The disadvantage of current resections, ablations, expansions, re-locations, suturing, nerves stimulation techniques or transoral robotics surgery is their invasiveness or morbidity. In contrast to this, the bipolar RF interventions respectfully to basic valuable anatomical and physiological knowledge as well to the new pathophysiological and histological research, maintain the involved anatomical structures intact and due to their simplicity and low patient impediment are still advantageous as the means of first therapeutically choice. Within this topical context the contemporary study was undertaken in an effort to re-evaluate the use and the efficacy of an already published simultaneous and/or multi-level bipolar RF own method for snoring and moderate OSA.
We present a retrospective non-randomised study of clinical cases with a trial of 90 snorers (BMI 27.3) and 26 out-patients (4 CPAP assisted) with mild (tAHI 5-15) to moderate (tAHI 16-30) OSA (BMI 31.3) operated between the years 2005 and 2012. The patients were selected by polysomnography (PSG) trial and depending on anatomical findings operated primarily in one or in two stages (nose, palate, lingual tonsils) upon local anaesthesia. To assess the critical obstructions and implicit the collapsed areas, the contacts or pressings points we routinely used both rigid and flexible (awake) video-endoscopy, occasionally rhinomanometrically valuations and in selected cases palatal MRI investigations and cephalometric radiologically measurements. A 6-12-24 month follow-up survey was carried out. The intensity as well as the snoring density was determined on a numeric analogue scale (NAS). PSG control-studies were performed by OSA patients. Histological examinations of resected uvula tissues or small biopsy of the treated palatal folds helped us to evaluate the RF effects. To compare the method`s morbidity with those of other surgical techniques actually used for the treatment of OSA, the author has reviewed and considered a large number of published works in the literature (PubMed, Excerpts, Sleep Med Rev, Oxford Academic, Sleep Research Society).
After 6 and 12 months postoperative 78% of snorers and after 24 months 69% of them, reported (NAS score 0 to 2, preoperative 3, 3) a noticeable decrease of snoring intensity or density. Moderate improvement in AHI (baseline 22, postoperative 16 ± 1) values were objectified by OSA patients. Two of them have renounced to CPAP. 50% of OSA patients felt a durable relief in the throat, reporting better oral respiration. All reported improvements in that nasal. Preoperative video-endoscopically observations were compared with those postoperative. The patient's tolerance of the procedures and local anaesthesia, respectively the acceptance of the graduate multi-level technique applications was very good. The intra- and post-operative outcome was short and fast without complications.
Multilevel bipolar RF is a low-morbidity generally office-based procedure performed with local anaesthesia and is an effective first-line treatment option generally for snoring peoples and for some patients with OSAS.
Sleep apnea syndrome, Radiofrequency surgery, Multi-level, Snoring
Since the recent evolution regarding therapeutically strategy for OSA focuses on the concept of the pharyngeal wall collapse rather than on ablation of the redundant pharyngeal soft tissue, the interest on this minimally-invasive with minor morbidity treatment procedure can be relevant. The multi-level RF method with dual probes (Figure 1) which benefit of the inherent advantages of the bipolar technology, was introduce several years ago [1-5]. The method is adapted to the anatomical and physiological peculiarity in the nasal and oropharyngeal regions [6-10] and use, with one exception, bipolar electrodes designed by the author [3] and manufactured by Sutter Medizintechnik (Freiburg, Germany). A 4 MHz Sutter generator supplied the RF energy. For relaxing the sphincter action of palato-pharyngeal muscle and reduce without cut the palatal webbing we developed later a special electrodes [3,4]. To circumvent the tongue complications reported after various treatments as well to avoid the counterproductive injury of the anti-collapse tongue intrinsic muscles, we performed and recommended to limit the tongue base reductions only on the level of the lingual tonsils [1,3]. The present retrospective non-randomised office-based trial-study re-analyse the patient tolerance to the method, the safety and the effectiveness of multi-level procedures, performed in one to three sessions. This presentation is based on personal experience and is completed by the literature review.
