In sleep apnea/hypopnea syndrome (SAHS) a superior airway collapse can occur in the anteroposterioror lateral direction. The primary or secondary decrease in the tone of the dilating muscles of the pharynx, due to the negative pressure produced by the contraction of the diaphragm cause the collapse. Pharyngoplasty surgical techniques try to improve lateral collapse by repositioning the muscles that constitute the pharyngeal lateral wall, mainly the palatopharyngeal (PP), palatoglossal (PG) and upper constrictor (UC).
To determine the effectiveness of pharyngoplasty to improve sleep apnea-hypopnea syndrome (SAHS) in patients who did not tolerate or refused treatment with continuous positive airway pressure (CPAP).
Prospective and descriptive.
Patients with SAHS who did not tolerate or refused CPAP treatment were included, and were treated by some of the pharyngoplasty surgical techniques at the Hospital Italiano of Buenos Aires between march 2011 and october, 2018.
We consider that there was an improvement when the postoperative apnea/hypopnea index (AHI) was reduced by 50% and was less than 10, this decreases cardiovascular risk in patients with SAHS. If it was less than 5, it was considered that they were cured.
Twenty-four patients with SAHS were treated with pharyngoplasty techniques. Fifteen performed postoperative polysomnographic studies and were included in the study. Eight sphincter pharyngoplasty, 3 lateral pharyngoplasty and 4 combinations of sphincter and lateral pharyngoplasty were performed. Considering a reduction in AHI > or = 50%, 9 patients (60%) improved. If a 50% reduction in AHI is considered, but leaving this index equal or below 10, eight patients had an improvement (53.33%).
The AHI reduction of 50% and below 5 (cure) was obtained in 4 patients (44.44%).
With different techniques of pharyngoplasty we obtained an improvement of 53.33% (8/15) considering as an improvement a reduction of the AHI of 50% and less than 10. The AHI reduction of 50% and below 5 (cure) was obtained in 4 patients (44.44%). We believe that the sphincter pharyngoplasty technique has lower morbidity and is equal to or more effective than lateral pharyngoplasty to treat patients with SAHS who cannot use CPAP. The combination of lateral pharyngoplasty and sphincter pharyngoplasty surgery does not necessarily mean a better result, but possibly increases complications.
Pharyngoplasty, Sphincter pharyngoplasty, Sleep apnea
The collapse of the upper airway that occurs in patients with sleep apnea (SAHS) can be anteroposterior or lateral.
The importance of lateral collapse is demonstrated by seeing how continuous positive airway pressure (CPAP) acts by dilating the airway mainly laterally.
Most of the surgical techniques used to treat patients with SAHS act by modifying the anteroposterior collapse.
Pharyngoplasty are surgical techniques designed to treat the lateral collapse of the pharyngeal wall, modifying the position and the action of the muscles of that region.
To determine the effectiveness of pharyngoplasty to improve sleep apnea-hypopnea syndrome (SAHS) in patients who did not tolerate or refused treatment with CPAP.
Prospective and descriptive.
Patients with SAHS who did not tolerate or refused CPAP treatment were included, and were treated by some of the pharyngoplasty surgical techniques at the Hospital Italiano of Buenos Aires between march 2011 and october, 2018.
Patients who had an apnea/hypopnea index (AHI) of less than 10, patients with SAHS treated with other surgical techniques, and those who did not perform a postoperative control polysomnography were excluded.
Body mass index (BMI) was less than 30 in all patients.
The data collected and evaluated in the patients were: Age and sex, Mallampati index, size of tonsils and uvula (Friedman scale), AHI, rejection or non-tolerance to CPAP, BMI, pharyngoplasty surgical technique, complications, and results (AHI according to PSG postoperative, after 6 months).
They were noted in a Microsoft Office Excel 2010 table.
The following classification was used to establish the SAHS grade according to the apnea/hypopnea index: Mild (AHI: 5-14.9), moderate (AHI: 15-29.9) and severe (AHI > 30).
