Objective: Dietary factors and the nutritional status of adolescents determine health outcomes in later years. This study investigated dietary factors as predictors of overweight and obesity.
Methodology: A descriptive cross-sectional study of 2261 in-school adolescent girls, 10-19 years was conducted using a multistage stratified random sampling procedure from three geopolitical zones in Nigeria. Dietary factors - Nutrition Knowledge (NK), Dietary Diversity (DD), Dietary Behaviour (DB) and Dietary Proficiency (DP) were investigated. Weight and height were measured using standard procedure. Body Mass Index-for-age percentiles were used to classify into nutritional status (NS). Chi-square was used to test the association between NS and dietary factors while binary logistic regression was used to predict overweight/obesity. Statistical significance was taken at p < 0.05.
Results: Mean scores recorded were age (14.86 ± 1.78 years), NK (9.33 ± 2.15), DD (8.47 ± 2.93), DB (5.66 ± 1.80) and DP (29.12 ± 4.12). Percentage with high NK, DD, and DB scores was highest among the 14-16 years group. About 10%, 4.4% and 2.6% were underweight, overweight and with obesity respectively. Significant associations existed between NS and NK (p = 0.046) and DB (p = 0.009). Those who were overweight (OR = 0.825, 95%CI = 0.552-1.234) and obese (OR = 0.477, 95%CI = 0.274-0.830) were less likely to have high NK. Those who were overweight (OR = 1.287, 95%CI = 0.860-1.927) and obese (OR = 1.171, 95%CI = 0.686-1.999) were more likely to have high DD. In addition, those with overweight (OR = 0.519, 95%CI = 0.344-0.784) and obese (OR = 0.704, 95%CI = 0.413-1.200) were less likely to have high DB, likewise, those who were obese (OR = 0.839, 95%CI = 0.493-1.429) had the likelihood of lower DP.
Conclusion: Being overweight or obese was predicted by decreased NK, DB and DP as well as increased DD among adolescent girls. This could be addressed through targeted nutrition education, age-specific intervention, promoting a more diverse diet, and encouraging healthy eating habits to empower adolescent girls to achieve optimal health in Nigeria.
Nutrition knowledge, Dietary diversity, Dietary behaviour, School adolescent female, Body weight, Nigeria
Adolescence is defined by the World Health Organization (WHO) as the second decade of life (10-19 years of age) [1]. There are 1.3 billion adolescents in the world today, more than ever before, making up 16 percent of the world’s population [2]. In Nigeria, adolescents account for 24% of the total population. The number of adolescents will continue to grow as fertility rates in Nigeria remain high (4.6%) [3].
Adolescence is a time of rapid growth and development. It offers the 2 nd window of opportunity for catch up in growth that flattered during childhood. In most developing countries, many adolescents enter this stage in life undernourished. In Nigeria for instance, under-nutrition was widespread among adolescents with wasting and stunting being more frequent in the rural areas [4]. Adolescent girls are particularly vulnerable to undernutrition because they are growing faster than at any time after their first year of life [5]. They need protein, iron, and other micronutrients to support the adolescent growth spurt and meet the body's increased demand for iron during menstruation. Yet Adolescent girls either eat too little or too much, many have food fads, skip meals and regularly eat junk foods. Also, they tend to eat more meals outside the home compared to younger children [6]. Moreover, there is a lot of peer pressure to indulge in unhealthy meals and snacks. Meal convenience is important to many, and they may be overeating the wrong types of food like soft drinks, fast foods, ultra-processed foods, less nutrient-dense foods and more energy-dense foods [7]. These lead to increased weight, consequently overweight and obesity, which is on the increase [8-10].
