Study objectives: In 2015 the existence of a "Glymphatic" system in the brain was proposed and further confirmed by subsequent studies. This system is supposed to drain brain waste metabolites particularly during sleep, when it has been shown to increase its activity by about 90%. This system may slow its activity with advancing years; furthermore, in patients with sleep disturbance or Obstructive Sleep Apnoea (OSA) it could be significantly reduced. This systematic review aims to estimate the association of sleep disturbances and OSA with the development of cognitive impairment or dementia.
Methods: We searched PubMed, EMBASE, and PsycINFO up to July 2021 for observational comparative studies. Patients with sleep disorders, including OSA, were considered. Mild and severe cognitive impairment or dementia was chosen as outcomes. Risk of bias was evaluated by validated checklists. Results were described narratively.
Results: Of 1794 studies identified by the search, 39 were included (14 longitudinal and 25 cross-sectional studies). Twelve longitudinal studies assessed the association between sleep disturbance and cognitive impairment, while five assessed the association between OSA and cognitive impairment. All studies except two, which assessed the impact of sleep disturbance, showed a positive association with cognitive impairment or dementia. Four out of five studies that assessed the impact of OSA also found a positive association with the incidence of cognitive impairment or dementia. Follow-up ranged from 1 to 17 years.
Conclusions: Patients affected by sleep disturbance and sleep apnoea may have an increased risk of developing cognitive impairment or dementia in the following years.
Cognitive impairment, Dementia, Sleep disturbance, Obstructive sleep apnoea
CNS: Central Nervous System; GS: Glymphatic System; apoE: Apolipoprotein E; CSF: Cerebrospinal Fluid; ISF: Interstizial Fluid; OSA: Obstructive Sleep Apnoea; AHI: Apnoea-Hypopnea Index; AD: Alzheimer Disease; MCI: Mild Cognitive Impairement; CI: Cognitive Impairement; MRI: Magnetic Resonance Imaging
Traditional anatomical and physiological view of the brain assumed that lymphatic vessels were absent in the brain and Central Nervous System; this in 2015 was challenged by evidence showing functional lymphatic vessels lining the cranial dural sinuses in rodents [1].
This nouveau concept based on scientific observation in animals, could lead to a profound impact on our understanding of inflammatory and degenerative central nervous system (CNS) diseases [2].
This so called para-vascular space was already recently known in a route for clearance of glucose, lactate and β-Amyloid [3]; more recently also as a pathway for the clearance of interstitial solutes. This has been confirmed by fluorescent markers that revealed how cerebrospinal fluid (CSF) enters the brain parenchyma along the para-arterial space and exit via a para-venous space [4].
“Glymphatic” System (GS) term derives from the dependence on glial cells and functional similarity to the lymphatic system.
The GS allows distribution of ApoE, the predominant apolipoprotein in CSF and major carrier of cholesterol essential to neuronal function, as long as other growth factors, neuromodulators, carrier proteins and nutrients [5], and drug delivery [6].
Iliff, et al. suggested that their findings of lymphatic vessels may represent the second step in the drainage of the interstitial fluid from the brain parenchyma into deep cervical lymph nodes after first been drained into the CSF through a glial “lymphatic” (glymphatic) para-vascular pathway [4].
In this theoretical model CSF and interstitial fluid (ISF) continuously interchange between them; from the subarachnoid space, CSF is driven into the perivascular space, the Virchow-Robin space, by a combination of arterial pulsatility, respiration, and CSF pressure gradients: thus, the loose fibrous matrix of the perivascular space can be viewed as a low-resistance highway for CSF influx.
An additional role for perivascular spaces, in addition to being a pathway for the influx of CSF, they are important sites for delivering energy substrate and regulating blood flow. In pathological conditions, such as multiple sclerosis [7] and stroke [8], the innate inflammatory response and the cascade leading to oedema formation are initiated in the perivascular spaces.
Clearance of brain waste metabolites by the Glymphatic System is enhanced during sleep: Sleep is essential for the restoring of a lot of physiologic functions, among them the activation of the GS, that is reduced by 90% in the awake state [9].
However, our knowledge of CNS lymphatic circulation is largely based on animal studies [9].
