Objectives: First-in-human evaluation of a novel magnetic apnea prevention (Magnap) device for obstructive sleep apnea (OSA) treatment was disrupted by the COVID-19 pandemic which negatively impacted the ability to track patient outcomes with in-lab polysomnograms (PSG). The objective of this study is to report the modifications undertaken in response to COVID-19 and to discuss the feasibility of home sleep apnea testing (HSAT) to monitor novel OSA therapies.
Methods: HSAT was used as an adjunct for in-lab PSG in an ongoing Phase I clinical trial of the Magnap device conducted from July 2016 to July 2022. Study participants included patients aged 21-70 years with moderate-to-severe OSA and continuous positive airway pressure (CPAP) intolerance. Participants received the internal magnetic implant and instruction on use of the paired external magnetic brace during sleep periods. Pre-COVID-19, participants underwent four in-lab PSGs post-implantation. Post-COVID-19, social distancing modifications adopted HSATs in lieu of in-lab PSGs.
Results: Seven patients (mean BMI 27.6 ± 2.5 kg/m2; mean apnea-hypopnea index, AHI 33.4 ± 17.4 per hour) completed the full study period and five successfully adopted HSAT to complete the study. HSAT introduction led to an increase in the mean number of sleep studies per participant from 3.2 to 33. There were no serious adverse events in this study.
Conclusions: The results of this interim report suggest that HSAT can be safely used as a remote adjunct for sleep-related outcome monitoring of novel OSA therapies which has important implications in the monitoring of novel and existing OSA therapies.
Obstructive sleep apnea, Magnetic apnea prevention, Magnap, Home-based sleep apnea testing
AASM: American Academy of Sleep Medicine; AHI: Apnea-Hypopnea Index; BMI: Body Mass Index; CPAP: Continuous Positive Airway Pressure; FDA: Food and Drug Administration; HSAT: Home-Based Sleep Apnea Testing; IQR: Inter-Quartile Range; Magnap: Magnetic Apnea Prevention; OSA: Obstructive Sleep Apnea; PSG: Polysomnogram; SD: Standard Deviation; UCSF: University of California San Francisco
Approximately 20 million adults in the United States suffer from at least moderate obstructive sleep apnea (OSA), characterized by an apnea-hypopnea index (AHI) of 15-29.9 per hour [1,2]. This can cause various adverse effects ranging from daytime sleepiness to cardiovascular morbidity [3-6]. The most common treatment for OSA is continuous positive airway pressure (CPAP), but many patients struggle to adhere to this therapy [1]. Thus, alternative therapies that facilitate patient comfort and ease of use are needed.
The magnetic apnea prevention (Magnap) device explores the use of magnetic force to treat OSA. Magnap functions by attracting an implanted hyoid magnet with the sufficient force (2N) to keep the airway open. Preclinical cadaver-model studies demonstrated that the Magnap device achieves an optimal force vector on the hyoid bone to keep the airway opens [7]. After investigational device exemption was obtained, a Phase I clinical trial was initiated to evaluate safety and feasibility during device implantation and device use (Supply file 1).
During the course of this trial, the COVID-19 pandemic profoundly impacted healthcare research as ongoing clinical trials were suspended or terminated due to a sharp decline in access to in-person or hospital-based treatment monitoring due to safety concerns [8]. This delay allowed alternative approaches for treatment monitoring to be explored and home-based sleep apnea testing (HSAT) was adopted as a viable adjunct to in-lab polysomnography (PSG) [9,10]. The CONSERVE-SPIRIT guidelines have allowed teams to share trial protocol modifications that may better inform and aid ongoing studies [8]. The purpose of this interim report is to report the clinical trial modifications undertaken in response to the COVID-19 pandemic and to introduce HSATs as a feasible monitoring adjunct in the evaluation of the novel Magnap device for OSA treatment. Our experience may better inform ongoing and future clinical trials evaluating novel OSA therapies. Per FDA regulatory guidance, until completion of the trial, comprehensive individual participant data on safety and efficacy will remain confidential (Supply file 2).
