Objective: Obstructive sleep apnea (OSA) is characterized by frequent episodes of upper airway collapse during sleep. The lingual tonsil, when hypertrophic, can contribute to airway obstruction. The purpose of this study was to establish the utility and safety of the carbon dioxide (CO2) laser for tonsillar reduction in the management of OSA.
Methods: Retrospective cohort study including patients who all underwent CO2 laser lingual tonsil reduction for OSA during a two-year period. The degree of preoperative and postoperative dysphagia was assessed using the Eating Assessment Tool (EAT-10) and the Reflux Symptom Index (RSI) and postoperative diet.
Results: 15 patients underwent CO2 laser lingual tonsil reduction from April 2019 through April 2021. The cohort was 53% male with an average age of 39.8 years and mean body mass index (BMI) of 28.3. The average preoperative Epworth sleepiness scale (ESS) was 10.1 with an average preoperative apnea hypopnea index (AHI) of 28.3 and a mean preoperative SpO2 nadir of 85.2%. On preoperative Mueller maneuver, the average degree of lingual tonsil hypertrophy was 2.6/4 and base of tongue collapse was 3.1/4. The mean preoperative EAT-10 was 3.6 while postoperative EAT-10 was 3.75. The average EAT-10 improved by 2.4 points postoperatively. The mean RSI preoperatively was 10.8 and 11 postoperatively. All patients were discharged home on a regular diet.
Conclusions: The results of this feasibility study indicate that the use of CO2 laser to be a safe and effective method of lingual tonsil reduction in patients with mild to moderate sleep apnea.
Brief Summary: The purpose of this study was to establish the utility and safety of the carbon dioxide (CO2) laser for tonsillar reduction in the management of OSA. The results of this feasibility study indicate that the use of CO2 laser to be a safe and effective method of lingual tonsil reduction in patients with mild to moderate sleep apnea with little negative impact on swallow function.
Lingual tonsil, Obstructive sleep apnea, CO 2 laser
OSA: Obstructive Sleep Apnea; CO 2 : Carbon Dioxide
Obstructive sleep apnea (OSA) is a chronic sleep disorder characterized by frequent episodes of partial or complete airway collapse during sleep. Subsequent reduction or cessation of ventilation results in impaired gas exchange and patient arousal from sleep. Although OSA has a multifactorial pathogenesis affecting a wide spectrum of the population, those of increased age, predominantly male sex, or of a high body max index (BMI) seem to be affected more commonly. The current prevalence of OSA in the adult population worldwide is estimated to be between 9% and 38% [1,2]. Elevated risks of myocardial infarction, nocturnal cardiac arrhythmias, stroke, resistant hypertension, depression, and motor vehicle crashes all related to OSA have been reported [3,4]. Being this disorder affects a vast number of individuals and has such negative health implications, it is crucial that providers safely and effectively address the condition. Diagnosis is established by polysomnography with the apnea-hypopnea index (AHI), average number of apneas and hypopneas per hour of sleep, used to determine disease severity [5].
Although obstruction can occur anywhere along the upper airway, a common cause is from the base of the tongue (BOT) collapsing during sleep. The lingual tonsil sits bilaterally atop the base of tongue musculature, between the circumvallate papillae and vallecula, with the median epiglottic ligament typically dividing it midline [6]. If these tonsils are hypertrophic, the pharyngeal lumen may be narrowed, increasing airway obstruction during sleep, along with disrupting normal swallow function by displacing the epiglottis posteriorly and inhibiting laryngeal elevation and epiglottic inversion [7].
Multiple management strategies to alleviate OSA currently exist ranging from medical to surgical interventions. The gold standard treatment for OSA is continuous positive airway pressure (CPAP) therapy, which has been shown to improve the physiology of OSA and additionally quality of life (QOL) in OSA patients [8,9]. However, the impact of CPAP therapy is limited by low adherence rates [10]. Some patients who do not tolerate CPAP are candidates for surgical intervention to reduce airway obstruction.
Surgical treatment options for OSA aim to create a more patent airway during sleep and can involve multiple different structures of the upper airway, such as the nose, soft palate, uvula, tongue, bony structure of the face (maxilla and mandible), and tonsillar tissue. The lingual tonsil has been reduced in many ways previously including cold steel, cautery and coblation. Each of these methods is plagued by the risks of postoperative hemorrhage, severe postoperative pain, postoperative dysphagia and dysgeusia. Historically, for this reason, the lingual tonsil has been a difficult area to address surgically in treating sleep apnea. This feasibility study is intended to demonstrate the utility of CO 2 laser for lingual tonsil reduction in adults with OSA while preserving normal swallow function.
