Drug-induced sleep endoscopy, Micro camera, Medical innovation, Obstructive sleep apnea, Upper airway obstruction
Obstructive sleep apnea is a disease consisting of episodes of partial or complete closure of the upper airway that occur during sleep and lead to breathing cessation defined as a period of apnea more than 10s. Symptom include restlessness, snoring, recurrent awakening, morning headache and excessive day time sleepiness. Diagnosis of obstructive sleep apnea is based on sleep history and polysomnography [1]. Obstructive sleep apnea syndrome (OSAS) affects 6-17% of adults in global world [2].
Continuous positive airway pressure (CPAP) is the gold-standard treatment in severe OSAS. In case of intolerance to CPAP, alternative treatment is sleep surgery or dental appliance. Success of sleep surgery depends on informations about sites of collaps of upper respiratory tract during apnea attacks. Drug-induced sleep endoscopy (DISE) is a diagnostic technique for 3D dynamic anatomical visualisation of upper airway obstruction during sedated sleep. Drug-induced sleep/sedation endoscopy (DISE) or video sleep nasendoscopy, first described by Croft and Pringle in 1991, enables exploration during induced sleep [3]. DISE is usually performed in an operating room, in silence and under soft lighting. During Performing sleep endoscopy (DISE) several anesthetic drugs may be used, alone or in association. Two are particularly widely described: midazolam (Hypnovel®), the first to be used in sleep endoscopy, and propofol (Diprivan®). Others, such as diazepam (Valium®) and dexmedetomidine (alpha-2 agonist), are also used, but less widely.
Drug-induced sleep endoscopy is currently the examination that enables obstruction sites to be located under conditions best approximating natural sleep. But there are certain handicaps: The limitation of studies is the constraint in the duration of DISE not being identical to that of natural physiological sleep [4]. Another handicap of sleep endoscopy (DISE) is neccesity of an operation room and anesthesiologist staffs for performing it.
The main aims of this novel designed method are: 1- Visualization of upper respiratory tract's collaps sites during physiological sleep; 2- Elimination of neccesity of operation room and anesthesiologist staffs.
For visualizing of upper respiratory tract during physiologicaly sleep we need a camera wich should contains features bellow:
1. Opposite sides view camera heads
2. Wide angle cameras
3. Wi-Fi unit
4. Light
5. Energy source
Today there are cameras with these features using by Gastroenterologists for visualizing the intestinal system during capsule endoscopy. Colon capsule endoscopy is a wireless and minimally invasive technique for visualization of the whole colon [5]. These cameras are not small enough for visualizing upper respiratory tract. In Figure 1 we could see one of these cameras (Figure 1). In a capsule endoscopy camera there are spaces between camera head and outer sites of device in each end. Every space's length is 5.6 mm. There are betteries inside the device is enough for 8 hours. Batteries length is up to 10 mm (Figure 2). The camera wich could use for visualizing the upper respiratory tract needs batteries just for 20 minutes. It doesn't need the spaces between camera head and outer layer of device. It could be at least 16-20 mm shorter than the camera wich uses during capsule endoscopy. The mini camera should have clipses at it's board of back side for attaching to soft tissues (Figure 3).
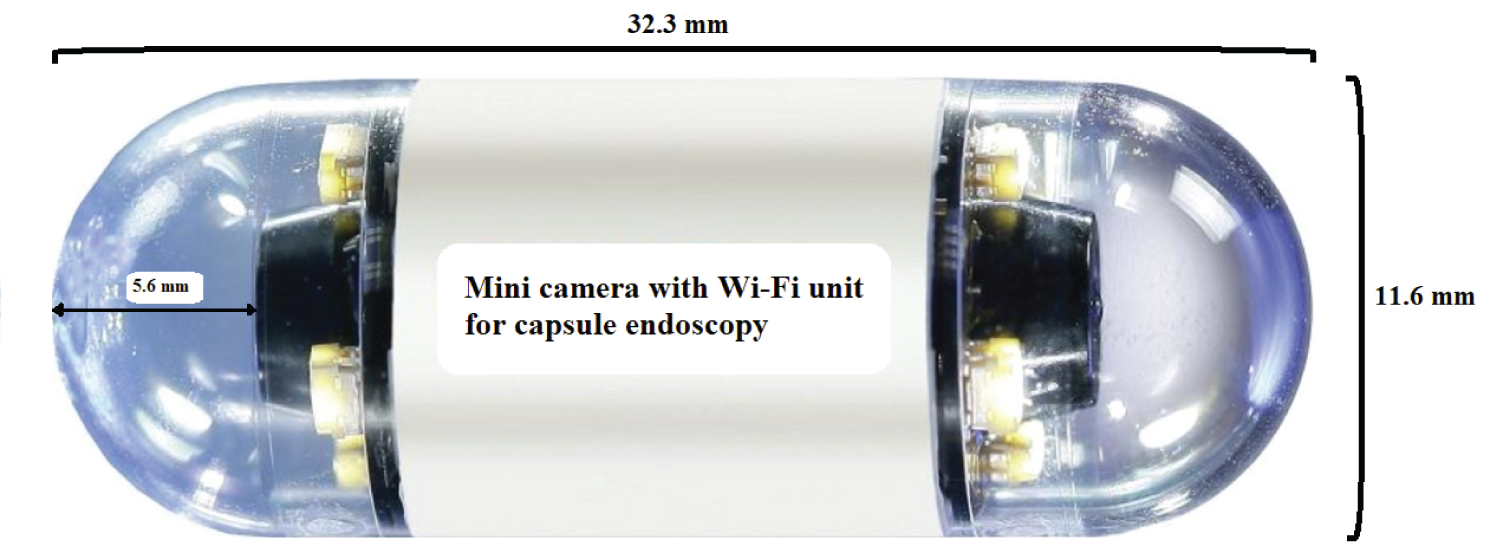 Figure 1: Mini camera with Wi-Fi unit for capsule endoscopy.