In humans, some diseases can cause sleep deficits. Among these, one of the most common is Obstructive Sleep Apnoea (OSA). OSA is characterized by upper airway collapse, leading to recurrent arousals and hypoxia [10]; these alterations cause insomnia, resulting in ineffective rest [11].
The number of awakenings, polysomnography, measurement of saturation, the apnoea-hypopnea index (AHI) and a series of vital parameters are among the diagnostic and prognostic criteria of this syndrome [12,13].
The AHI is a gravity disease index, based on the count of apnoea and hypopnea per sleep hour. An AHI between 5 and 15 is index of mild OSA; an AHI between 15 and 30 is index of moderate OSA; an AHI > 30 is index of serious OSA [13,14].
While it is commonly known that the OSA is associated with an increased risk of cardiovascular disease [13], less is known about the possible correlation with brain degenerative disease and this sleep disorder.
Some studies have looked for correlations between OSA and the development of pathologies on a degenerative basis of the brain, such as Alzheimer’s Disease [15-19].
The GS allows distribution of ApoE, the predominant apolipoprotein in CSF and major carrier of cholesterol essential to neuronal function, as long as other growth factors, neuromodulators, carrier proteins and nutrients [5], and drug delivery [6].
As a matter of importance also for the present proposal, GS participates also in β-Amyloid removal from the brain, a marker of Alzheimer Disease (AD); the process has been demonstrated to be linked to AQP4 channels, as in vivo experiment on mice showed [4]. This has been furtherly confirmed in mice, in the aging brain, where older mice showed a 40% reduction of β-Amyloid protein in parallel to reduction of AQP4 expression [5].
A part of Aging Brain in mice, other disease models showed changes in β-Amyloid clearance in the GS: reduction in sleep deprivation, depression and obstructive sleep apnoea [20], improved in association to exercise and omega-3 fatty acids.
Peng [21] hypothesised that the dysfunction of the para-vascular pathway can be used as a marker of AD.
Other products subjected to removal by the GS are metabolites and interstitial solutes, as lactate; lactate removal rate is different depending on a variety of sleep conditions, so enforcing the important role of sleep in allowing a correct functioning of the GS.
Also, Tau protein, implicated in progressive neurodegenerative diseases, and α-synuclein, involved in Parkinson Disease, are described to be cleared by the GS [22,23].
As hypothesized by Ju, et al. [20] a possible link could exist between OSA and deficiency of the Glymphatic System [20], mainly due to the reduced activity of the nocturnal waste cleaning that happens overnight during sleep.
In addition to OSA, there are other pathologies that cause difficulty in sleep, almost primitive insomnia [24] obesity [25], reduced physical activity [26] as it also happens to working conditions like night-shift workers.
The aim of this systematic review was to evaluate the strength of association of sleep disturbances and OSA with the development of cognitive impairment or dementia.
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [27]. The study protocol was registered on the International Prospective Register of Systematic Reviews (PROSPERO reference number CRD42021276173).
We searched PubMed, EMBASE, and PsycINFO from databases inception up to 6 July 2021. The literature search was performed using a combination of free text and Mesh terms related (“sleep disturbance” OR “insomnia” OR “sleep disordered breathing” OR “sleep apnoea” OR “obstructive sleep apnoea” OR “overweight” OR “obesity” OR “reduced physical activity” OR “frequent awakenings” OR “overnight shifts” OR “shift workers”) AND (“cognitive impairment” OR “cognitive decline” OR “cognition” OR “cognitive function” OR “dementia” OR “Alzheimer”). In addition, we screened the reference list of retrieved articles. Finally, we asked experts in the field for additional reports. No language or time restrictions were applied. The full search strategies for different bibliographic databases are presented in the Supplemental Material.
Participants: Adults (≥ 18 years) and elderly with obstructive sleep apnoea measured polysomnography and defined by the apnoea-hypopnea index (AHI) or clinical diagnosis by International Classification of Diseases, Ninth Revision (ICD-9) codes; sleep disturbance (insomnia or other disturbance of the quality or quantity of sleep as measured by validated scale or instrument (e.g., Pittsburgh Sleep Quality Index (PSQI), Epworth sleepiness scale (ESS), Actigraphy) or ICD-9, due to overweight or obesity, physical illnesses, reduced physical activity, frequent awakenings, overnight shifts, shift works.