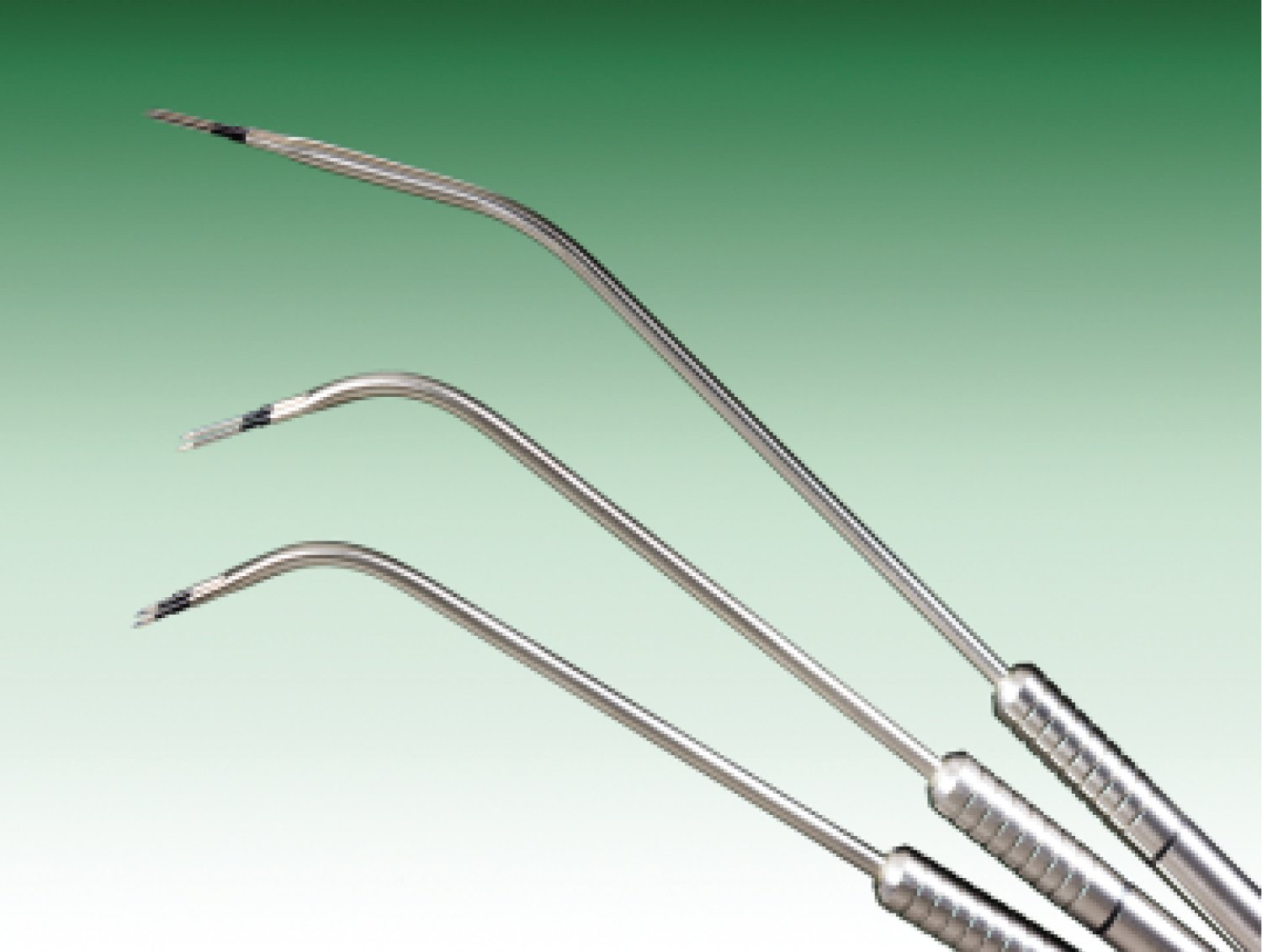 Figure 1: Multilevel bipolar electrodes.
View Figure 1
Figure 1: Multilevel bipolar electrodes.
View Figure 1
We present a retrospective non-randomised study of clinical cases with a trial of 90 snorers (Body-Mass-Index, BMI 27,3) and 26 out-patients (4 CPAP assisted) with slight (Apnea-Hypopnea Index, tAHI 5-15) to moderate (tAHI 16-30) OSA (BMI 31.3) operated between the years 2005 and 2012. 116 patients suffering from snoring and associated [11] mild OSA, fulfilling the inclusion criteria (socially disruptive snoring, moderate OSA without serious ventilation events, selected CPAP cases, patients with nasal or retropalatal obstructions, hypertrophic posterior pillars but moderate webbing, lingual tonsils hypertrophy-LHT; (Figure 2 and Figure 3) were enrolled after they underwent at least two combined (Figure 4) level-interventions in one (simultaneous) or two (different) sessions. The exclusion criteria were severe OSA, palatal tonsils hypertrophy, retrognathism, macroglossia, cardio-pulmonary diseases, diabetes, therapies with sedatives. As long the drug induced sleep endoscopy (DISE) produce a central sleep apnea syndrome, condition having no surgical therapeutically indication, exacerbate or modified the outcomes [12-14], we haven't proposed this exploration to our patients with obstructive sleep apnea. The operative indications where established subsequent polysomnographically trial and cardio-pulmonary investigations. To determine the critical obstructions levels in the upper way, as the vibrating and structures contact (sloping downward velum vs. posterior pharyngeal wall, uvula vs. tongue or epiglottis, lingual tonsils vs. epiglottis, aspiration of the uvula in the laryngeal vestibule) or the eventually collapses areas, we used routinely the anterior and posterior rhino-endoscopy (Figure 5), the pharyngo-laryngeal endoscopy and awake video-fiberscopy examinations. In the aim to determine objectively the effectiveness of the treatment, documented preoperatively video-endoscopically observations of the nasopharyngeal, velopharyngeal and retrolingual spaces, were correlated with the postoperatively findings. Polysomnography follow up studies were carried out by most OSA patients. Histological examinations of the resected uvula tissue and biopsy of treated pillar (Figure 6) helped to evaluate the RF effects. Some dysfunctional parameters assessed by the clinical examination needed others para-clinically investigations as rhinomanometry, orthodontic council, cervical or cephalometric X-rays and occasionally to ascertain soft palate and tongue base tissues profile abnormalities, also MRI (Figure 7).
 Figure 2: Retrovelar endoscopy: Slopping downward/posterior closure/collapse pre- and postoperative.