Globally, there has been an increase in the prevalence of overweight/obesity among children and adolescents aged 5-19 from 8% in 1990 to 20% in 2022 [11]. The rise has occurred similarly among boys and girls: In 2022 19% of girls and 21% of boys were overweight [11]. In developing countries, the prevalence rose from 2% in 2017 to 8% in 2019 [12]. Nigeria ranges between 4.1% and 14.6% for overweight and 1.3% to 10.2% for obesity [13-16]. Africa is facing a growing problem of obesity and overweight, and the trends are rising. This is a ticking time bomb. If unchecked, millions of people, including children, risk living shorter lives under the burden of poor health [11]. This can be resolved as well because many of the causes of obesity and overweight are preventable and reversible.
Nutritional deficiencies and poor eating habits established during adolescence can have severe immediate and long-term consequences, including delayed sexual maturation, loss of final adult height, micronutrient deficiencies- anaemia, osteoporosis, including increased susceptibility to infections, cognitive impairment, behavioural problems, decreased school performance and work productivity, as well as increased risk of overweight/obesity and increased presentation of cardiometabolic risk factors later in life [17]. Even worse, stunted adolescent girls are more likely to give birth to underweight infants that would be stunted in later life [18]. These children are more likely to face cognitive impairments, short stature, lower resistance to infections, and a higher risk of disease and death throughout their lives, continuing the vicious cycle of malnutrition [5].
Significant risk factors for malnutrition among adolescent girls included dietary diversity, eating sweet foods or beverages, and poor nutrition knowledge [19]. Other studies found that good nutrition knowledge among adolescent girls had a positive influence on healthy food choices and diet quality [20]. Poor dietary habits, such as skipping meals, low intake of fruits, and high consumption of sweetened drinks were shown to have an association with poor nutritional status of adolescents [21,22]. Additionally, the consumption frequency of various food groups like rice, milk, red meat, vegetables, and fruits plays a crucial role in determining the nutritional status of adolescent girls [23,24].
In general, dietary factors determine the nutritional status either positively or negatively. Both underweight and overweight/obese co-exist in adolescents with overweight/obese on the increase. Therefore, this study aimed to further investigate the dietary factors that predicted overweight and obesity in-school adolescent girls in Nigeria.
This is a descriptive cross-sectional study among in-school female adolescents aged 10-19 years. Three geopolitical zones were purposively selected out of the six geopolitical zones in Nigeria. Two states each were selected from the three zones namely, North Central (Kogi and Niger States), South East (Abia and Imo States) and South West (Osun and Ondo States).
Sampling was done using a multistage stratified random sampling procedure to select schools and students who participated in this study. In the first stage, six states were purposively selected. In the second stage, the local government areas (LGAs) in each of the selected states were grouped according to their urban, peri-urban or rural statuses. Two most-peri-urban LGAs and 2 most-urban LGAs were purposively selected in each state. In the third stage, the lists of secondary schools in the selected LGAs were obtained from their respective Local Education Authorities; two schools were randomly selected from each of the LGAs by ballot. Twenty-five students each were randomly selected in junior and senior arms of the designated schools. School registers were used to generate a sampling framework from which eventual participants were selected using a systematic sampling technique with K th interval once a participant had been chosen randomly.
The sample size was determined using the Research Advisors, 2006 [25] at 95% confidence and 5% margin of error. Since parameters were determined in each of the six selected states, each state was treated as a population. From the Research Advisor, the sample of 355 is considered sufficient to allow rational estimation in each of the six states, irrespective of the population size. However, a proportionate sampling size distribution method was used to allocate sample size to each state. Assuming a non-response rate of 5%, the adjusted calculated sample size for each of the six states was 372, and this translated to a total minimum sample size of 2,232. Schools that run boarding house systems, pregnant and lactating adolescents, and privately owned schools were excluded from this study.
Four research assistants were recruited and trained to assist in data collection for each state. Two days of training on the use of Open Data Kit (ODK) for data collection was conducted. The field assistants worked in pairs to reduce interpersonal bias. The data were collected concurrently for 2 weeks in April 2023 in all the states to prevent seasonality bias in food availability.