This retrospective cohort study was approved by the Institutional Review Board at Stanford University. Physical paper charts and electronic medical records (EPIC) of patients were reviewed for all patients who underwent CO 2 laser reduction of the lingual tonsil for obstructive sleep apnea in a 2-year period from April 2019 through April 2021. Evaluated data included demographics (MRN, name, sex, age, date of birth, race), surgical information, clinical visits, medication information, disease status (diagnoses and severity of disease), and comorbidities. The inclusion criteria consisted of patients who had been previously diagnosed with OSA via polysomnography, non-adherent to CPAP therapy, and subsequently were referred for surgical management of their obstructive sleep apnea. Non-adherence was defined as patient non-compliance despite multiple attempts to use CPAP therapy for several days. All CO 2 laser lingual tonsil reduction were performed by the senior author (Dr. Dewan), while all other sleep surgeries were performed by a fellowship trained senior sleep surgery (Dr. Liu). Patients with a varying range of BMIs were included. Exclusion criteria for this study were as follows: Prior diagnosis of neuromuscular disorders, prior diagnosis of dysphagia, or rheumatologic disease, and any prior pharyngeal surgery.
Prior to surgery, subjective evaluation of swallow and swallow associated complaints were assessed with the Reflux Symptom Index (RSI) and the 10 item Eating Assessment Tool (EAT-10). The RSI is a nine-item questionnaire used to monitor symptoms and severity of laryngopharyngeal reflux; a score equal to or greater than 13 indicates clinically significant reflux disease. The EAT-10 is used to measure self-perception of dysphagia; a score of 3 or greater is considered significant, with higher values indicating more severe symptoms. The Epworth Sleepiness Scale (ESS) was used to estimate preoperative daytime sleepiness; a value of 11 or greater indicates excessive daytime sleepiness. Additionally, the degree of lingual tonsil hypertrophy, as well as the degree of base of tongue collapse was assessed using the Mueller maneuver. Preoperative AHI and SpO 2 nadir values were also considered.
During the preoperative evaluation all patients underwent a flexible videolaryngoscopic evaluation to assess the degree of lingual tonsil hypertrophy. At this time they also underwent a Fiberoptic Endoscopic Evaluation of Swallowing (FEES), administered by a Speech Language Pathologist. At this time data about the preoperative diet was collected using the functional oral intake scale (FOIS).
Each patient underwent CO 2 laser lingual tonsil reduction as a part of multilevel sleep surgery (Figure 1). The lingual tonsil was exposed using the Lindholm laryngoscope placed in suspension. The Lumenis (Yokneam, Israel) CO 2 laser when then used in a 5 mm circle pattern, on a setting of 6 watts Ultrapulse to shrink down, or attenuate the lingual tonsil tissue. As char accumulates the suction is used to remove char and expose deeper tonsil tissue for reduction. Any significant bleeding is cauterized with the Steiner endoscopic suction cautery.
 Figure 1: Surgical set-up for CO2 laser reduction of lingual tonsil.
View Figure 1
Figure 1: Surgical set-up for CO2 laser reduction of lingual tonsil.
View Figure 1
Postoperative bleeding requiring operation room intervention, along with diet at time of discharges was evaluated. To determine surgical effects on deglutition, the RSI and EAT-10 scales were re-assessed within a month postoperatively. Unfortunately, other postoperative objectives could not be assessed due to the severity of COVID-19 infection and subsequent lockdown. Additionally, follow-up appointments had to be virtual, rather than in-office visits, which limited the ability to perform elective evaluations and procedures as well as postoperative FEES as has been previously planned. The primary outcome measure used in this study was the average change in EAT-10 scoring. The mean EAT-10 scores of the study sample were calculated prior to and after sleep surgery, and a t-test was used to determine differences between the groups.
The cohort was composed of 15 patients with an average age of 39.8 years and a range of 16 to 74 years. Of those, 53% were male and 47% female. The average BMI was 28.2 kg/m 2 with a range of 18.3 to 47.5 kg/m 2 .