View Figure 2
Figure 2: Retrovelar endoscopy: Slopping downward/posterior closure/collapse pre- and postoperative.
View Figure 2
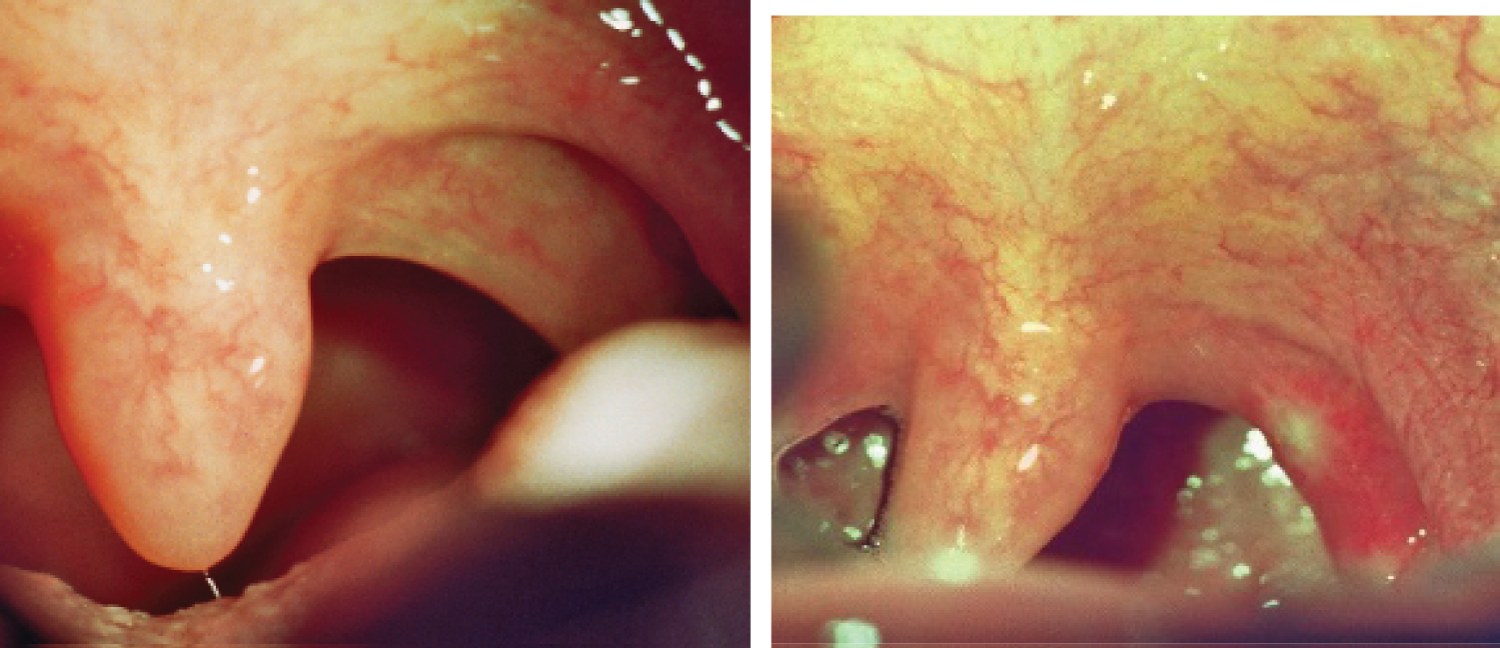 Figure 3: Hypertrophic palatopharyngeal web and muscle before and few days after transmucosal breakup of the palatopharyngeal muscle (2-3 spots along the arch).
View Figure 3
Figure 3: Hypertrophic palatopharyngeal web and muscle before and few days after transmucosal breakup of the palatopharyngeal muscle (2-3 spots along the arch).