A validated questionnaire was used to elicit information from the adolescent girls. This consisted of Nutrition Knowledge (NK), Dietary Diversity (DD), Dietary Behaviour (DB) and a section for recording Anthropometric measurements. NK was used to assess the adolescents' understanding of nutrition. The questionnaire included a list of fifteen pre-defined statements with a score of one for correct response and zero for incorrect. The total nutrition knowledge score was obtained by adding the responses and the maximum score obtainable was 15 points. Knowledge scale was drawn by calculating the overall mean and standard deviation scores. The score obtained by adding the mean and standard deviation was classified as high [26].
For DD, a food intake checklist 24-hour dietary recall was used. The adolescent girls were asked to describe the foods and drinks they consumed in the preceding 24 hours. Two 24-hour diet recalls (one weekday and one weekend day except party days) were completed for each girl. DD Questionnaire consisting of fifteen food groups was used to calculate the DD Score. The most varied diet has a score of fifteen. DD score was created by summing the number of individual food groups consumed over the past 24 hours and the scale was calculated by obtaining the overall mean and standard deviation scores. A high DD score was obtained by adding the mean and standard deviation [26-28].
For the DB, seventeen questions were investigated out of which nine were included in the DB score calculation. The DB scale was drawn by calculating the overall mean and standard deviation scores. The score obtained by adding the mean and standard deviation was classified as high. The NK, DD and DB scores were classified into tercile for descriptive purposes; however, the focus was on high scores. These were further dichotomized for binary logistic regression analysis. High NK, DD and DB were taken at a score above the summation of the mean and standard deviation of the total score.
Dietary Proficiency (DP) was used to condense a combination of NK, DD and DB. The DP score was calculated by the summation of DD, NK and DB scores, which were later dichotomized into Healthy Dietary Proficiency (HDP) and Unhealthy Dietary Proficiency (UDP). HDP was taken at a score above the summation of the mean and standard deviation of the total score.
Body Mass Index was calculated as the weight in kilograms divided by the square of the height in meters (kg/m 2 ). It was classified using the sex-specific BMI-for-age Z-scores WHO Growth Reference for school-aged children and adolescents. Percentile of < 5 th = Underweight, 5 th -85 th percentile = Healthy weight, 85 th -95 th percentile = Overweight and > 95 th percentile = Obese. This was done using WHO AnthroPlus [29,30].
A total of 2261 verified data were entered into the computer using SPSS version 24. The descriptive statistics employed included mean, standard deviation, frequency distribution and percentage while the inferential statistics used included Chi-square for continuous variables and binary logistic regression for categorical variables. The statistical significance was set to a p-value of less than 0.05.
In total, 2261 in-school adolescent girls (10-19 years) were included in this study. The data in Table 1 showed that those who were in the 10-13 years age group were 529 (23.4%), 14-16 years were 1315 (58.2%) and 17-19 years were 417 (18.4%). The mean age was 14.86 ± 1.78 years. Those from urban were 51.7% and 48.3% were from peri-urban. Proportional distribution was observed across regions; with South West having 38.7%. The mean weight was 47.81 ± 9.02 kg and height was 1.55 ± 0.09m.
Table 1: Socio-demographic and anthropometry characteristics of adolescent girls (n = 2261). View Table 1
In terms of nutrition knowledge, 96.1% understood the role of water in aiding digestion and 87% knew that exercise helps in the prevention of obesity. Also, majority (85.4%) knew milk and meat are food sources of protein and about 85% knew vitamins and minerals protect the body against diseases. About four in five adolescent girls knew milk and milk products provided calcium and vitamin for bone health (79.6%), carbohydrate and fats produced energy for the use of the body (79.4%), and that protein repairs worn out tissues (78.6%). Likewise, 61.3% knew that iron is relevant in the formation of red blood cells, however, 31.8% had a misconception about anaemia and thought it could be corrected by eating fatty foods. Only 24.8% and 28.4% got the function of fiber-rich food in constipation prevention and nuts and pulses as protein alternatives to fish correctly respectively. In all, the mean nutritional knowledge score of the girls was 9.33 ± 2.15 (Figure 1).