Subjects with comorbid conditions known to be risk factor for further cognitive impairment were excluded: brain damage due to previous traumatic brain injury; repeated micro-traumatisms; neurological inherited syndromes such as autosomal disorders, autosomal dementia, hereditary extrapyramidal syndrome, and chorea syndrome; Parkinson disease; multiple sclerosis; epilepsy; chronic renal failure; diabetes type 2; hypertension; coagulation disorders; chronic health failure; chronic obstructive pulmonary disease; ischemic or haemorrhagic stroke.
Outcomes: mild cognitive impairment (MCI), severe cognitive impairment (e.g., Alzheimer’s, age-related dementia, or other form of dementia) as measured by validated cognitive tests (e.g., Mini-Mental State examination (MMSE), Trail Making Test (TMT), Digit Symbol Subtest (DSS), Word Fluency test (WF) or by clinical diagnosis by International Classification of Diseases, Ninth Revision (ICD-9) codes.
Types of studies: Observational quantitative studies such as prospective and retrospective controlled cohort studies, cross-sectional studies, case control studies.
Two authors (DN, SM) independently screened articles retrieved via the search strategy from the title and abstracts. Potentially relevant studies were acquired in full text and assessed for final inclusion independently by two authors. Any disagreement was discussed with a third author (AS). Two review authors (DN, SM) independently extracted data from the studies. We extracted the following information: number and characteristics of participants: mean age, % male, type of sleep disturbance, covariates adjusted for in the analysis (e.g., age, gender, ethnicity, education, alcohol consumption, antidepressant/anxiolytic consumption), country, types of outcomes and results.
Two authors (SM, MGL) independently rated methodological quality. The Newcastle Ottawa Scale-Cohort studies were used for prospective and retrospective cohort studies [28], and a modified version for cross-sectional studies [29]. Though not expected by the scales’ guidance, in order to achieve a picture of the overall quality of the included studies, we counted the number of the “good” answers (indicating that the criterion was met) over the total number of questions for each study, to compute an overall score for quality. Across checklists, studies were categorized as high-quality if they met ≥ 90% of criteria, medium- if ≥ 50% but < 90%, and low-quality if < 50%).
We planned to combine the adjusted estimates of the effect measures from the individual studies through meta-analysis where possible (comparability of exposure and outcomes between studies) with a random-effects model for all analyses, allowing for heterogeneity between studies. However, the retrieved studies were very heterogeneous for type of exposure assessed (e.g., insomnia, different types of sleep disturbance, Obstructive Sleep Apnoea, sleep-related movement disorders, daytime sleepiness, time in bed, etc.), type of outcomes (e.g., CI alone, dementia, combined CI and dementia, Alzheimer disease, length of follow up; finally, the statistical analysis methods used were very different, with some studies measuring the hazard ratio, some other the OR, some using pooled estimates of continuous measures.
Therefore, we described the results narratively grouping the studies for study design (longitudinal or cross-sectional) and for type of exposure: Sleep disturbance/insomnia or sleep apnoea.
The bibliographic search retrieved 1794 records after duplicates were removed. One hundred-twenty articles were judged as potentially relevant and acquired in full text. For two studies we were unable to retrieve the full text. Eighty-one articles were excluded because they did not meet the inclusion criteria, references of excluded studies and reasons for exclusion are described in the Supplemental Material. Thirty-nine studies were finally included (Figure 1). Fourteen were longitudinal studies, 13 retrospective or prospective cohort studies [30-42] and 1 case control study [43]; 25 were cross-sectional studies [44-68].