Prior to surgery, there was an average ESS of 10.1, an average AHI of 28.3, and an average SpO 2 nadir of 85.2%. On Mueller maneuver, the average degree of lingual tonsil hypertrophy was 2.6/4, and the average degree of base of tongue collapse was 3.1/4. The average RSI preoperative score was 10.8 and the average EAT-10 preoperative score was 3.6. At follow-up, patients were found to have a mean postoperative RSI score of 11 and a mean postoperative EAT-10 score of 3.75. The average change in EAT-10 score after surgery, improved by 2.4 points. At time of discharge assessment, no incidence of postoperative bleed or postoperative airway obstruction was identified, and all patients were discharged on a regular diet without modification (Figure 2).
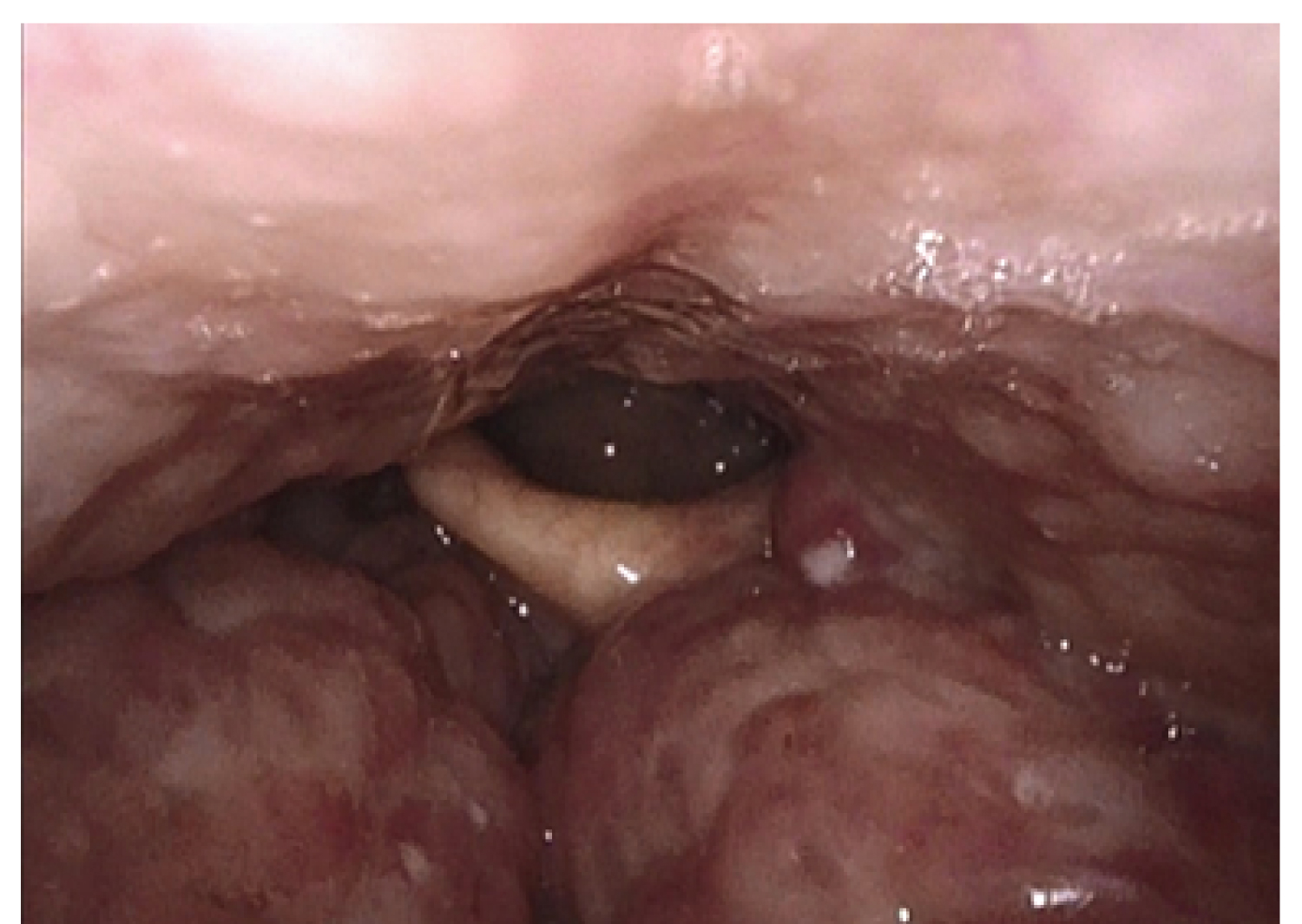 Figure 2a: a) Before base of tongue reduction with CO2 laser. The lateral channels on either side of the epiglottis are nearly completely obliterated, and the epiglottis is being pushed posteriorly such that the right aspect is touching the posterior pharyngeal wall. There is no room between the lingual tonsil and the epiglottis; b) Four weeks after base of tongue reduction with CO2 laser. There is reduced density of the tongue base with notably reduced bulk, and it is well healed and re-mucosalized. The epiglottic frenulum can now be visualized, and the laryngeal inlet is more open. This patient reported improved sleep and dysphagia, additionally, there was a decrease in the patient's ESS and EAT-10.