 Figure 1: Percentage of correct responses in nutrition knowledge statements.
View Figure 1
Figure 1: Percentage of correct responses in nutrition knowledge statements.
View Figure 1
Based on the 24-hour recall, fifteen food groups were investigated and ranking was done from most consumed in number 15 to the least in number 1. Mean DD was 8.47 ± 2.93. Energy-dense food groups were the largely consumed food groups. Oil and fats (15), cereals (14), roots and tubers (12) and sweets (10). However, nutrient-dense food groups that are of importance to adolescent girls’ health were the least consumed which included vitamin A-rich vegetables (1), other fruits (2), eggs (3), nuts and seeds (4), vitamin A-rich fruits (5), milk and milk products (6) and beans and peas (7) (Figure 2).
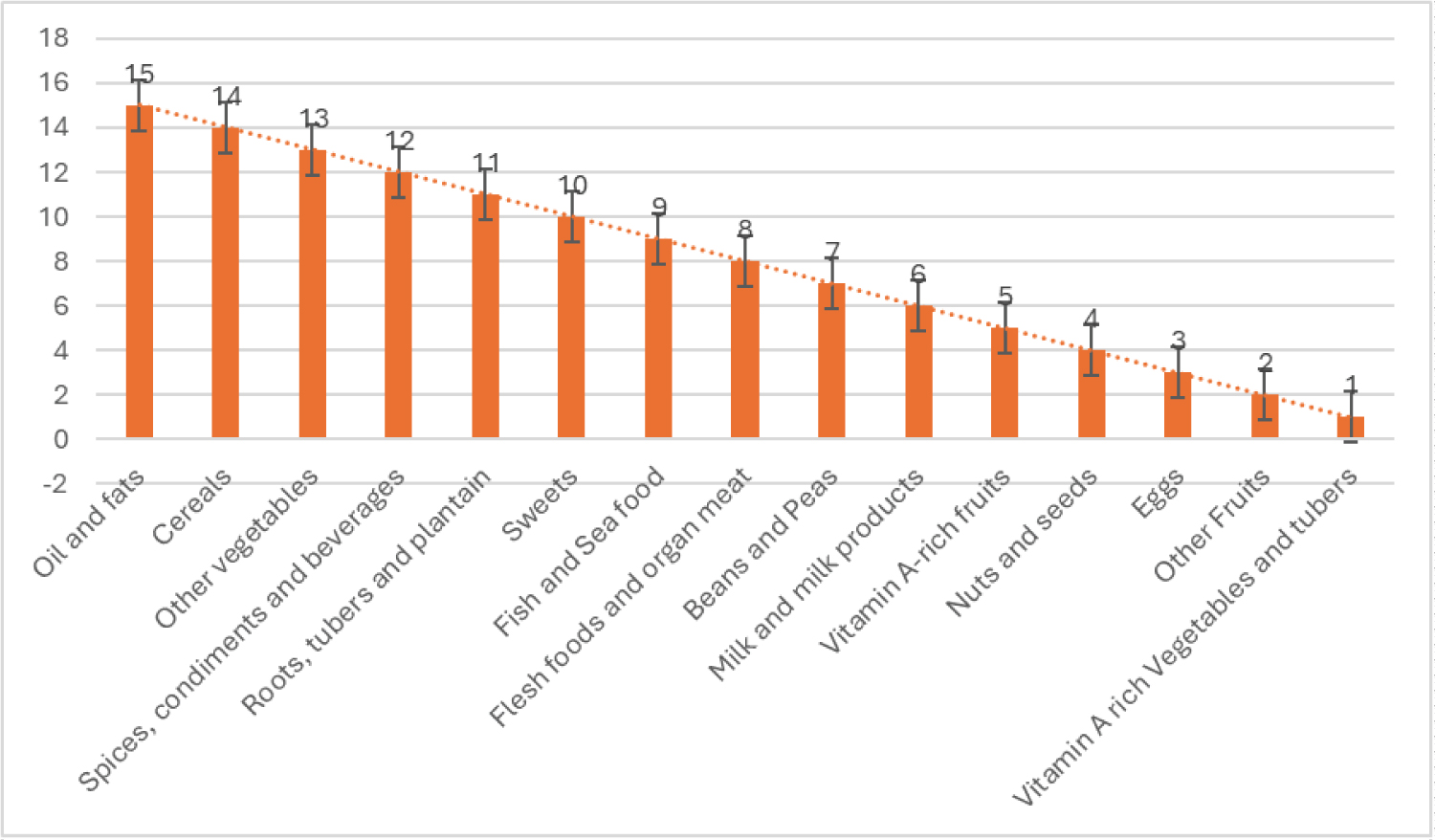 Figure 2: Dietary diversity ranking from most to least consumed food groups.