The Magnap system contains an internal magnetic implant and an external magnet in a customized neck brace (Figure 1). Each component contains a neodymium-iron-boron rare earth magnet encased in titanium, with a unidirectional back-plate (Figure 1). The brace is worn during sleep to prevent airway collapse by attracting the internal hyoid magnet with sufficient force to keep the airway open (Figure 2). Preclinical studies in a human cadaver model demonstrated significant improvement in critical airflow and airway patency with the Magnap system [7]. The Magnap system achieves a perpendicular force vector, resulting in increased airflow and airway patency compared to alternative therapies [7] (Figure 3).
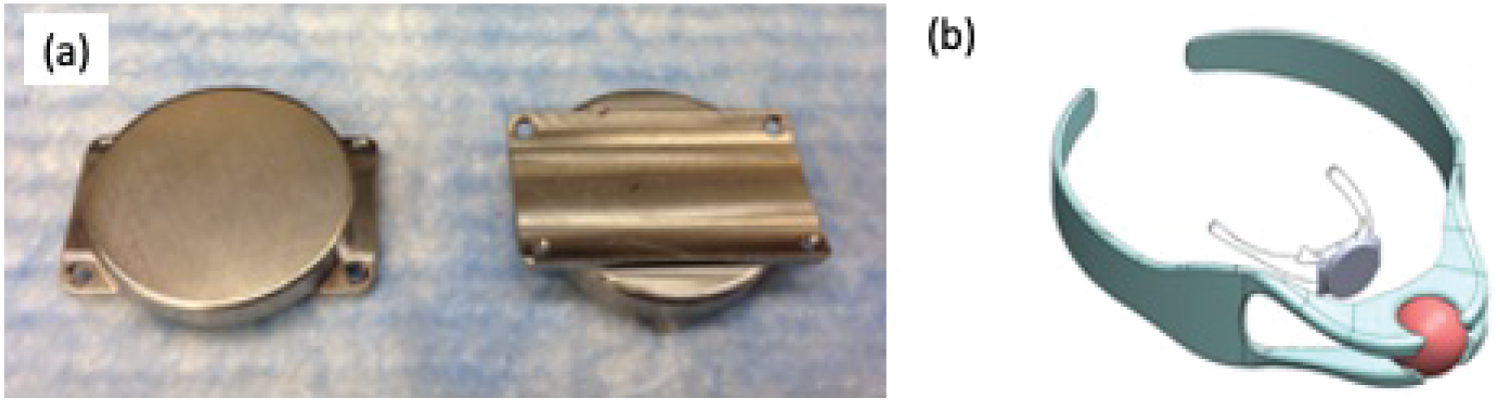 Figure 1: a) Internal implant; b) Schematic of internal magnetic device implanted onto the hyoid bone and paired external magnetic brace to be worn during sleep.
View Figure 1
Figure 1: a) Internal implant; b) Schematic of internal magnetic device implanted onto the hyoid bone and paired external magnetic brace to be worn during sleep.