View Figure 2a
Figure 2a: a) Before base of tongue reduction with CO2 laser. The lateral channels on either side of the epiglottis are nearly completely obliterated, and the epiglottis is being pushed posteriorly such that the right aspect is touching the posterior pharyngeal wall. There is no room between the lingual tonsil and the epiglottis; b) Four weeks after base of tongue reduction with CO2 laser. There is reduced density of the tongue base with notably reduced bulk, and it is well healed and re-mucosalized. The epiglottic frenulum can now be visualized, and the laryngeal inlet is more open. This patient reported improved sleep and dysphagia, additionally, there was a decrease in the patient's ESS and EAT-10.
View Figure 2a
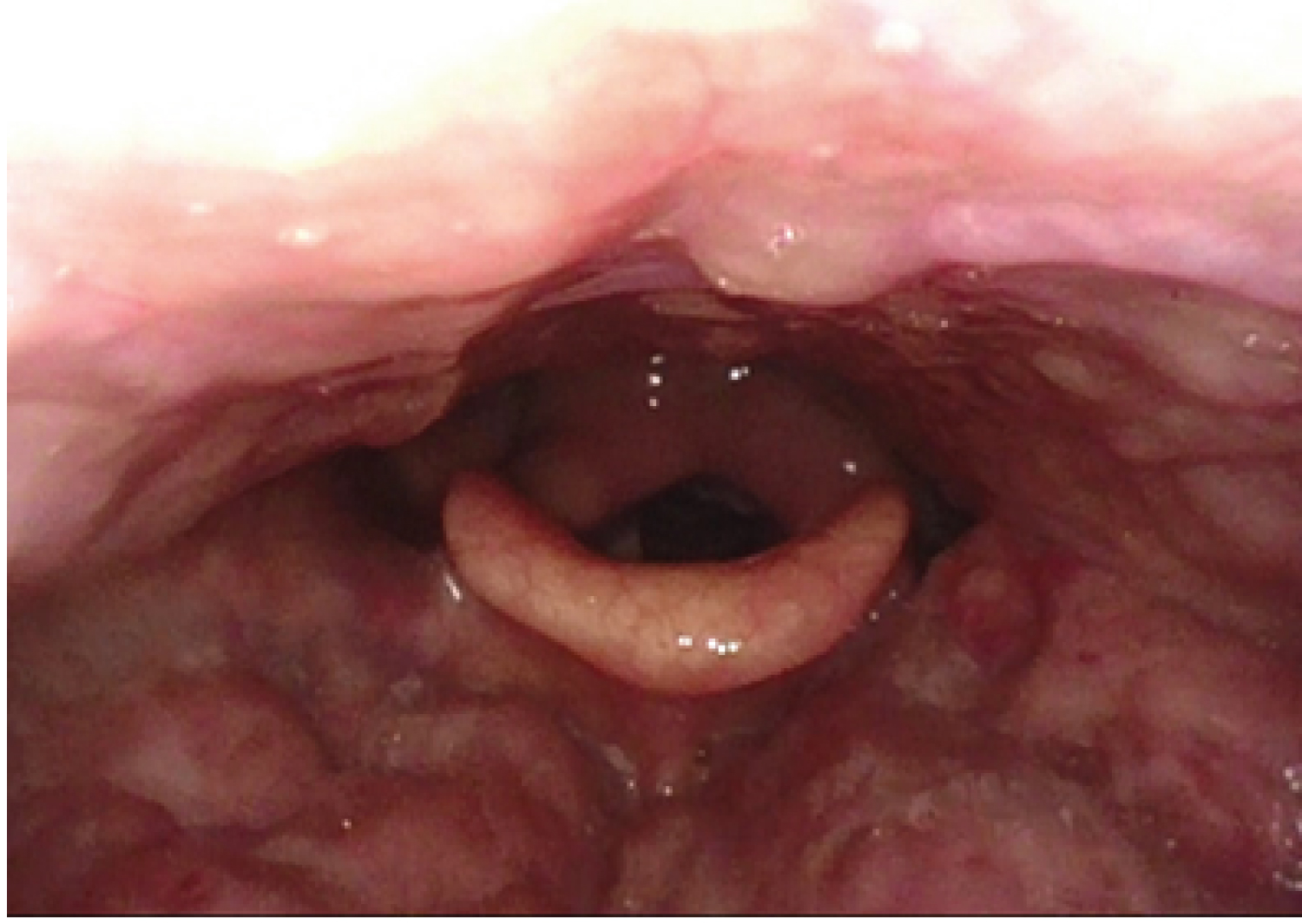 Figure 2b: b) Four weeks after base of tongue reduction with CO2 laser. There is reduced density of the tongue base with notably reduced bulk, and it is well healed and re-mucosalized. The epiglottic frenulum can now be visualized, and the laryngeal inlet is more open. This patient reported improved sleep and dysphagia, additionally, there was a decrease in the patient's ESS and EAT-10.