View Figure 2
Figure 2: Dietary diversity ranking from most to least consumed food groups.
View Figure 2
Information on the dietary behaviour of adolescent girls is presented in Table 2. The mean DB score was 5.66 ± 1.80. About 34 percent sometimes skipped meals, out of which 31.9% sometimes skipped breakfast and 56% skipped lunch. Majority (81.1%) ate lunch and dinner (95.9%), however, 32.2% and 24.5% ate their lunch and dinner late respectively. Most of the girls (95.0%) consumed snacks and 86.9% took carbonated drinks daily. About 51% of the adolescent girls confirmed replacing main meals with snacks, particularly for lunch (67.0%) and breakfast (22.8%). About 34 percent of the girls patronized food vendors.
Table 2: Dietary behaviour of adolescent girls (n = 2261). View Table 2
In this article, we were particular about age-specific data as presented in Figure 3. Percentage of adolescent girls having high DD, NK, DB and DP scores was highest among the 14-16 years group. Surprisingly, those who were transitioning into adulthood; 17-19 years that scored high were 18.5%, 20%, 17.2% and 18.4% for DD NK, DB and DP respectively.
 Figure 3: Percentage of adolescent girls having high DDS, NKS, and DBS by age group.
View Figure 3
Figure 3: Percentage of adolescent girls having high DDS, NKS, and DBS by age group.
View Figure 3
Data in Figure 4 showed that 17.5% of the adolescent girls were rated as having Unhealthy Dietary Proficiency. Although the majority (82.5%) were rated as having Healthy Dietary Proficiency, considering the mean values of individual dietary factors that make up DP, the values were marginal and slight exposure to vulnerability shock could tilt the adolescent girls towards UHDP.
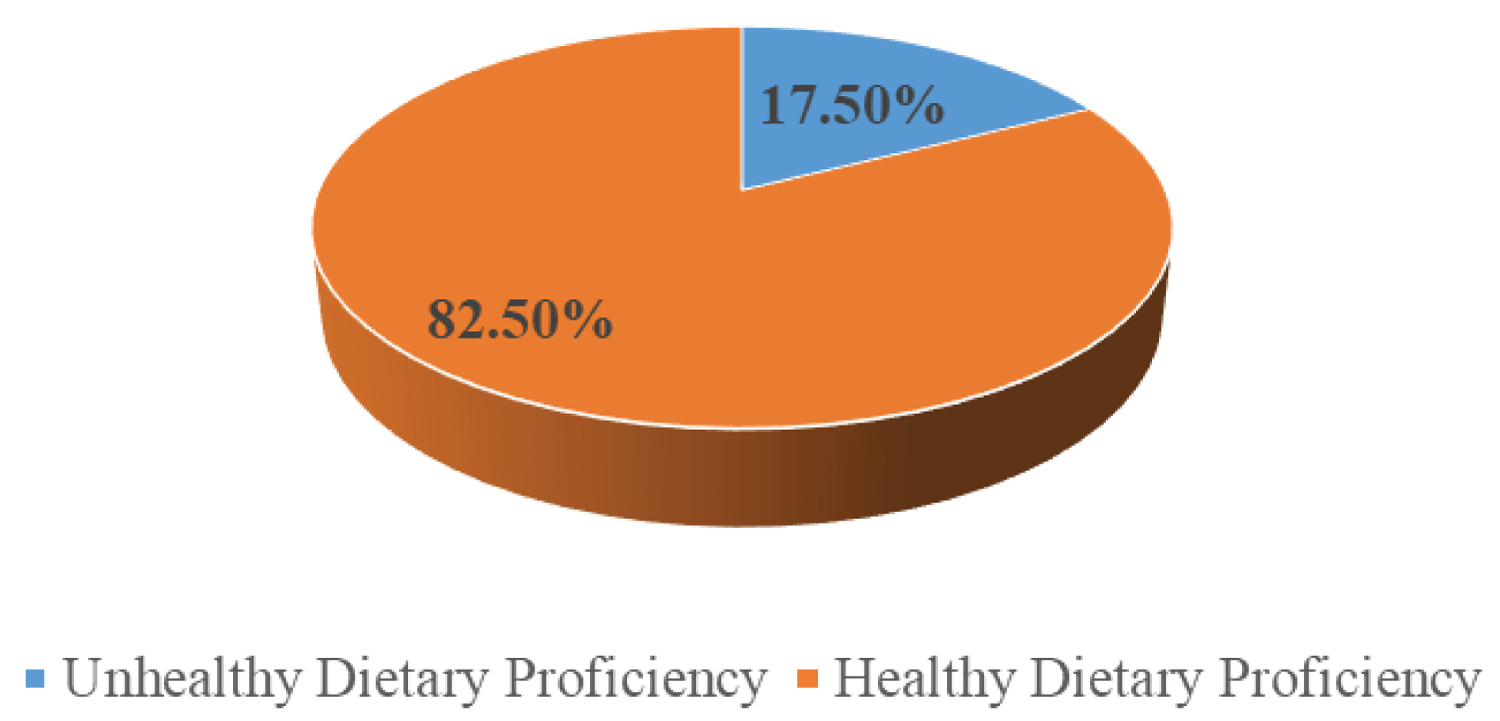 Figure 4: Level of dietary proficiency.