View Figure 1
Figure 1: Mini camera with Wi-Fi unit for capsule endoscopy.
View Figure 1
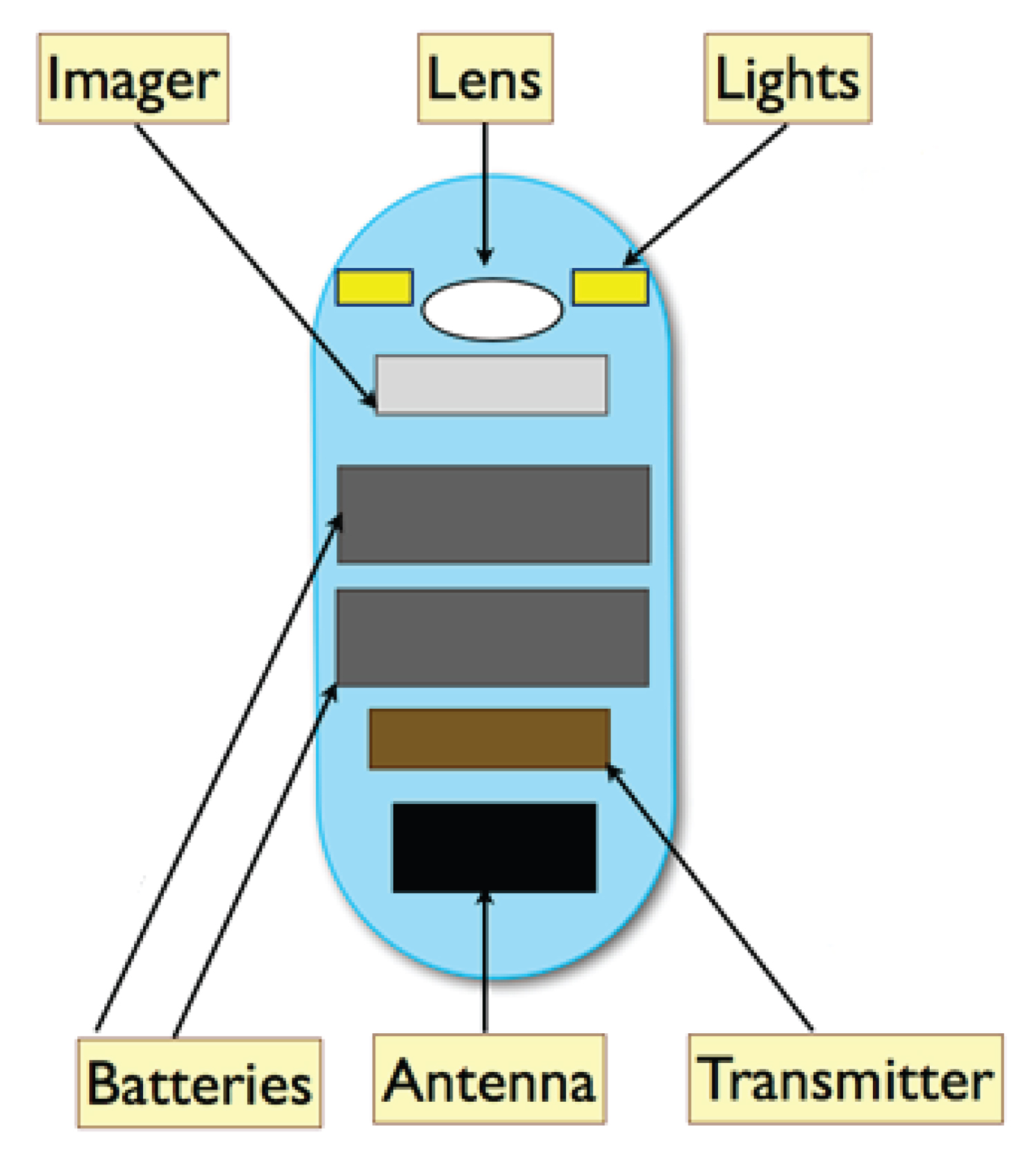 Figure 2: Capsule endoscopy camera.