The evaluation of the patients included: Clinical history with Epworth scale, ENT exam assessing the size of the tonsils (grade 1-2-3-4), uvula and features of the palate veil, tongue position according to modified Mallampati classification (Friedman scale), determination of body mass index, rhinofibrolaringoscopy with Muller's maneuver and nocturnal polysomnography with oximetry performed in a sleep laboratory or with portable home equipment.
All were operated under general anesthesia.
The surgical techniques used to treat lateral pharyngeal collapse consisted of resecting the tonsils or mucosa between the pillars, dissecting the palatopharyngeal muscle bilaterally (posterior pillar), sectioning it at its lower end and rotating it to suture it anteriorly, superiorly and laterally in the palate with resorbable material preferably at the level of the pterygomandibular raphe (sphincter pharyngoplasty) (Figure 1).
 Figure 1: Sphincter Pharyngoplasty (A) Palatopharyngeal muscle (PP) dissection; (B,C) Lower section and upper and lateral muscle rotation; (D,E) PP muscle suture on the palate; (F) Deep suture of the PP muscle to the pterygomandibular raphe (Sorrenti modification).
View Figure 1
Figure 1: Sphincter Pharyngoplasty (A) Palatopharyngeal muscle (PP) dissection; (B,C) Lower section and upper and lateral muscle rotation; (D,E) PP muscle suture on the palate; (F) Deep suture of the PP muscle to the pterygomandibular raphe (Sorrenti modification).
View Figure 1