View Figure 1
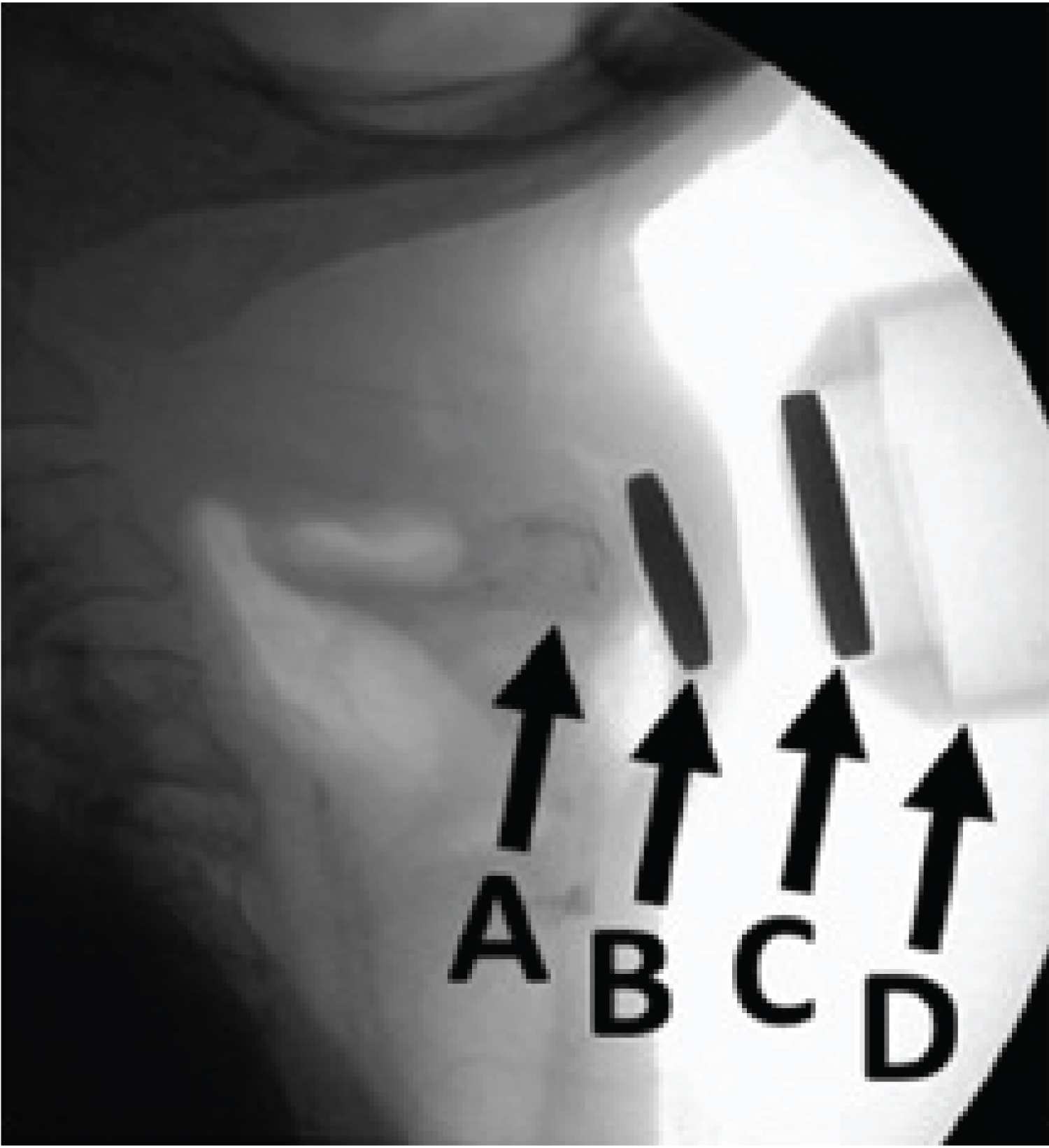 Figure 2: Lateral radiograph with (B) internal magnetic device implanted onto the (A) hyoid and (D) external neck brace containing (C) paired external magnetic device.
View Figure 2
Figure 2: Lateral radiograph with (B) internal magnetic device implanted onto the (A) hyoid and (D) external neck brace containing (C) paired external magnetic device.