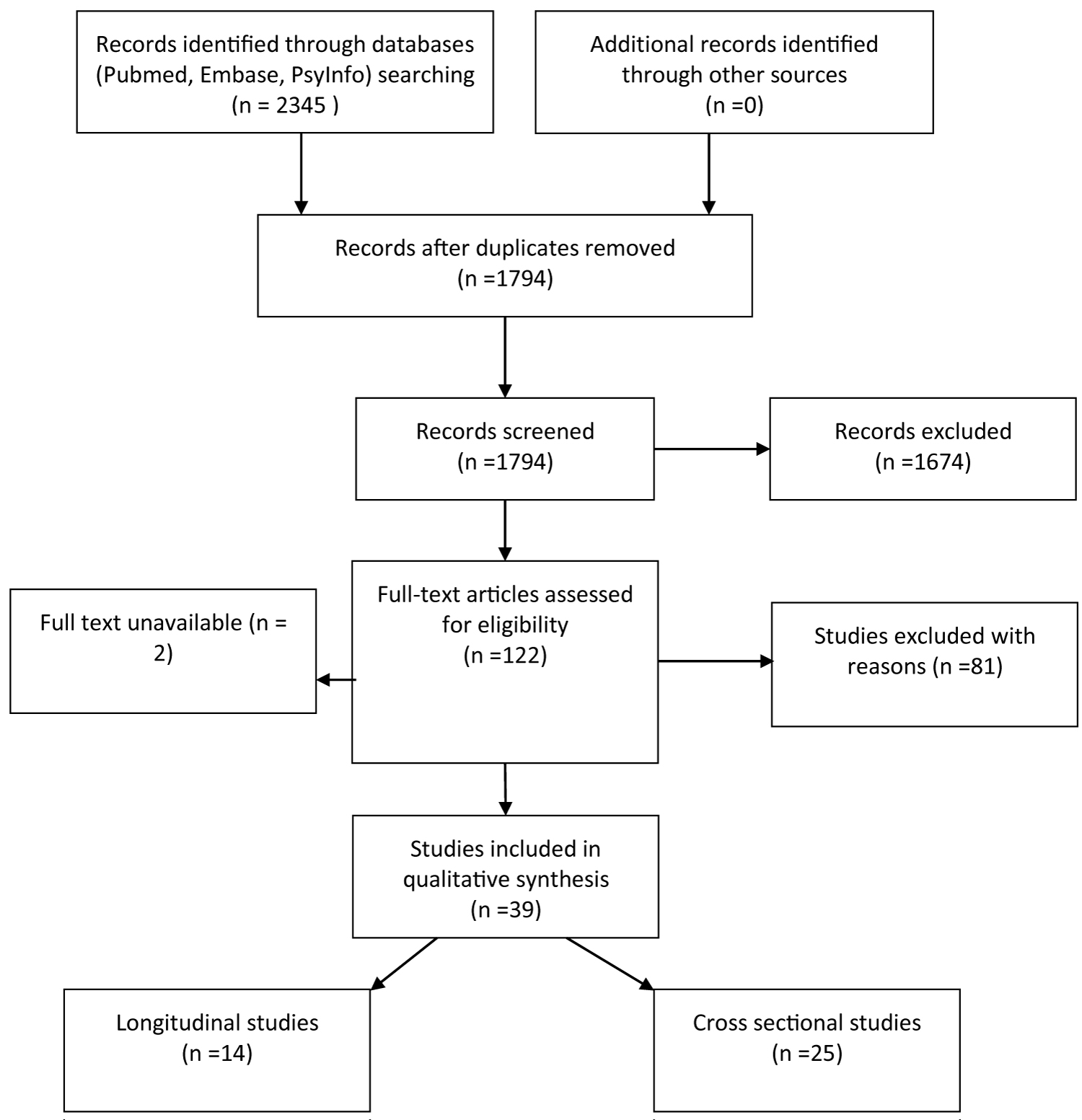 Figure 1: Flow Diagram.
View Figure 1
Figure 1: Flow Diagram.
View Figure 1
The longitudinal studies included a total of 598.969 participants; mean age ranged between 47 and 89 years across the studies, mean percentage of male ranged between 33.6% and 65.9%; three studies included men only [31,36,42], two included women only [35,41] and one study did not reported gender of participants [33]. Median Follow was 4.1 year (range 1 to 17 years). Four studies were conducted in US, four in Taiwan, two in UK and one each in Spain, Sweden and Canada. For a detailed description of the included studies see Table 1.
Table 1: Characteristics and results of longitudinal studies. View Table 1
Nine studies [30-32,34,37,38,40,42,43] were rated as high quality, and the remaining as medium quality. The most frequent flaws of the studies were a lack of description of the adequacy of follow up of cohorts or lost at follow up higher than 20% and the lack of information about blindness of outcome assessment (Supplementary Table e1 and Supplementary Table e2).