Section of the superior constrictor muscle of the pharynx, lateral constrictor suture to the palatoglossal muscle and mucous suture of the tonsillar fossa (lateral pharyngoplasty) (Figure 2), and combination of lateral pharyngoplasty without suture of the lateral sector of the superior constrictor muscle and sphincter pharyngoplasty.
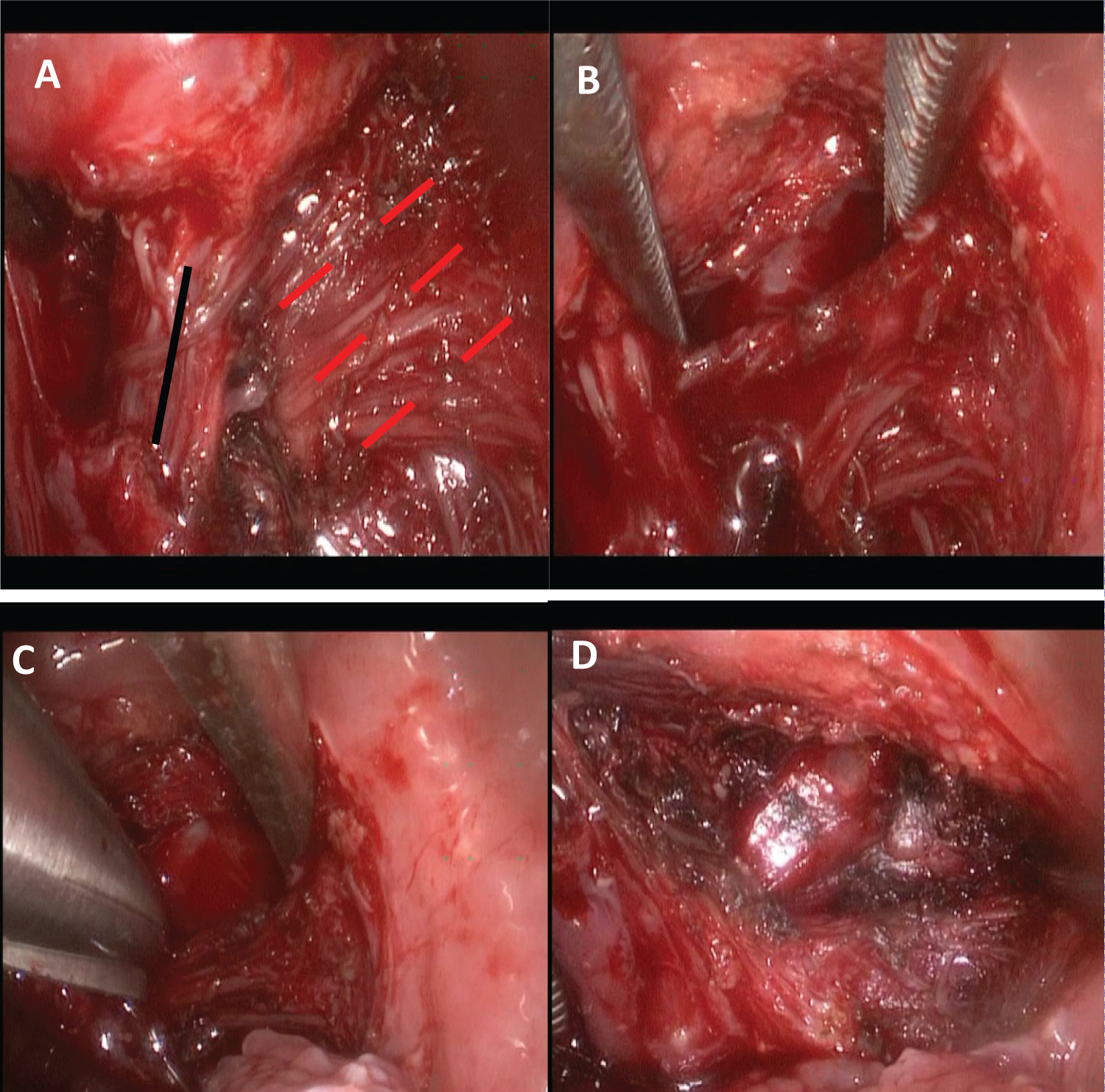 Figure 2: Lateral Pharyngoplasty (A) Vertical black dotted line: palatopharyngeal muscle, horizontal red lines: Upper constrictor muscle of the pharynx; (B, C, D) Constrictor muscle section.
View Figure 2
Figure 2: Lateral Pharyngoplasty (A) Vertical black dotted line: palatopharyngeal muscle, horizontal red lines: Upper constrictor muscle of the pharynx; (B, C, D) Constrictor muscle section.
View Figure 2
All patients were hospitalized for 24 hours in an intermediate therapy unit.
A post-operative PSG was requested in all after 6 months of surgery.
It was considered that there was improvement when the postoperative AHI was reduced by 50% and was less than 10, this decreases cardiovascular risk in patients with SAHS and healing when the AHI was = or < to 5.
Twenty-four patients with SAHS were treated with pharyngoplasty techniques.
Twenty were men and four women, the oldest was 71-years-old and the youngest 26, the average age was 48 years.
Considering the position of the tongue, and the size of the tonsils, the staging of the patients (Friedman) was: stage I: 1/15, stage II: 5/15, and stage III: 9/15.
A lateral collapse in the pharyngeal wall was diagnosed in all patients by rhinofibrolaringoscopy with Mueller's maneuver.
According to the PSG, moderate SAHS was diagnosed on 7/15 and severe SAHS on 8/15 (Figure 3).