View Figure 4
Figure 4: Level of dietary proficiency.
View Figure 4
The measurement of the nutritional status (Table 3) showed that majority of the adolescent girls (83.3%) had healthy weight (5 th -85 th percentile while 9.8%, 4.4% and 2.6% were underweight (< 5 th percentile), overweight (85 th -95 th percentile) and with obesity respectively.
Table 3: Nutritional Status of adolescent girls in Nigeria. View Table 3
Empirical evidence from the chi-square analysis in Table 4 showed that significant associations existed between nutritional status and nutrition knowledge (p = 0.046), as well as dietary behaviour (p = 0.009). Whereas, no significant relationship was recorded between nutritional status and dietary diversity, likewise dietary proficiency (p > 0.05).
Table 4: Chi-square analysis showing the association between Dietary factors and Nutritional Status. View Table 4
The binary logistic regression analysis in Table 5 indicated that those who were overweight (OR = 0.825, 95%CI = 0.552-1.234) and obese (OR = 0.477, 95%CI = 0.274-0.830) were less likely to have high NK compared to the reference group. The girls who were overweight (OR = 1.287, 95%CI = 0.860-1.927) and obese (OR = 1.171, 95%CI = 0.686-1.999) were more likely to have high DD. In addition, those with overweight (OR = 0.519, 95%CI = 0.344-0.784) and obese (OR = 0.704, 95%CI = 0.413-1.200) were less likely to have high DB as well as those who were obese (OR = 0.839, 95%CI = 0.493-1.429) had the likelihood of lower DP compared to the reference group.
Table 5: Binary logistic regression analysis showing the odds of nutritional status and dietary factors. View Table 5
Being overweight or obese was predicted by decreased odds of NK, DB and DP as well as increased odds of DD among adolescent girls.