View Figure 2
Figure 2: Capsule endoscopy camera.
View Figure 2
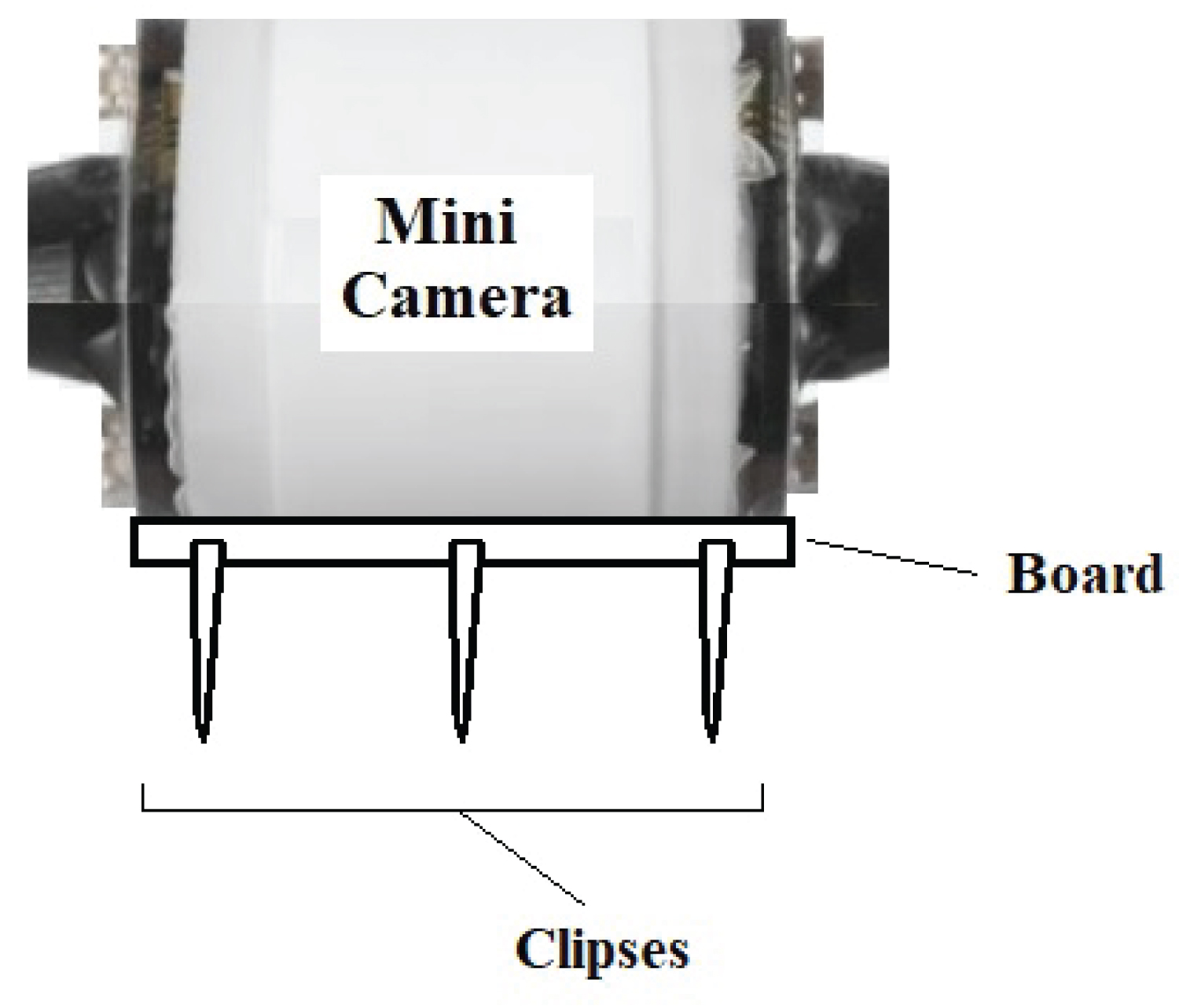 Figure 3: Mini camera.
View Figure 3
Figure 3: Mini camera.
View Figure 3
For visualizing the collapse sites of upper respiratory tract during physiological sleep the camera should attached by clipses of mini camera to the posterior pharyngeal wall, between level of velum and level of base of the tongue under topical and local anesthesia (Figure 4). During physiological sleep after apnea attacks begin, a sleep technician should start the camera. 15-20 minuets recording of movments of upper respiratory tract sites could show us the behaviour of tissues during apnea attacks.
 Figure 4: Working procedure of mini camera.
View Figure 4
Figure 4: Working procedure of mini camera.
View Figure 4
This designed method could give us apportunity of observing the upper respiratory tract collapse sites for first time during physiological sleep.