Table 2: Sleep disturbances and risk of cognitive impairment or dementia -longitudinal studies. View Table 2
The cross sectional studies included a total of 15900 participants; mean age ranged between 34 and 85 years across the studies; seven studies [47-49,52,59,62,68] enrolled only elderly participants (70 years and older), mean percentage of male ranged between 3% and 82%; three studies included men only [48,49,52], one study included women only [47]. Six studies were conducted in USA, four in China, two each in Brazil, France and South Korea and one each in Egypt, Japan, New Zealand, Spain, Turkey, Australia, Israel, Belgium and Malaysia (Supplementary Table e3).
Table 3: Sleep apnoea and risk of cognitive impairment or dementia. View Table 3
Eight studies (32%) were rated as high quality, seven (28%) as medium quality and ten (40%) as low quality. The most frequent flaws of the studies were small or very small sample not randomly selected from the population of interest, lack of information about blindness of outcome assessment and statistical analysis that did not adjust for confounding factors (Supplementary Table e4).
Sleep disturbance and incidence of Cognitive impairment or dementia: Twelve studies [30-39,42,43] assessed the effect of sleep disturbances, including insomnia, cognitive impairment or dementia. Sleep disturbance was assessed by objective measures (Actigraphy) only in one study [35], by subjective measures only (Karolinska Sleep Questionnaire, Wisconsin Sleep Questionnaire, Pittsburgh Sleep Quality Index (PSQI) Epworth sleepiness scale (ESS)) in four studies [32,33,36,39]. Two studies [30,31] used both objective and subjective measures. Four studies [34,37,38,42] used retrospective data collected from national databases and reported diagnoses of insomnia according to ICD-9-CM codes. One study [43] used the red code indicating insomnia in the database, or presence of the hypnotic medication in the prescribing history from the primary care dataset of the UK’s Clinical Practice Research Datalink. Cognitive decline was assessed with a variety of instruments in the included studies (Mini-Mental State Examination (MMSE), Trail Making Test (TMT, Trails-B), Delayed Word Recall Test (DWR), WAIS-R Digit Symbol Subtest (DSS), Word Fluency test (WF), Six-Item Screener (SIS; mental status); Brief- Verbal Learning Test (B-SEVLT; Cambridge Cognitive (CAMCOG), Informant Questionnaire on Cognitive Decline in the Elderly, California Verbal Learning Test). Dementia diagnosis was based on ICD-9 or 10 codes from national databases in five studies [32,34,37,38,42], on the red code indicating dementia in the database, or presence of anti-dementia medication in the prescribing history from the primary care dataset of the UK’s Clinical Practice Research Datalink in one study [43].
One study [30] that measured the impact of sleep disturbance on change from baseline in the score of several scales, found that longer sleep-onset latency was the only sleep disturbance measure associated with declines in global cognitive function, verbal learning, and verbal memory. No association was found between actigraphy-derived sleep duration and sleep continuity (eg, sleep fragmentation) with cognitive change (Table 1). Another study [33] that assessed the impact of sleep disturbance on cognitive impairment one to two years later measured by correlation coefficient between Epworth Sleepiness Scale (ESS) results and cognitive function found no association (Table 1).
All the remaining studies that measured the risk of mild CI or dementia by odds ratio (OR) or hazard ratio (HR) found that most of the types of sleep disturbance and insomnia significantly increased the risk of mild CI or dementia in the following years (Table 2).
Sleep apnoea and incidence of cognitive impairment or dementia: Five studies [33,36,40-42] assessed the effect of sleep apnoea or sleep disorders breathing on cognitive impairment or dementia. Sleep apnoea or disordered breathing were measured objectively through polysomnography in two studies [33,41], subjectively by questionnaires (Wisconsin Sleep Questionnaire) in one study [36]; two studies [40,42] used retrospective data collected from national databases and reported diagnoses of sleep apnoea according to ICD-9-CM codes. Cognitive impairment was assessed in one study [33] by Delayed Word Recall Test (DWR), WAIS-R Digit Symbol Subtest (DSS), Word Fluency test (WF)). Dementia diagnosis was based on ICD-9 codes from national databases in two studies [40,42], by the Clinical Dementia Rating in one study [36] and by clinical diagnosis according to DSM-IV in one study [41].
One study [33] that assessed the impact of sleep disordered breathing on cognitive impairment one to two years later measured by correlation coefficient between hypoxemia index and cognitive function found no association (Table 1).