View Figure 2
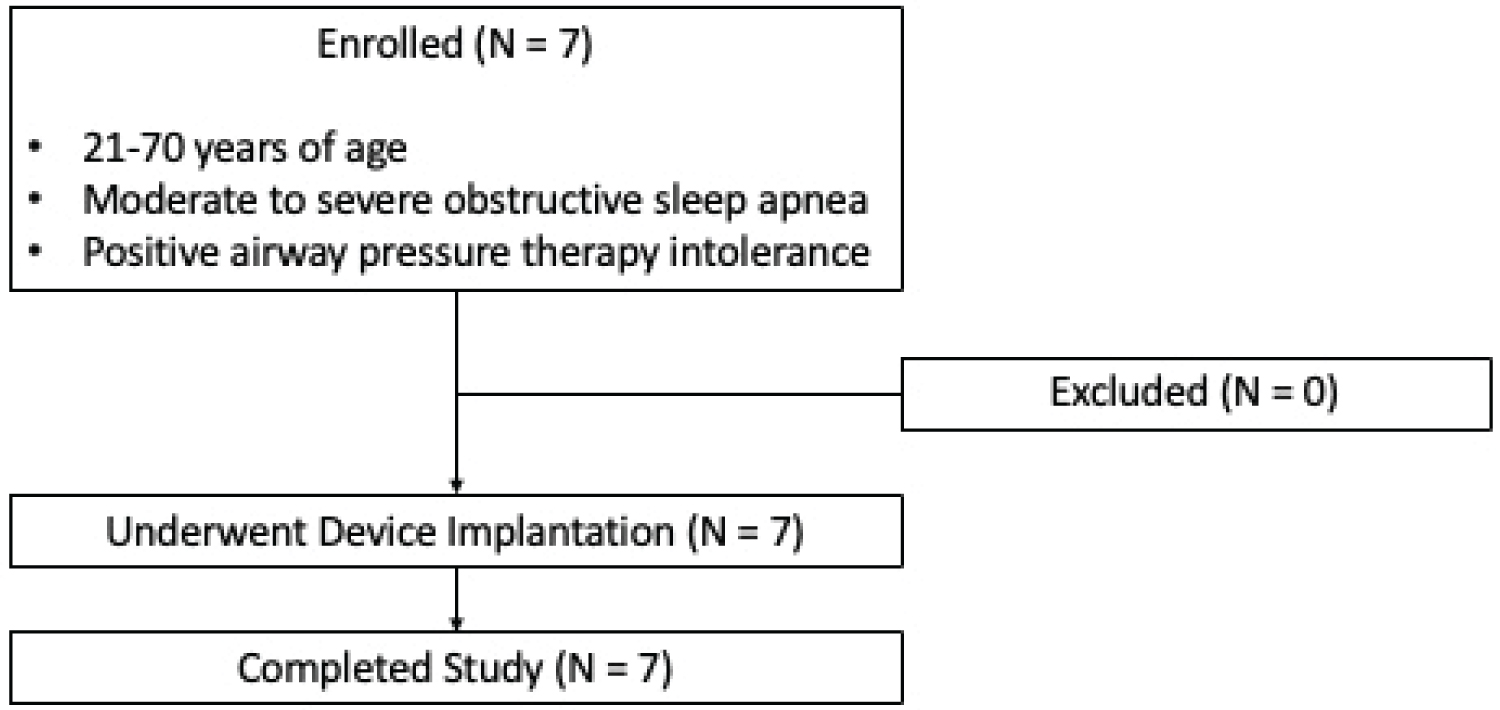 Figure 3: CONSORT flow diagram.
View Figure 3
Figure 3: CONSORT flow diagram.
View Figure 3
This first-in-human trial was designed as a Phase I non-randomized open label single-group assignment clinical trial to evaluate the safety and feasibility of the Magnap device for treatment of OSA [11]. The study began in July 2016 at a single academic medical center (University of California San Francisco) with planned enrollment of 10 participants (Table 1). This study was reviewed and approved by the FDA under an Investigational Device Exemption (G110121), as well as by the University of California San Francisco (UCSF) Institutional Review Board.