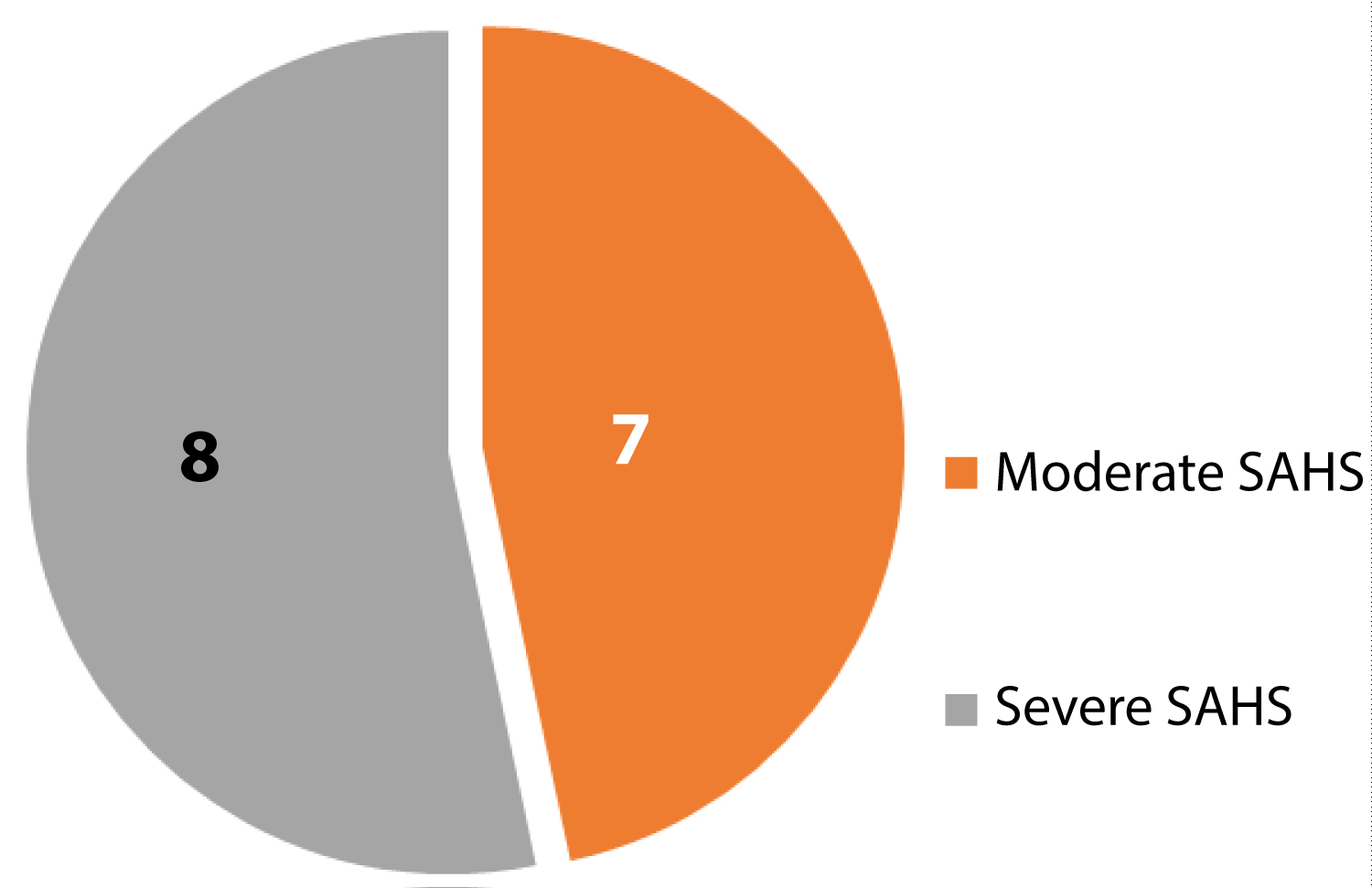 Figure 3: Distribution of patients according to SAHS severity.
View Figure 3
Figure 3: Distribution of patients according to SAHS severity.
View Figure 3
Eight sphincter pharyngoplasty, 3 lateral pharyngoplasty and 4 combinations of sphincter and lateral pharyngoplasty were performed.
In two patients, a septoplasty and submucosal bilateral inferior turbinoplasty with coblation were associated and in another, a reduction of a lingual tonsil hypertrophy with CO2 laser.
Considering a reduction in AHI > or = 50%, 9 patients (60%) improved.
If a 50% reduction in AHI is considered, but leaving this index equal or below 10 (decrease in cardiovascular risk) 8 patients had improvement (53.33%).
The AHI reduction of 50% and below 5 (cure) was obtained in 4 patients (44.44%).
Of the 6 patients who did not have a 50% reduction in AHI, two had an equal postoperative index, two were worse and in two the improvement was partial (it did not reach a 50% reduction in AHI) (Figure 4).