The other four studies found that sleep apnoea significantly increased the risk of dementia 4.7 to 10 years later, although Elwood found significant result for vascular dementia only (Table 3).
Cross-sectional studies: Nine studies [44,46-48,58,59,62,65,66] assessed the association between sleep disturbance and cognitive performance or impairment. Sleep disturbance was assessed by subjective measures (such as the Pittsburgh Sleep Quality Index (PSQI) and the Epworth Sleepiness Scale (ESS) or by actigraphy). Three studies [51,53,54] assessed the association between Insomnia according to the ICD-10 codes and cognitive performance. Thirteen studies [45,49,50,52,55-57,60,61,63,64,67,68] assessed the association between sleep apnoea and cognitive impairment. Sleep apnoea was measured by polysomnography and determination of the AHI index.
Cognitive performance was assessed by a variety of scales and instrument, the most frequently used being the Mini-Mental State Examination (MMSE), the Montreal Cognitive Assessment (MoCA) the Trail Making B Test (Trails B), the Digit Vigilance Test (DVT), the Wechsler Scale, the Stroop test.
Results were mixed, with some studies showing an association between sleep disturbance or sleep apnoea and poor cognitive performance, while others did not. However, the studies were vey heterogeneous, for types of participants, sample’s representativeness and dimension, instrument used to assess cognitive performance, methodological quality and type of statistical analysis performed making any statistical or narrative pooling of the data very difficult and poorly informative. Results of individual studies are shown in Table e1 in the online appendix.
This systematic review aimed to evaluate the strength of association of sleep disturbances and sleep disordered breathing with the development of cognitive impairment or dementia. We included a total of fourteen longitudinal studies with 598.969 participants and 25 cross-sectional studies with a total of 15900 participants. We found a relevant number of longitudinal studies with a great number of participants and of high or medium methodological quality, which could allow to assess the existence of a possible causal relationship between sleep disturbance or sleep breathing disorders and the subsequent development of cognitive impairment; on the contrary, the evidence coming from cross sectional studies, that derived from very heterogeneous studies of medium or low quality, could allow only to assess the presence of an association but not a causal relationship; for this reason, we focussed our analysis on the results of the longitudinal studies only. Twelve longitudinal studies assessed the association of sleep disturbance and incidence of cognitive impairment or dementia. All but two studies found that most of the types of sleep disturbance and insomnia significantly increased the risk of mild CI or dementia in the following years. Five longitudinal studies assessed the association of sleep apnoea or sleep disordered breathing and CI or dementia. All but one studies found that sleep apnoea significantly increased the risk of dementia 4.7 to 10 years later.
The evidence of an association between sleep disturbance or sleep apnoea and the subsequent development of CI or dementia from longitudinal studies can be considered robust as 63% of the studies were of high quality and the remaining were of medium quality; all the studies recruited large samples truly representative of the population of interest and followed up for a median of four years; all studies adjusted the analyses for the most relevant confounders. Finally, nearly all the studies found consistent results.
In view of this analysis we could claim that sleep alterations and the development of dementia or cognitive impairment are linked. But what pathophysiological mechanism underlies this association?
The Glymphatic System theory may provide an explanation. During sleep, the Glymphatic System increases its clearance capacity, thus removing waste products of brain metabolism. It is well known that duration and quality of sleep are pathologically impaired in Obstructive Sleep Apnoea and sleep disturbance patients. Metabolites, therefore, tend to accumulate within the brain, eventually blocking the Glymphatic System. Taoka and Naganawa in 2020 introduced the concept of 'interstitial fluidopathy' of the Central Nervous System to denote this 'blockage' of the Glymphatic System. This pathological mechanism would appear to be implicated in the development of certain neurodegenerative diseases such as Alzheimer's disease and Parkinson's disease (Taoka 2020).
Furthermore, Roy, et al. in 2022 performed a magnetic resonance imaging study (MRI) measuring water molecules’ motion in the perivascular space direction by quantifying Diffusivity (Diffusion Tensor Imaging analyzed along the Perivascular Space, DTI-ALPS index). The study reported a decreased capacity for free water movement (proportional to Glymphatic System activity) in patients with sleep apnoea (Roy 2022).
Sleep and the Glymphatic System are therefore interrelated. The main studies in the literature have analyzed the accumulation of β-Amyloid in animal models.