Table 1: Selection criteria for study participation. View Table 1
Primary outcomes were 1) Successful use of the Magnap device and 2) Safety of the Magnap device. Successful use was defined as successful implantation, full study period use without premature explantation, and nightly use of the external brace. Safety was determined by tracking the occurrence of all serious adverse events. Secondary outcomes evaluated the device’s ability to open the airway during sleep by comparing apnea-hypopnea indices (AHI) with and without Magnap device activation (i.e. with and without external brace use).
The implantation surgery was performed under general anesthesia by the same otolaryngologist at UCSF to minimize variation. A 3-4 cm transverse skin incision was made overlying the hyoid bone. A small subcutaneous pocket was created deep to the platysma and anterior to the hyoid bone. The implant was then secured to the anterior hyoid bone with two non-absorbable sutures using the holes on either side of the titanium implant. The overlying skin and soft tissues were then closed. Each participant was admitted overnight (23-hour stay) for monitoring of adverse events, followed by standard postoperative follow-up visit at one week post-hospital discharge. All participants wore either a dog tag or medical alert bracelet to avoid any MRI.
Post-implantation, participants were followed for 13 months (clinical trial endpoint) with four planned in-lab sleep studies at months one, four, seven, and 13. PSGs were interpreted - per standard criteria outlined by the American Academy of Sleep Medicine (AASM) - by the same UCSF pulmonologist board-certified in sleep medicine to minimize variation [12]. The AHI was defined as total number of apneas plus hypopneas per hour of sleep.
Participants underwent nightly use of the external neck brace during sleep. Monthly patient follow-up was conducted to evaluate for any adverse events, device adherence, and feasibility of nightly use.
On March 19, 2020, California issued a statewide stay-at-home order which led to the closure of sleep laboratories and diversion of resources. This delayed ongoing outcome monitoring for one patient (participant number six) due to inaccessibility to in-lab PSG. In addition, patient recruitment was halted from March 2020 to March 2021 due to COVID-related infection control measures, study candidate reluctance, inability to perform baseline in-lab PSGs, and cancellation of elective surgical procedures.
These extenuating circumstances were mitigated by utilizing a secure video conferencing platform for interval follow-up visits and adopting the FDA-approved AcuPebble SA100 (Acurable, London, United Kingdom) device for remote sleep apnea testing (Supply file 1). The AcuPebble SA100 device was chosen for HSAT due to its entirely virtual instruction, ease of use without cumbersome device components, and validated efficacy in detecting apnea and hypopnea events [13]. It is an external wireless wearable device which detects acoustic signals, translates them to disordered breathing events, and provides automated AHI scoring based on AASM diagnostic criteria [13]. Participants were virtually trained on HSAT use, which allowed for continued outcome monitoring for participant number six and continued outcome monitoring for participants who refused device explantation. After implementation of these study modifications, participants used HSAT at least monthly to closely monitor sleep outcomes, or more frequently if requested by the study participant or study staff to facilitate customized adjustments to the external brace. Total number of successful sleep studies per study participant was tracked both before and after HSAT implementation. Mean number of sleep studies per participant were calculated including in-lab PSGs and HSATs. AHI improvement was calculated as the difference between the baseline AHI (prior to device implantation) and the final/most recent study AHI with device use.
Descriptive statistical analysis was performed with categorical variables summarized as absolute values (n) and proportions (%) and continuous variables summarized as either medians with inter-quartile ranges (IQR) or means with standard deviations (SD). No formal hypothesis testing was performed in this interim report.
Seven participants were enrolled in the study from July 2016 to July 2022 and underwent successful implantation and completion of the study period without premature explantation of the device. All participants were able to use the external brace during sleep and there were no serious device-related adverse outcomes. One participant reported minor skin irritation with external brace use which resolved without intervention two months post-implantation. Baseline characteristics are outlined in Table 2.