View Figure 3
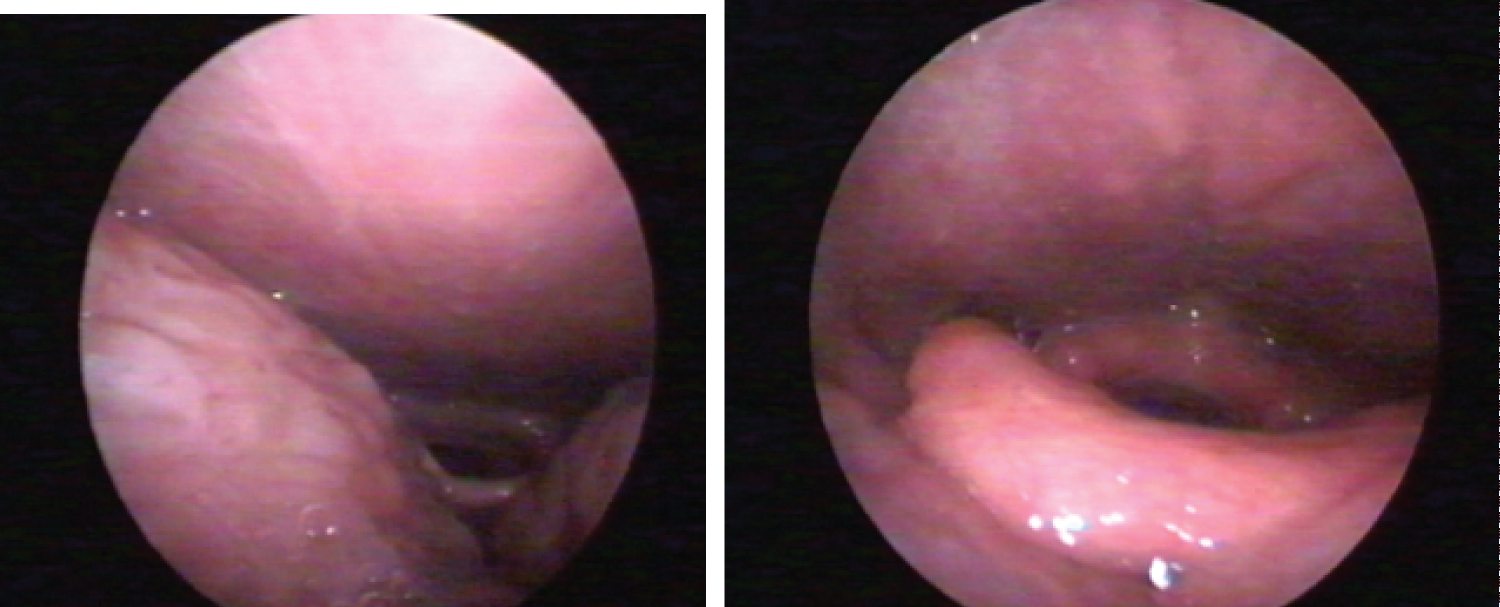 Figure 4: Three days after simultaneous vellum and para uvular webbing reduction (moderate oedema and fibrin membranes) respectively cranial retracted ("velarisation") pillar and enlarged velo-lingual distance right two weeks postoperatively.
View Figure 4
Figure 4: Three days after simultaneous vellum and para uvular webbing reduction (moderate oedema and fibrin membranes) respectively cranial retracted ("velarisation") pillar and enlarged velo-lingual distance right two weeks postoperatively.
View Figure 4
 Figure 5: Endoscopy: Lingual tonsils hypertrophy before and after volume reduction.
View Figure 5
Figure 5: Endoscopy: Lingual tonsils hypertrophy before and after volume reduction.
View Figure 5
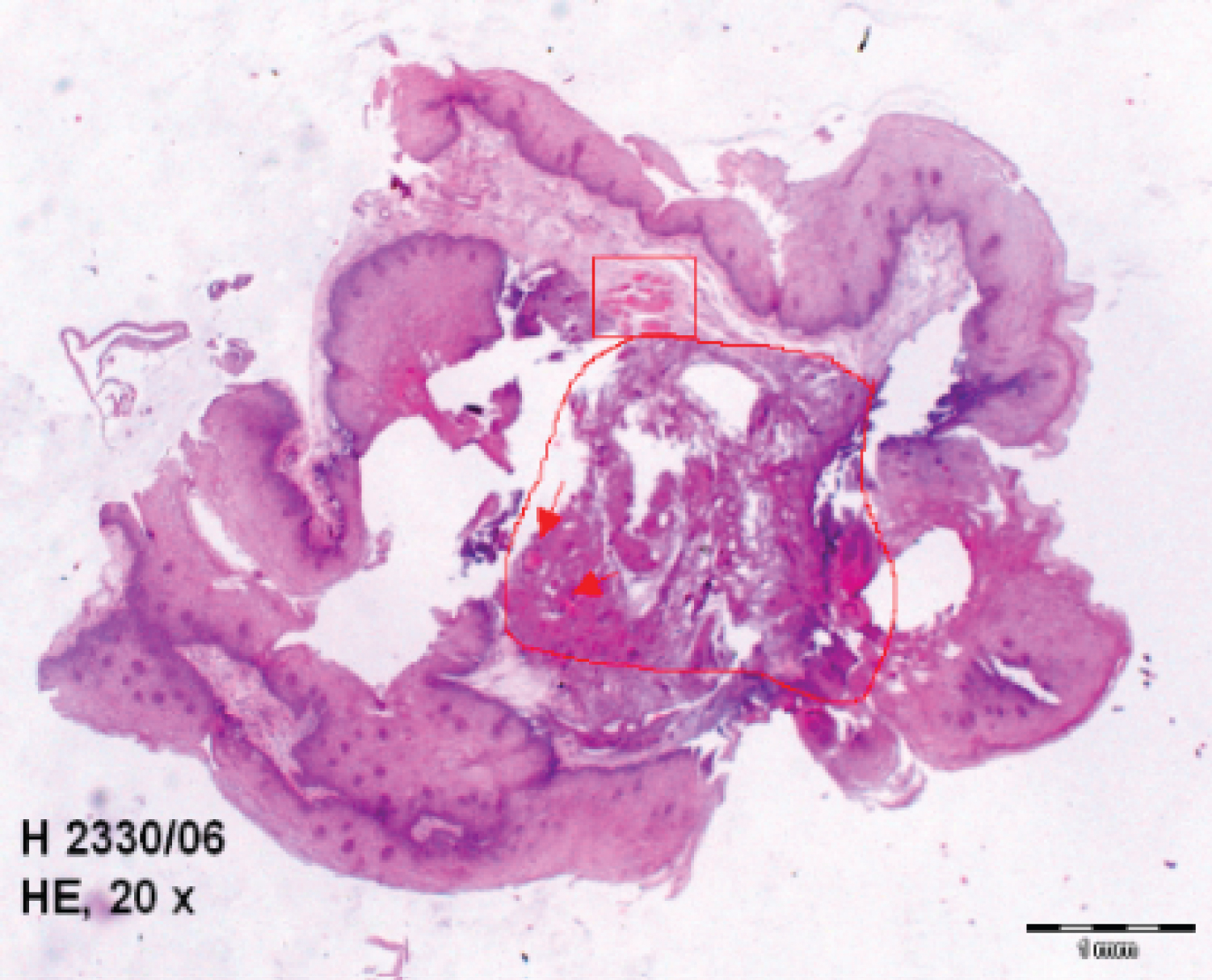 Figure 6: Palatopharyngeal arch piece microscopy after bipolar RF treatment: Central stroma coagulation and sharply circumscribed necrosis lesion in the centre (polygon), intravascular reversible fibrin and thrombosis (arrows), peripheral rest of atrophic musculature (rectangle).
