Objectives: To report a case of accidental application of cyanoacrylate (superglue) to the external auditory canal (EAC) and offer guidance on the management of this type of injury.
Methods: Case report and literature review.
Results: A 74-year-old man presented with right aural fullness after accidentally administering cyanoacrylate to his EAC. Dissolution with acetone and careful removal with alligator forceps was successful and led to complete resolution of symptoms without injury to the tympanic membrane or ear canal.
Conclusions: Cyanoacrylate is a common household product that can pose distinct challenges in management when involving sensitive tissues of the head and neck, including mucosa, ear canals and eyes. Pre-treatment with optimal solvents can greatly enhance safe removal of the substance and mitigate damage to existing structures.
Cyanoacrylate is a highly adhesive compound formed by formaldehyde and cyanoacetate that comprises the product Superglue ® . Cyanoacrylate monomers polymerize quickly after contact with rigid structures, and the agent has been popularized since its commercial introduction in 1958 [1-3]. Since that time, many injuries have been reported in the literature.
Even though medical applications of cyanoacrylate exist, such as dental cements and skin adhesives, these formulations generally use longer-chain cyanoacrylate derivatives and have lower tissue toxicity compared to non-medical superglue [4]. Additionally, involvement of sensitive structures and tissue (such as the eyes, nasal mucosa and ears) can incur distinct complications that warrant careful interventions [5-7]. Notably, superglue applicators are commonly mistaken for eye or ear drops, and one study of 105 ocular superglue injuries reported that over 78% of injuries were a result of accidental application by patients [5].
A 74-year-old male is referred to otolaryngology-head and neck surgery clinic for a complaint of right ear fullness. His medical history was remarkable for elevated body mass index and pre-diabetes. Patient is a United States veteran, with a history of loud-noise exposure. He denies any history of ear ailments and surgeries.
On presentation, he reported a three-day history of right sided aural fullness, decrease in hearing, and feeling something palpable “in his ear”. He denied vertigo, dizziness, and balance issues. He noted a lengthy history of cerumen impaction, treated successfully with occasional over the counter carbamide peroxide ear drops. He denied ear pain, otorrhea, and pruritis. Recent otologic examinations had shown there to be an intact ear drum bilaterally.
His exam was remarkable for the complete occlusion of his right ear canal with a white, crystalline substance visibly extending outside of his external ear canal (Figure 1A). His tympanic membrane was unable to be visualized on the right side due to the obstruction (Figure 1B). The external ear was unremarkable and not inflamed. The left ear exam was unremarkable, with minimal soft, yellow cerumen noted.
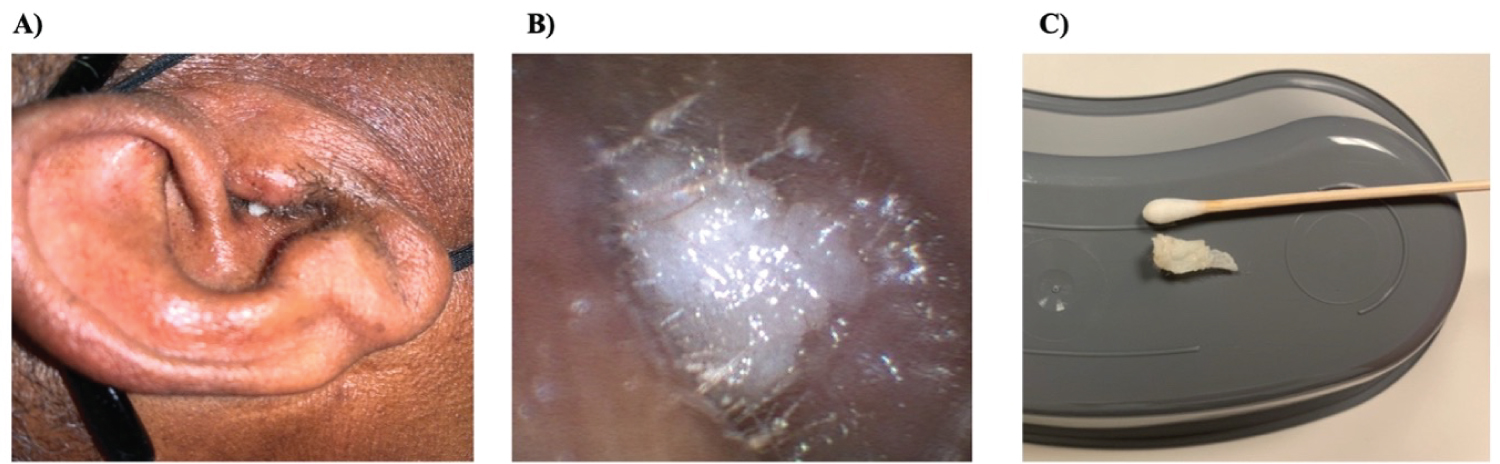 Figure 1: Otologic examinations (A) His exam was remarkable for the complete occlusion of his right ear canal with a white, crystalline substance visibly extending outside of his external ear canal; (B) His tympanic membrane was unable to be visualized on the right side due to the obstruction; (C) Thus, we continued with gentle, slow traction until the cast was removed in its entirety from the ear.