Table 2: Baseline characteristics of study participants. View Table 2
After implementation of COVID-related modifications, 2 participants adopted HSAT for continuation of device monitoring during the study period and 3 participants for continued post-trial device monitoring. 100% of participants who adopted HSAT monitoring were able to appropriately use the HSAT system without in-person education. The average number of sleep studies performed per participant increased from 3.2 to 33 (Table 3). Post-implantation outcomes are outlined in Table 3. There were no adverse events associated with device implantation or explantation. Lifestyle-related factors led to external brace non-adherence for one participant, while a previously undiagnosed component of central sleep apnea limited efficacy in the second participant. Five participants refused explantation upon completion of the study period due to reported satisfaction with the Magnap device (Table 3). AHI improvement was observed in four participants at the end of the study period with a mean improvement of 14.8 ± 5.4 per hour (Table 3).
Table 3: Post-implantation outcomes of study participants. View Table 3
The pandemic caused delays and disruptions in ongoing research studies and clinical trials, leading to a halt in outcome monitoring and a delay in trial recruitment. This was due to redirection of healthcare resources, social distancing efforts, and fewer referrals – which may have ultimately led to study termination. To address this issue, we successfully adopted HSATs as a remote monitoring platform. Results demonstrated that: 1) All active trial participants were able to effectively transition to home-based OSA therapy monitoring; 2) Participant enrollment continued, and 3) Sleep-related outcomes were measured more frequently. While prior studies during the pandemic have described the use of HSATs, no prior studies have described the use of HSATs in monitoring novel OSA therapies [14].
During the pandemic, the primary benefit of using HSAT was to reduce in-person interaction [13]. All trial participants were able to use the HSAT device correctly without in-person training - which allowed for study completion or continued monitoring in those who had completed the study period but chose to continue use of the Magnap device. When compared to in-lab PSGs, HSATs also offered improved patient comfort [15,16], patient convenience [17], potential cost savings [18], and increased access to OSA testing [16,19,20]. Prior work comparing HSATs to in-lab PSGs has also shown that in-lab PSGs may be subject to confounding from the artificial sleep setting and potential environmental factors (i.e. “first night effect”), as well as their inability to detect nightly variation in sleep parameters [21-23].
We observed that the use of HSATs allowed for more frequent objective measurements to be obtained. The increased frequency of AHI measurements, in conjunction with subjective patient feedback, allowed for real-time tracking of device efficacy and improvement of the external brace design to optimize both patient comfort and objective sleep parameters. Monthly HSATs were well tolerated by study participants and study participants often requested an increased frequency of HSATs to monitor their objective metrics and to seek out external brace adjustments that may improve their metrics. Thus, the convenience of HSAT monitoring may have facilitated participant tolerance to an increased frequency of HSATs. More frequent HSATs also allowed for prompt notification of any device-related issues and this may play an important role in remote safety monitoring of novel OSA therapies.
Interim analysis of the ongoing first-in-human Phase I trial evaluating the Magnap device for the treatment of OSA suggests safety in device implantation, use, and explantation. There has been no device-related or peri-operative serious adverse events to-date. While all participants were able to successfully use the device by wearing the external brace during sleep, adherence was limited in one participant due to lifestyle-related factors such as alcohol use and frequent air travel. Completion of this trial and future studies will be aimed at identifying the optimal patient characteristics for efficacy. In addition, conclusions regarding the safety and feasibility of the Magnap device await final study completion. This study is continuing to recruit and enroll participants with future research needed to assess device efficacy and characterize patient-related factors that may optimize Magnap use.