View Figure 6
Figure 6: Palatopharyngeal arch piece microscopy after bipolar RF treatment: Central stroma coagulation and sharply circumscribed necrosis lesion in the centre (polygon), intravascular reversible fibrin and thrombosis (arrows), peripheral rest of atrophic musculature (rectangle).
View Figure 6
The intensity as well as the snoring density was assessed on a numeric analogue scale (NAS ranging from 0 = "patient doesn't snore anymore" to 4 = "patient continues to snore as before"), which was filled out by the partner preoperatively and postoperatively generally after 6 months. A progressive or graduate interventional sequence depending from the preoperatively findings (AHI values, nasal or retro-palatal narrowing but moderate septal deviation, functionally disturbs of the turbinate, hypertrophic posterior pillar, hypotonic palate but moderate webbing, elongated uvula, lingual tonsils hypertrophy) and patient's wish or grade of satisfaction after an eventually first stage operation, was by the physician proposed. The succession of the anatomical location or level that would be first treated by radio-frequency was decided together with the patient. The most treated structures according to our methodology where the turbinate (inclusive the posterior end in selected cases) and the soft palate (inclusive the posterior pillar sin selected cases) in ca. 70% of cases followed by the sequence turbinate + soft palate + uvula (partial uvulectomy-PU as associated operation) in ca. 20% of cases. Shared after the treated sites our survey numbers 85 turbinate, 56 soft palate, 20 posterior pillars, 22 PU (cold or RF-monopolar realized and bipolar assisted) and 9 lingual tonsils operations. In order to avoid the discomfort of an endoscopic assistance, generally necessary or preferable, the volume reduction at this last level in the conditions in which the turbinate or the soft palate were primarily operated, was performed alone, in one stage. All the operations were performed in local anaesthesia (lidocaine 1%, with adrenalin in the oropharynx, without in the nose).
The controls were followed 6, 12 up to 24 months. After 6 and 12 months postoperative, 78% of snorers and after 24 month 69% of this, reported (NAS score 0 to 2, preoperative 3, 3) a decreasing of the snoring intensity or volume (density). Fast 50% of the OSA-patients felt a relief in the throat and reported better oral respiration. 25% of the patients have amelioration on Epworth-Sleepiness-Scale (ESS) respectively on the Quality-of-Life questionnaire (from negative to indifferent or positive). All patients reported better nasal breathing while the ventilated ones improvements in CPAP compliance. Moderate improvement in AHI (baseline 22, post- operative 16 ± 2) values, and snoring/h events were objectified by OSA [11] patients.
Enlargements of the palato-lingual (due to the "velarisation" of the posterior pillars) distance and latero-lateral oropharyngeal diameter, respectively of the retropalatal and post lingual spaces with reduction of the tongue-epiglottis contacts were constantly observed (Figure 7 and Figure 8). The patient tolerance of the procedures was very good, the intra- and postoperative outcome short and simply, fast (minor and short nasal perioperative bleedings, rare postoperative rhinitis or odynophagia) deprived from complications. Following the three days after oral RF treatment, a constant but mild palatal oedema occurred. Partial uvula resections associated or not with palatal and pillars applications, caused for short time (24-48 h) some intensively pains and transient difficulties in swallowing. Postoperative discomfort, pains and ulcers on tongue base persisted more and required antibiotics and topic disinfection. The grade of patient satisfaction was high but it did not corroborated always with the slight reduction in the number of apnea events.