β-Amyloid, as a waste product, is transported by the Glymphatic System [69]. Its slowing down may contribute to the accumulation of β-Amyloid in specific areas, such as the hippocampus and thalamus, typical of Alzheimer's disease [70,71].
Many forms of dementia and cognitive impairment, such as Alzheimer's disease, were included in our study. Many of the included patients may have developed early forms of this disease although stratification is complicated. Indeed, the diagnosis of Alzheimer's disease is autopsy-based and based on the identification of β-Amyloid plaques.
Another noteworthy fact is the speed at which dementia forms develop. In addition to the possibility of the presence of interstitial fluidopathy, multiple hypoxic episodes with acute stages must also be considered. In the brain, myelin appears to be among the structures most sensitive to hypoxic damage [72]. A principal characteristic of sleep apnoea is exposure to periods of sustained intermittent hypoxia [73]. Stroke is a cause of impairment of the Glymphatic System [74]; although patients with this condition were excluded from our study, the existence of ischaemic damage in patients with sleep apnoea must be considered. Elwood, et al. analyzed a cohort of 1225 men and found an association between sleep disorders and the development of vascular dementia [36]. In the study, the author only counted characteristics based on blood pressure and increased risk of stroke. These factors, which are known to lead to the development of dementia [75,76], must be taken into account. In addition, Kumar, et al. [77] observed a damage of both axons and their surrounding myelin, using Diffusion Tensor Imaging (DTI), in newly diagnosed treatment-naïve OSA subjects [77]; these pathological alterations were localised in encephalic areas critical for cardiovascular and respiratory regulation, like ventrolateral medulla and cerebellar cortex. Considering this, we could also hypothesize a self-powered pathophysiologic process where sleep reduction determines ischaemic harm that strengthens sleep dysregulation. Both Sleep reduction and ischaemic events could act synergistically on the reduction of Glymphatic System activity, thus leading to the early development of cognitive impairment.
This review has some limitations. Despite a very comprehensive bibliographic search on several databases, we can’t exclude that some relevant studies could have been missed. The second limitation is that we were unable to pool the data of longitudinal studies because of the heterogeneity among the studies in scales and instruments used to measure the outcomes, duration of follow up and confounding factor adjusted for in the meta-analyses.
Patients affected by insomnia, sleep disturbance and sleep apnoea have an increased risk of dementia. Instrumental examinations aimed at the description of sleep stages, serious controls and interventions aimed at restoring the physiological duration of rest could reduce the incidence of dementia in these subjects. In addition, many patients with insomnia and sleep disorders remain unknown to their doctors with an underestimation of the incidence of the phenomenon. The early identification of subjects affected by these sleep disorders would allow the initiation of therapeutic paths with possible improvement in the long-term quality of life of patients.
The analysis of data centred on the theory of the Glymphatic System would seem to highlight an essential role of sleep in the elimination of brain waste products. The forms of dementia determined by sleep deficiency could be caused by the accumulation of proteins and metabolites toxic to the central nervous system. Future studies should investigate this phenomenon, describing it both from a biomolecular and radiological point of view. A further field of research could be represented by the identification of an instrumental technique able to measure the CSF flow of the Glymphatic System: the demonstration of the effective reduction of this value, would represent strong evidence of its role in the pathophysiology of dementia.
Thakkar, et al. examined the current status of advanced imaging for Glymphatic System mapping, pinpointing methods such as MRI with gadolinium contrast (injected by intrathecal or intravenous way), DTI-MRI and 4D-flow MRI, SPECT/CT imaging, Ultrafast MR Encephalography, Fluorescence Microscopy and Macroscopic Imaging [78]. In addition to these techniques, a novel and promising imaging method for Glymphatic clearance evaluation was proposed in Örzsik’s work, where the diffusion of water molecules has been analyzed using a Kurtosis model (Diffusion Kurtosis Imaging and Diffusion Kurtosis Tensor Imaging), instead of the Gaussian one [79].
Finally, more research is needed to discriminate if there are isoforms of dementia: sleep disturbance could be a primitive cause of the development of a certain form, possibly typeable by the characteristic of accumulation proteins.
This work was supported by the AGING Project for the Department of Excellence at the Department of Translational Medicine (DIMET), Universit� del Piemonte Orientale, Novara, Italy.