In this study, on the average, the adolescent girls demonstrated good nutrition knowledge, however, gaps existed in the knowledge of the health benefits of fibre-rich foods, dietary approach to anaemia prevention, and nutrient composition of fruits and vegetables among others. One of the health benefits of dietary fibre, which is predominant in fruits and vegetables is the prevention of overweight/obesity. This knowledge gap might result in low consumption since a high proportion of the girls thought that fibres are rich in fat. Good nutrition knowledge in the current study agrees with the reports among adolescents in Ibadan [31], Lagos [32], and Abuja [33] but contradicts the poor nutrition knowledge among adolescent girls in some rural communities of Northern Nigeria [34]. Regional differences and rural-urban differences in access to information, nutritional situation and health outcomes are well-known in developing countries, and this may be responsible for the contradiction with the reports from rural areas in Northern Nigeria. In a systematic review [35], it was noted that nutrition knowledge is not sufficient to result in healthy eating as four of the studies reviewed reported a non-significant association between overall nutrition knowledge and practices. In another study in Ethiopia [36], it was reported that although nutrition knowledge affects dietary practices, nutrition knowledge alone cannot guarantee an individual’s behaviour, however, it can significantly shape their attitude which can be reflected in a person’s actions. The above underlies the importance of adequate nutrition education to these adolescent girls.
Iron deficiency anemia remains a public health challenge in Nigeria and the gap in nutrition knowledge may be a major contributory factor. Presently, more than half of women of reproductive age show some form of anaemia in Nigeria [37]. Studies in Nigeria and Bangladesh have reported poor knowledge of diet and prevention of anaemia among adolescents [22,38]. In Nigerian settings, opportunities available to adolescents to learn about nutrition are largely limited to school-based subjects with few nutrition components and social media. However, the subjects taught may be inadequate in facilitating dietary behaviour change, especially where poor skills and lack of motivation hamper these subjects’ teachers' abilities or competencies. Likewise, social media are poorly regulated and misleading information may be disseminated, thereby causing more confusion among adolescents. It is therefore, expedient to put in place more opportunities at the community level, school-based platforms and religious settings to promote active nutrition education among Nigerian adolescents. Exploring the known linkage between nutrition knowledge and dietary practices is important to promote good nutrition outcomes among adolescents.
This study also found that the diets of the adolescents are devoid of many food groups notable for the supply of micronutrients of public health significance. The dietary diversity score among the adolescent girls reflects largely the consumption of less diverse food groups [32,39], which were predominant in fats, oil and starchy staples [40,41]. Neglect of fruits, legumes and animal products raises concern about micronutrient deficiencies. A similar study in South West Nigeria [26] also reported low consumption of iron from dietary sources.
In this study, dietary behaviour constitutes a serious concern following the predominance of meal skipping, late consumption of dinner, high consumption of snacks and soft drinks, patronage of food vendors, and the replacement of meals with snacks. These behaviours constitute health and nutrition risks that warrant immediate intervention and can contribute to the rising prevalence of overweight and obesity. In a similar study, skipping meals increases the odds of inadequate dietary diversity [42] and could likewise lead to overeating or making poor dietary choices which include less fruits and vegetables, high-energy snacks and soft drinks whenever the next meal is taken. Meal skipping among Nigerian adolescents was also documented in earlier studies in Nigeria [22,33,43-46]. The high rate of meal skipping among adolescents is worrisome because of the well-known linkage between nutrition and learning outcomes. Another study on breakfast skipping found that skipping breakfast was associated with lower cognitive and emotional engagement in school [47]. Nevertheless, in this current study, it is comforting to note that breakfast being the most important meal of the day was less frequently skipped, as was also reported in Lagos [45]. However, a fraction replaced it with snacks in this study. Talking of cognitive function, it was observed that the nutrition statements that were rated low were all in negative forms. Perhaps the girls did not comprehend that the correct responses would also be in the negative form.