View Figure 1
Figure 1: Otologic examinations (A) His exam was remarkable for the complete occlusion of his right ear canal with a white, crystalline substance visibly extending outside of his external ear canal; (B) His tympanic membrane was unable to be visualized on the right side due to the obstruction; (C) Thus, we continued with gentle, slow traction until the cast was removed in its entirety from the ear.
View Figure 1
Patient reports that he lives at home with his middle-aged son, who is affected by cognitive disabilities. He serves as the primary caretaker for his son, and about three days ago he was helping his son repair his broken glasses with adhesive gel. Upon further questioning, it was determined that he had mistaken a superglue product for ear drops and had administered the cyanoacrylate agent to his right ear accidentally.
The patient was then offered and consented for debridement with a pre-treatment of acetone, in the formulation of nail polish remover. We soaked a cotton tip applicator in nail polish remover and gently rimmed the superglue cast with the applicator under microscopic guidance in clinic. This was repeated several times and performed until the superglue cast was circumferentially freed and lifted off the external meatus soft tissue. Once free, we gently grabbed the cast with alligator forceps and applied minimal traction. In doing so, patients denied any pain, vertigo, or change in hearing. Thus, we continued with gentle, slow traction until the cast was removed in its entirety from the ear (Figure 1C). After removal, microscopic guidance revealed a mildly inflamed external meatus, with a healthy appearing tympanic membrane. Inspection of the superglue cast showed it to be about 1.8 cm in length (for reference a typical adult ear canal is approximately 2.5 cm in length).
Cyanoacrylate administration to the external auditory canal (EAC) can cause otalgia and trismus and can obstruct the meatus or damage the tympanic membrane leading to conductive hearing loss. A review of cyanoacrylate-related ear injuries by Dimitriadis, et al. summarized 10 cases between 1987 and 2008, seven of which were accidental [3]. Two were treated conservatively, while three resolved after application of pure acetone and one after warm hydrogen peroxide. The remaining four cases underwent surgery requiring general anesthesia to separate the cast from the meatus and tympanic membrane to endaural incision [3]. Since that review, three additional cases have been reported of superglue removal from the ear canal after acetone administration [2,6,8]. In one case, the acetone was reported to have no effect, but in all three cases the glue was extractable from the meatus [2,8] or from the tympanic membrane itself [6].
Acetone is a clear, rapidly evaporating volatile liquid that mixes with most organic solvents as well as water. It is a natural physiologic metabolite and thus low in toxicity [6]. In prior cases, acetone formulations have included pure acetone and nail polish remover within duration of application spanning from one minute [2] to 30 minutes [6]. Across the case reports, authors commonly discharged patients with a short course of oral antibiotics and topical ear drops. While three percent hydrogen peroxide has been reported to aid in removal of superglue [9], other solvents of cyanoacrylate (such as xylene, toluene, nitromethane and methylene chloride) are generally more toxic or irritating to skin and mucosa [10].
Our experience, combined with past reports summarized in Table 1, highlight the importance of recognizing this rare, yet serious occurrence. Moreover, our experience highlights that even in cases of substantial external ear canal occlusion with superglue, acetone application and careful microscopic removal in clinic may be attempted by an experienced otolaryngologist. Removal in clinic (versus operative exploration) maximizes patient outcomes, minimizes delay/morbidity of treatment, and limits unnecessary healthcare costs.
Table 1: Published case reports of cyanoacrylate applications to the EAC and treatment details. View Table 1
Cyanoacrylate is a common household product that can pose serious injury to vital structures and sensitive tissues in the head and neck. Although various solvents and interventions have been proposed, acetone remains a safe agent to enhance the safe removal of cyanoacrylate in many instances.
None.