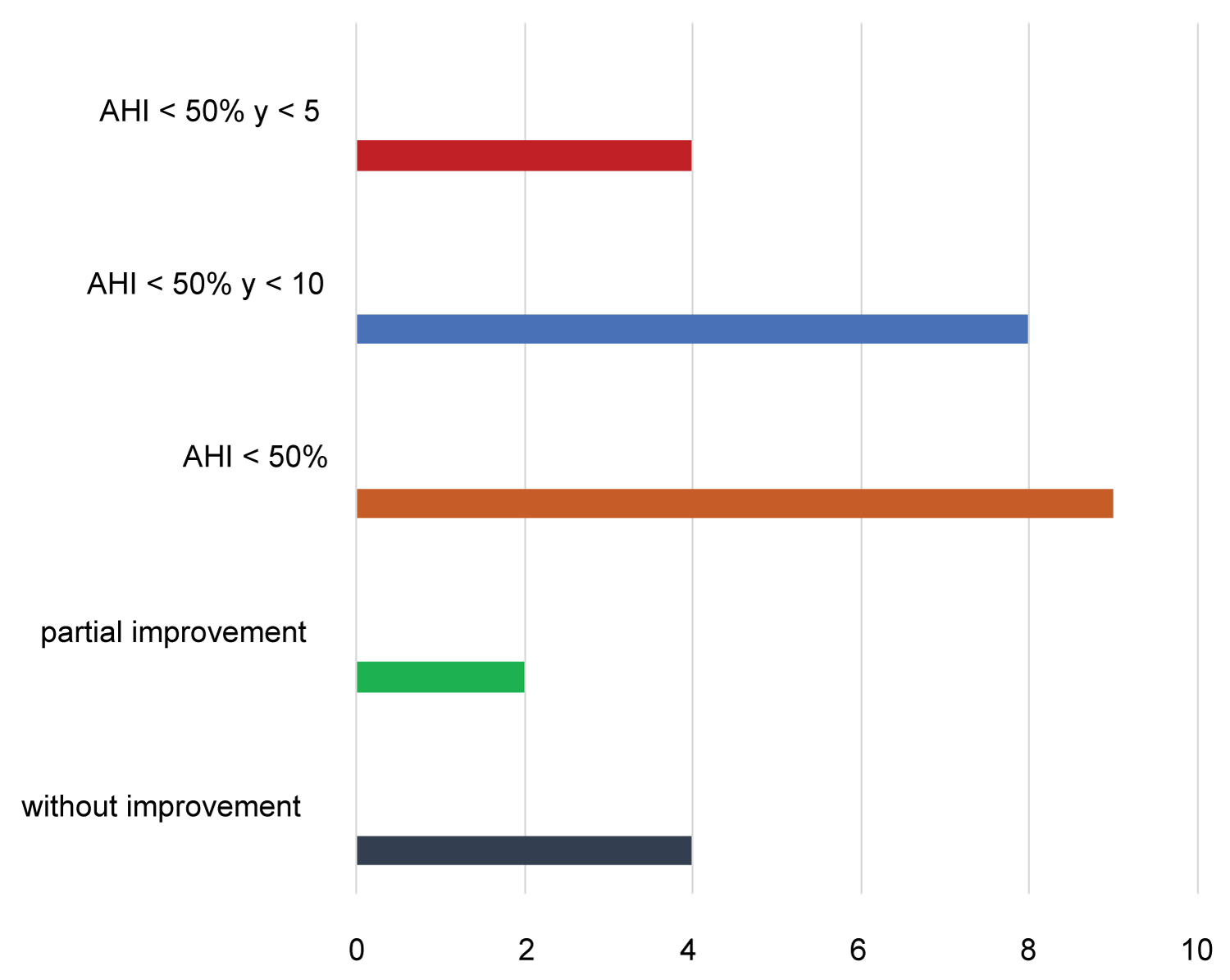 Figure 4: Results of treatment in patients with SAHS with pharyngoplasty surgical techniques.
View Figure 4
Figure 4: Results of treatment in patients with SAHS with pharyngoplasty surgical techniques.