Snacking is very common among the adolescents with half of them replacing the main meal, particularly lunch with snacks, which explains why lunch is the most frequently skipped meal. This is in tandem with the findings in Ghana where 56% of the adolescents reported they consumed snacks [48]. The prevalence of daily consumption of soft drinks in this study is higher than the observation of similar studies reported among adolescents in Ogun State [49] and Europe [50].
Healthy dietary behaviour cultivated during adolescence is critical for optimal physical growth, cognitive and psychosocial development and prevention of diet-related diseases [48]. In this study, the most consumed foods were energy-dense while the least were nutrient-dense. This observation agrees with the reports of similar studies in Ghana [42], and Europe [51]. Globally, adolescents have been shown to consume excessive amounts of energy-dense ultra-processed foods with high contents of sugar, fat and sodium but do not consume sufficient micronutrient-rich foods such as fruits and vegetables, pulses, whole grains and nuts and oil seeds [52,53]. The cereals, roots, tubers and plantain are Nigerian starchy staples that are available, accessible and affordable to most segments of the population which may have contributed to their higher consumption. Consequently, too much consumption could lead to being overweight or obese.
In this study, malnutrition still constitutes a public health problem, particularly underweight with a steady rise in overweight and obesity reported in Sub-Saharan African countries [54], South Africa [55] and South-South Nigeria [56]. Similar studies also reported the same trend [12,14-16,31]. Other studies have shown a significant association between nutritional status and dietary behaviour [57,58] indicating that individuals with poor eating behaviours are at a higher risk of nutritional disorders. Being overweight or obese was predicted by decreased odds of NK, DB and DP as well as increased odds of DD among adolescent girls. This is expected as the NK, DB and DP decrease, there is the likelihood of being overweight or obese. Conversely, higher DD resulted in a higher likelihood of being overweight or obese. This aligns with the expectation that more diverse foods are a proxy for nutrient adequacy [59]. However, caution should be exercised in the consumption of energy-dense food which is a driver of weight gain as is the case in this study.
This study highlights the complex interplay between various dietary factors and nutritional status among adolescent girls in Nigeria. The findings revealed knowledge gaps, limited dietary diversity, and issues concerning dietary behaviours and rising overweight and obesity. It was concluded that a decrease in NK, DB and DP increases the likelihood of overweight/obesity. Whereas, an increase in DD with an increase in fats and oil, starchy food sources and sweets consumption increases the likelihood of overweight/obesity among adolescent girls in Nigeria. These findings raise some concern and echo similar trends observed in other developing countries.
To combat obesity and overweight, as WHO recommends [11], a range of priority measures such as promoting healthier foods among young people is recommended. By addressing these issues through targeted nutrition education, age/gender-specific intervention, promoting a more diverse diet, and encouraging healthy eating habits, we can empower adolescent girls in Nigeria to achieve optimal health.
This work was supported by the National Research Fund (NRF) of the Tertiary Education Trust Fund (TeTFund), Nigeria, [grant numbers: NRF_SETI_HSW_00161].
The authors declare no conflict of interest.
Approval for the study was obtained from the Health Research and Ethics Committee of the Institute of Public Health, Obafemi Awolowo University, Ile-Ife (IPHOAU/12/2205). Permission for approval was also obtained from the Education and Development Research Committee in the Ministry of Education of the selected states, the Executive Secretary of each Local Government, Local Inspectors of Education (LIEs) and principals of the selected schools. Verbal consent/assent was obtained from participants with assurance of confidentiality.
MFO: C onceptualization; formal analysis; funding acquisition; investigation; methodology; supervision; validation; and writing of the original draft. ON: Investigation; methodology; supervision; validation and revising the manuscript. OA: Methodology; supervision and reviewing the manuscript. OO: Investigation, methodology, validation and editing of the manuscript. BP: Investigation, data curation, manuscript draft. AG: Methodology and editing of manuscripts.
We appreciate the principals and teachers of the schools who participated in the project. Our sincere thanks go to the adolescent girls who actively engaged in the project. Lastly, our gratitude extends to the field officers and research assistants whose diligence and tireless efforts ensured the seamless execution of the project.