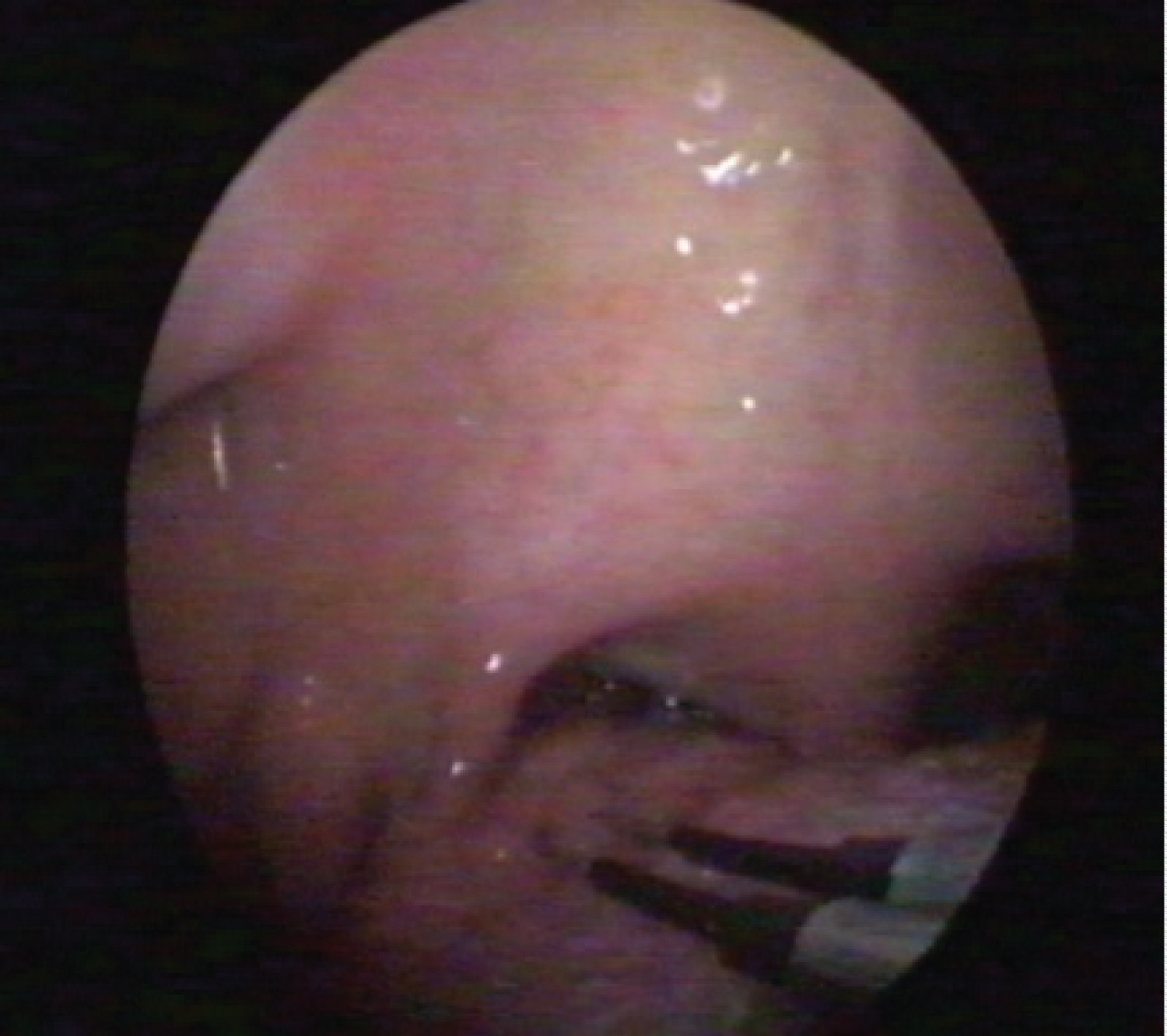 Figure 7: Fat accumulation in between degenerated fibers of tensor veli palatini; + free epiglottis, no LTH (lingual tonsils hypertrophy), wide retro- lingual space.
View Figure 7
Figure 7: Fat accumulation in between degenerated fibers of tensor veli palatini; + free epiglottis, no LTH (lingual tonsils hypertrophy), wide retro- lingual space.
View Figure 7
 Figure 8: Endoscopy: Use of the bipolar electrode on the base of the tongue tonsils.
View Figure 8
Figure 8: Endoscopy: Use of the bipolar electrode on the base of the tongue tonsils.
View Figure 8
New pathophysiological and technological researches influenced the disappearance of some old methods and determined the emergence of novels. Several factors have influenced the actual surgically management or strategy in the treatment of Obstructive Sleep Apnea Syndrome (OSAS) and Snoring:-
• The decline of classical pharyngoplasty (UPPP). The American Society of Anesthesiology reported in 2006 a general complication rate after surgery for OSA of over 10% [15]!
• The introduction of new pharyngoplasty techniques (expansion sphincter, lateral, anterior, barbed suture, etc.) some of that focusing the struggle against the collapse, rather than aggressive resected, understanding that "the lateral or superior injury of the elevating and stretching muscles, can diminish his tonus and project the vellum dorsally accentuating the obstruction and implicit the collapse at this level" [6].
• The generally let-down of the tongue base (corpus linguae) surgery (midline glossectomy, lingualplasty, lingual lightening and radiofrequency intra linguae applications [16]) due to its complications or functions trouble of the genioglossus muscle (following iatrogenic inevitable injury), lack of clear effectiveness and the need to novel strategy.
• The introduction of the radiofrequency lingual tonsils volume reductions [1,17] which preserve the tongue protrusions muscles intact or some radically lingual tonsillectomy via coblation [15,18] or diode-laser, procedures general validated as indicated therapeutically attitudes.
• The successfully revitalising of ingenious hypoglossal nerve stimulation [19] and the introduction of the high technological transoral robotic surgery (TORS) intended for tongue base resection procedures [20].
• The spreading of sleep endoscopy and the understanding that "OSA is a complex and multi-factorial disorder consisting of anatomical and non-anatomical features".