View Figure 4
There were two postoperative complications: Bleeding 14 days after surgery and a velopalatine insufficiency that resolved within 30 days. The two complications occurred in patients in whom a lateral pharyngoplasty was combined with sphincter pharyngoplasty.
The muscles that constitute the lateral wall of the pharynx are horizontal: Upper, middle and lower constrictors, and vertical: Salpingopharyngeal, palatoglossal (constitutes the anterior tonsillar pillar) and palatopharyngeal (posterior tonsillar pillar).
The constrictor muscles act by facilitating the entry of the food bolus into the esophagus and the palatoglossus (PG) and palatopharyngeal (PP) elevate the lateral wall of the pharynx and partially the tongue when swallowing, shortening the pharynx and medializing the lateral wall.
During breathing, the longitudinal traction of the pharynx stiffens the PP muscle and reduces compliance of the palate and pharynx. The transverse fascicle of the PP acts as a sphincter of the nasopharynx. The respiratory function of PG is unknown [1].
Surgeries designed to treat patients suffering from SAHS have evolved in the last 20 years. The surgeries indicated on the palate have changed from resective to conservative, trying to preserve the muscles of the palate and acting mainly on the mucosa and submucosa. Also, the concept of repositioning the muscles to modify their action and prevent collapse has been an important advance.
This concept was created by Cahali, who described the technique of lateral pharyngoplasty in 2003, which acts on the superior constrictor muscle of the pharynx [2].
Subsequently, he made several modifications to his original technique: vertical myotomy of the upper constrictor muscle in the tonsillar fossa without suture of the lateral sector, and the section of the palatopharyngeal muscle at its most caudal end, and lateral replacement of the muscle flap [3].
With his initial technique, he reported in a study on 10 patients an improvement in AHI greater than 50% in 8, a partial improvement in 1 and one patient worsened [2].
Pang and Woodson [4] subsequently described the sphincter pharyngoplasty technique. They reported in a comparative, prospective and randomized study in 45 patients with SAHS treated with uvulopalatoplasty and sphincter pharyngoplasty an improvement, considering a reduction in AHI > of 50% and < 20 of 68.1% in the group treated with UPP and 82.6% in those treated with EPP.
Subsequently, Sorrenti and collaborators [5] modified EPP, suturing the palatopharyngeal muscle deeply to the pterygomandibular raphe, and modifications also emerged using barbed sutures that wrap the palatopharyngeal muscle and fix it to the pterygomandibular raphe [6].
They obtain a reduction in AHI > 50% and < 20 in 89.2% of patients treated (n = 85) with associated nasal and hypopharyngeal surgery [5]. In pharyngoplasty performed with barbed sutures, they obtained similar results [6].
In a multicenter study on 75 patients who refused or did not tolerate CPAP and were treated with EPP, they reported 90% improvement according to Sher's criteria (AHI < 50% and < of 20) [7]. In another study, 63 patients treated with EPP reported an improvement of 67% (according to Sher's criteria) [8].
In our study we obtained an improvement in AHI in 53.3% of patients (AHI < 50% and below 10). This improvement rate is lower than that of some studies described above, we attribute it to the fact that we do not perform a sleep endoscopy (DISE) to perform the topodiagnostic of the collapse. Also, from 2017 we began to include in our study patients treated with LP and with a combination of LP (without suture of the lateral sector of the upper constrictor muscle) and EPP. Our results were lower than those obtained using only the EPP surgical technique to treat lateral pharyngeal collapse (AHI < 50% and < 10: 62.5%) [9].
We had few complications, but both occurred in patients treated with LP or combination of LP and EPP.
With different techniques of pharyngoplasty we obtained an improvement of 53.33% (8/15) considering as an improvement a reduction of the AHI of 50% and less than 10. The AHI reduction of 50% and below 5 (cure) was obtained in 4 patients (44.44%). We believe that the sphincter pharyngoplasty technique has lower morbidity and is equal to or more effective than lateral pharyngoplasty to treat patients with SAHS who cannot use CPAP. The combination of lateral pharyngoplasty and sphincter pharyngoplasty surgery does not necessarily mean a better result, but possibly increases complications.