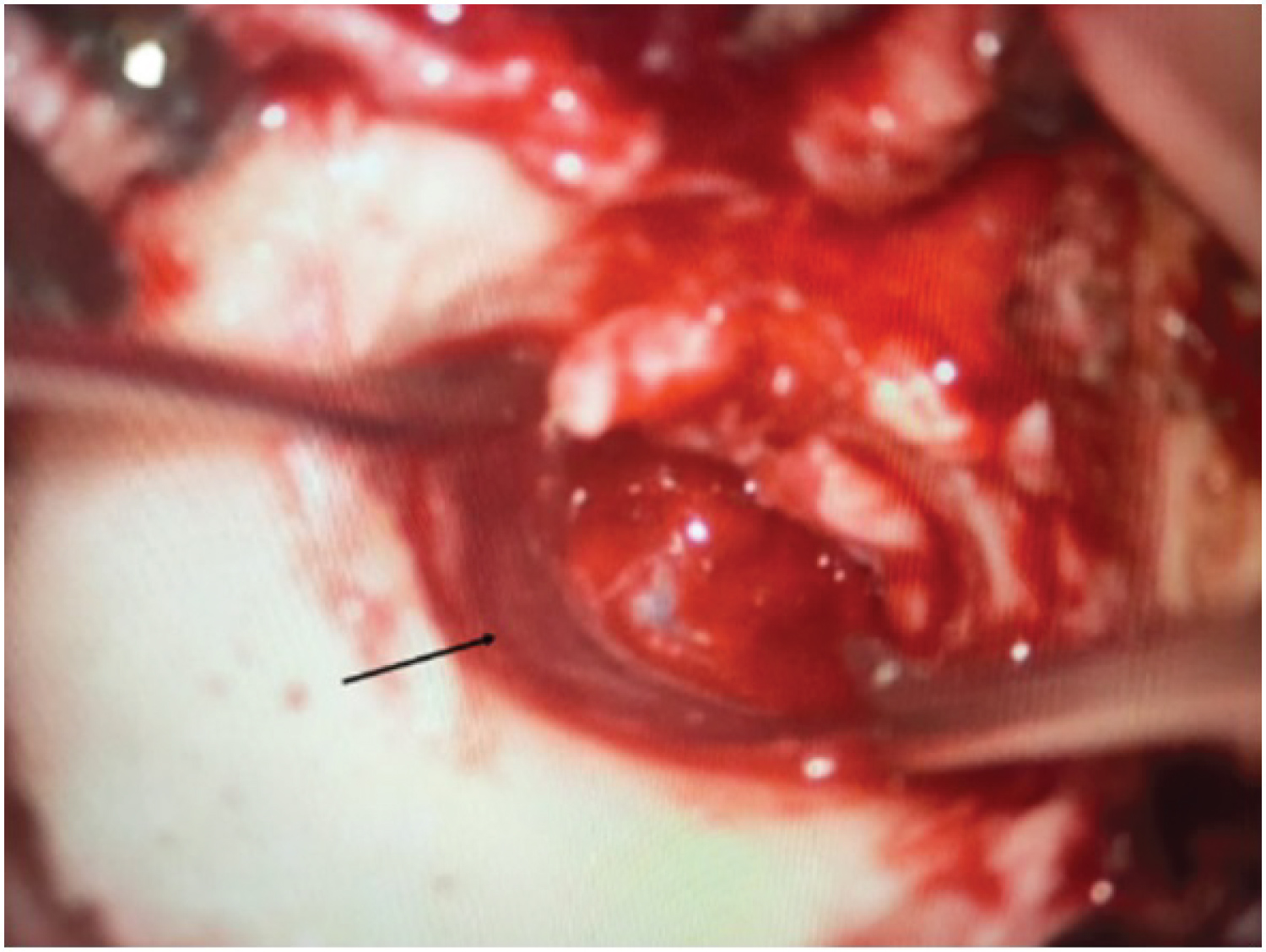 Figure 5: Temporalis fascia graft (arrow) over posterior meatal wall after canaloplasty in a patient with right EACC.
View Figure 5
Figure 5: Temporalis fascia graft (arrow) over posterior meatal wall after canaloplasty in a patient with right EACC.
View Figure 5
Although the etiology and pathogenesis of KO and EACC are different, there are some sharing features.
Multiple authors postulated that KO etiopathogenesis could be related to bronchiectasis, seborrheic dermatitis, eczema, and furunculosis [6-8] with subepithelial chronic inflammation [9].
The EACC was classified into primary (spontaneous) and secondary types with the rarity of the primary diseases estimated that its incidence was 1 per 1000 new otologic patients [10]. The etiopathogenesis of the primary EACC was illustrated under different theories. One theory of them concludes that any trauma to deep external canal skin as cotton buds or hard cerumen could induce osteonecrosis and localized periostitis [6,7,11]. With subsequent ulceration and cholesteatoma origination [12], thus the cause of EACC is the initial periostitis induced by trauma to the deep canal [13] and not the result of this disease [6]. Then, the proteolytic enzymes excreted leading to more bone erosion with characteristic dull pain [14].
Both EACC and KO could be linked together where their original theory and pathogenesis are inflammation. The presenting case is diagnosed with left KO and right EACC. The patient may be started with bilateral KO. Then, this patient starts manipulation to her right ear (dominant side) with cotton buds too early trying to remove annoying hard wax in the deep canal leading to focal periostitis and aural polyp formation. Progression of the diseases with repeated trial to self-cleaning her canal and delay in receiving medical consultation augment cholesteatoma formation with subsequent shifting the newly originating disease from KO to EACC.
The patient developed right aural polyp 1 month postoperatively due to her usual habits of trial to clean her right external canal. My hypotheses suppose that bad habits by the patients could change the pathogenesis of certain disease to another one.
Although the rarity of EACC and KO, Simultaneous coexistence of both diseases can be present. EACC treatment includes surgical intervention with canaloplasty and fascia grafting, while KO needs the removal of the plugs under the microscope.
The author declares that there are no conflicts of interest regarding the publication of this article.