Authors [7] suggest that OSAS is due to a combination of both anatomically airway narrowing and abnormal upper way neuromotor tone follow-on growing critical tissue pressure (Pcrit). Upper airway occlusion in obstructive sleep apnea has been attributed today to "a decline in pharyngeal neuromuscular activity" occurring in "a structurally narrowed airway" [21-23]. The OSA and Snoring patients may have significant histological and microstructural alterations in soft palate and uvula. Authors as Woodson, Edstrom, Friberg, Metternich, Sambataro and others describe, processes of denervation, neurogenic inflammation, fat degeneration and muscular atrophy" [22,24,25] or "abnormal vascular reactions" [26]. The large recognition of multi-obstructive and collapse sites followed by a numerous multi-level upper airway contemporary therapeutically models the changes of attitude in the patients with moderate symptoms toward extensive surgery (generally interested in simply and office based operations). According to authors as YP Krespi "the office-based surgery underwent significant changes due to the development and use of new or innovative technology that allows physicians to perform safe, cost-effective, and rapid office procedures with equivalent, if no better, clinical outcomes".
Expansion sphincter pharyngoplasty: Necessity previous a tonsillectomy, but this, one accomplished, can improve by itself the "quality" of the lateral wall. Enlarging per se the isthmus faucium, the tonsillectomy reduces the collapse and can make the sphincteroplasty inutile [27].
TORS for OSA (tongue base resections, da Vinci system): Transoral robotic surgery can represent the definitive treatment in hypertrophy of the lingual tonsil [20]. Three large studies inform significant decrease in AHI but reported also on their total complication rates with "an average of 22.3%" [20,28]. 6% patients showed significant aspiration on gastrographic examination after 1 week". Bleedings rate: 4.2% (A Systematic Review and Meta-Analysis, 2016). "However, the cost and morbidity may be greater than with other techniques offsetting its advantages in visualization and precision "conclude some Authors. For others the morbidly is "acceptable", the operating costs can be relatively high although the advantages to patients seem to justify the procedure "[29].
Coblation of the lingual tonsils: Need generally anaesthesia. According authors it is an efficient resection method capable to reduce manifestly the AHI [15,18,30]. A relatively high rate of postoperative haemorrhage concerning palatal or lingual surgical involvements was in the literature (2.8%, 3.2%, 7.3%, 8.5%, respectively 14.81%) differently observed. The most bleedings cases needed re-interventions [29,30]. The lingual tonsils are poly-morphic lymphoid structures closely adherent to the genioglossus muscle [10]. The tongue aponeurosis is missing exactly at this level and as a practically result it is very difficult to dissect the lingual tonsil without causing underlying morphological and functionally possible contractions damages (Figure 9).
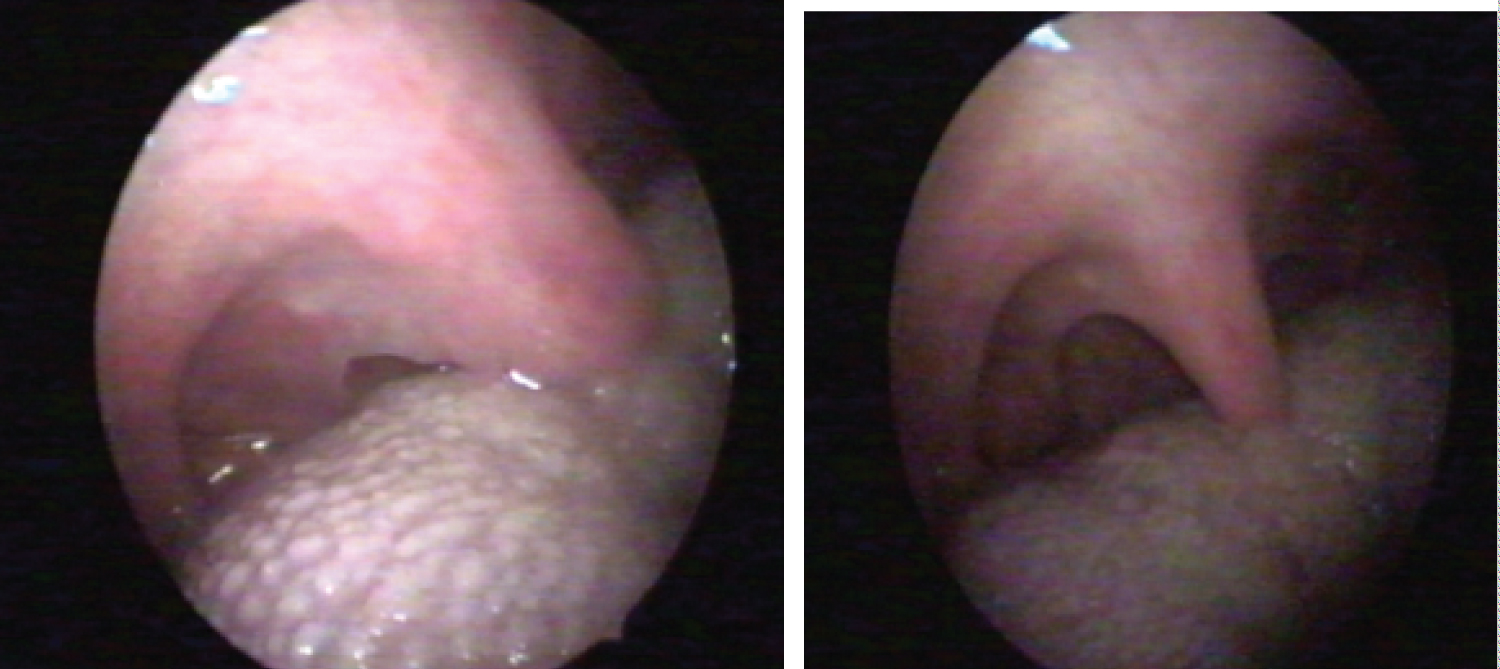 Figure 9: Endoscopy one month after parauvular treatment a): Enlargements of the velolingual distance; b) Previous situation (one week after the intervention).