This study has various limitations related to HSATs, including differences in physiologic parameters collected, possible underestimation of a participants “true” AHI, and variation in commercially available HSATs [9]. Type three HSATs measure at least two respiratory variables (e.g. effort, airflow), oxygen saturation, and a cardiac variable (e.g. heart rate). Prior validation studies have compared HSATs to gold-standard in-lab polysomnography with an OSA diagnostic accuracy ranging from 84-91% [12]. Thus, type three HSATs have been approved by the FDA and are recommended by the AASM as an alternative to in-lab polysomnography for ambulatory diagnosis of OSA in patients with a high pretest probability of moderate-severe OSA. As the AcuPebble SA100 was previously validated against gold-standard FDA-approved type three cardiorespiratory polygraphy using the AASM’s AHI-based diagnostic criteria with 95.33% accuracy, 96.84% specificity, and 92.73% sensitivity, this device was chosen as we transitioned to HSATs during the pandemic [13,24]. The limitations of the AcuPebble SA100 are the limited outcome metrics acquired by this HSAT device. While useful in obtaining accurate AHI data in a remote setting, the lack of air flow sensors to track airflow abnormalities, as well as the inability to track sleep stages, percentage of time spent in each sleep stage, and absolute oxygen saturation did not allow us to compare the breadth of objective outcome metrics that we had initially planned to. Thus, while HSATs may be a useful adjunct to in-lab PSGs for OSA treatment monitoring, especially in the setting of the COVID-19 pandemic which limited in-person contact, these monitoring limitations must be considered when incorporating HSATs during trial design.
In addition to the limitations intrinsic to HSATs, this interim analysis is limited by the small sample size, male predominance, and atypically low BMI which limits generalizability and does not allow for a direct comparison of objective metrics between outcomes obtained by in-lab PSGs and HSATs. Future study design directly comparing these two modalities in the monitoring of novel OSA therapies should include participant randomization and adequate power to validate the non-inferiority of HSAT monitoring. However, in the setting of social distancing during the COVID-19 pandemic, the adoption of HSAT monitoring provided a feasible adjunct to OSA monitoring during use of the novel Magnap device for OSA treatment.
While interim analysis of the first Phase I trial to evaluate the novel Magnap device for OSA treatment suggests safety, final analysis of the planned cohort is required. During the trial period, disruptions from the COVID-19 pandemic led to the successful adoption of HSATs as a remote adjunct for monitoring of sleep-related outcomes. However, further research is needed to determine the best use of HSATs in the clinical trial setting.
None.
All authors had full access to all of the data in the study and take responsibility for the integrity of the data and accuracy of the data analysis.
Study conception and design: WGL, LLE, JL, KH, JLC, DMC, MD, MRH; Data acquisition, analysis, or interpretation: WGL, LLE, JL, KH, JLC, DMC, MD, MRH; Drafting of the manuscript: WGL, LLE, JL, KH, JLC, DMC, MD, MRH; Critical revision of the manuscript for important intellectual content: WGL, LLE, JL, KH, JLC, DMC, MD, MRH; Final approval of this manuscript version to be published: WGL, LLE, JL, KH, JLC, DMC, MD, MRH; Statistical analysis: WGL, LLE, JL, KH; Administrative, technical, or material support: JL, KH, JLC, DMC, MD, MRH; Supervision: JLC, DMC, MD, MRH.
Institution where work was performed: University of California San Francisco.
All authors have evaluated and approved this version of the manuscript.
Co-authors, MRH, MD, JL, KH, participate with Magnap, Inc and are paid for their role. Senior author, MD, is the interim CEO of Magnap, Inc. Aforementioned involvement with Magnap, Inc is paid irrespective of study publication. The remaining authors have no financial or non-financial conflicts of interest to disclose.
This sponsor-funded clinical trial is funded by Magnap, Inc. The primary sponsor, Magnap, Inc., is responsible for the design and conduct of the study and assisted with data collection, manuscript preparation (including review and approval of the manuscript).
This device is currently under FDA-approved investigational use (IDE: #G130285).
Magnetic Apnea Prevention (MAGNAP) Device to Treat Obstructive Sleep Apnea: First-in-Human Study of Feasibility and Safety. ClinicalTrials.gov Identifier NCT02431507
( https://clinicaltrials.gov/ct2/show/NCT02431507 ).