View Figure 9
Figure 9: Endoscopy one month after parauvular treatment a): Enlargements of the velolingual distance; b) Previous situation (one week after the intervention).
View Figure 9
 Figure 10: Tongue muscles distribution according to R. Putz and R. Pabst in Sobotta Atlas of Anatomy.
View Figure 10
Figure 10: Tongue muscles distribution according to R. Putz and R. Pabst in Sobotta Atlas of Anatomy.
View Figure 10
Barbed sutures and relocation pharyngoplasty: It is hard to believe that the resections or sutures on soft palate doesn't interfere with the fine muscles structures. The anatomy of vellum teaches us that no really a dissection of the mucosa is possible. This one is intimately adherent and intricate to the muscles fibbers [6]. This method, in spite of same statements, can cause velopharyngeal insufficiency in terms of voice, nasality and articulations.
The Hypoglossal Nerve and Genioglossus Muscle Stimulation (HNS): The literature review confirm ongoing it good functionally results in the management of mild-to-severe OSA recommending it as second line therapeutically option. Contraction of the genioglossus muscle has been shown to improve upper airway patency [19]. A MAUDE database review [31] consider that patient adherence to treatment has been found to be as high as 86% after 12 months of therapy. However, a number of inherent technical difficulties and complications still exist and several anatomically or pathophysiological features (large palatal or lingual tonsils, important webbing, patients with complete concentric collapse of the retropalatal airway) are considered contraindications or exclusions from unilateral stimulation. Some authors as for example reported serious device-related adverse events as infection and dislodgement, removals or replacements factors "that may preclude a subset of patients from considering this therapy". Interesting can be the search of the FDA MAUDE data base [32], conducted from January 2000 to May 2020 which include "196 reports of adverse events associated to the implantable hypoglossal nerve stimulator: Most commonly, infection (34.2%), neuropraxia (15%), hematoma/seroma (11.6%). A total of 83 adverse events (42.3%) required reoperation, explantation, device repositioning/lead revision and most common replacement for device malfunction". The same search reported about "some complications not witnessed in previous large-scale clinical trials included pneumothorax, pleural effusion, and lead migration into pleural space". Lastly, a current randomized controlled study testimony the effectiveness in 89 patients who were already supplied with the HNS therapy. According to the authors, implant or therapy-related complications did not occur in the course of the study [33].
Well tolerated and fast deprived of complications is suitable for an office-based surgically approach in local anesthesia.
It employs the same types of instruments on all levels.
The dual needle electrodes configuration guarantee a precise limited coagulation followed by fibrosis and volume reduction without cut, resection or scars.
From the physio-anatomically point of view the method represent an appropriate but conservative therapeutically response to the complexes snoring mechanism which involve the "nose, the soft palate, the uvula, the tongue and the epiglottis" and a carefully surgical treatment alternative to the somnologycally recognized obstructions segments or critical points in the nasal and oropharyngeal region which can produce "peaks of upper airway resistance followed by increased negative pressure and collapsibility in OSA patients to some level" [14].
Preserve intact the nasal mucosa, the swallowing, the phonation and others functions of the soft palate with its "good" muscles as well the integrity of the tongue aponeurosis and that of the protrusions tongue muscles.
It is not a standard (multiple levels of obstructions sure exist but not all are equally important and all present by the same person) method. Each reproducible technique can be gradually applied, combined or associated with others surgeries in various multi-levels concepts but keep free the place for more radical methods, if necessary.
The turbinate's' and vellum volume reduction improve the CPAP compliance in a simple way, while reasonable reductions of the lingual tonsils (Friedman III-IV) and velar webbing might prepare the way, otherwise contraindicate, toward hypoglossal stimulation. A comparative study [20] considers the obtained results after the use of bipolar RF-palatal surgical techniques better as those obtained after the functional expansion pharyngoplasty operations.
Each segmental techniques, has proven to be a safe, simply, fast and effective mean for the treatment of snoring and selected cases of mild OSA. The main indication of this low-morbidity method, remain the snoring where could be considerate as being the procedure of first choice. Reducing the three soft obstructions sites in the upper airway by OSA patients the method improves the air flow and ameliorate even if moderate the AHI. The patient's tolerance of the procedures and local anesthesia, respectively the acceptance of the gradually approach was very good.
The author of this study declares no conflict of interests.
Excerpts presented at the 9th ISSS International Surgical Sleep Society Meeting, 5-7 April 2018 Munich.