View Figure 2b
Figure 2b: b) Four weeks after base of tongue reduction with CO2 laser. There is reduced density of the tongue base with notably reduced bulk, and it is well healed and re-mucosalized. The epiglottic frenulum can now be visualized, and the laryngeal inlet is more open. This patient reported improved sleep and dysphagia, additionally, there was a decrease in the patient's ESS and EAT-10.
View Figure 2b
The hypertrophic lingual tonsil is particularly difficult to address for several reasons. Not only is it challenging to visualize, but it is also adherent to an area on the genioglossus muscle lacking aponeurosis. Consequently, differentiating tissue is difficult and nearby structures is vulnerable to damage. Manipulation of the BOT neurovascular bundle (lingual artery, lingual veins, and hypoglossal nerve) is sources of serious complications namely hemorrhage, pain, dysphagia, and dysgeusia. Thus, it is important to weigh the risks of various surgical approaches with the severity of disease and to pursue the safest intervention.
Surgical management of lingual tonsil hypertrophy was first described in 1984 by M Joseph, et al. Initial attempts for lingual tonsillectomy were performed by cold dissection with the use of a snare, ring punches, and St. Clair-Thompson forceps. Unfortunately, this procedure was complicated by a 250 mL blood loss and tracheostomy was required in the immediate postoperative period [6]. Malleable suction cautery has also been used for lingual tonsillectomy having the appeal of improved visualization, precise dissection, and efficient hemostasis. However, this technique is faulted for its increased risk of thermal injury to surrounding tissues, particularly when charred debris occludes the device. After an extensive literature review of electrocautery-associated injuries, Ritcher and willing found the most reported complication to be airway fires, although, commissure burns and primary mucosal injuries were also frequently documented [11]. Such adverse events can result in catastrophic cosmetic deformities or functional disabilities for patients.
Thus, surgeons have shifted towards the microdebrider technique. The microdebrider is an electromechanical shaving device with continuous suction at its aperture. Constant suction provides a relatively clear visual field, as blood is removed throughout the operation. However, it does not provide a source of hemostasis, requiring other devices for coagulation. This powered tool aspirates and cuts only the tissue that is vacuumed into the aperture, despite that it occurs within a fraction of a second leaving little room for error [12]. Although the literature does not support more frequent complication rates, it is generally accepted that microdebrider complications are more severe [13]. Potential for serious damage to underlying muscle or neurovascular bundle limits this technique [14].
Transoral robotic surgery (TORS) for BOT reduction, with the use of the Da Vinci Surgical Robot, was previously thought to be advantageous as the smaller operating space improves access. Enhanced visualization, better dexterity and precise dissection between the tonsillar tissue and muscle also provide an upper hand. Literature shows that this method successfully reduces AHI and symptoms of sleepiness in adults with OSA [15]. However, despite these advantages, there are considerable drawbacks. Up to 21.3% of patients have experienced minor complications. Of those complications, 7.2% was attributed to transient dysphagia thought to arise from post-operative pain. Furthermore, a study done by Parker, et al. found a negative impact on long term swallowing performance, with 32% of patients experiencing persistent swallow disturbance after an average of 27.4 months postoperatively [16]. Dysphagia, or difficulty swallowing, gravely affects patient quality of life. Ekberg, et al. reported more than 40% of individuals with swallow disorders experience panic attacks or anxiety during meals, and data shows these patients are more likely to be depressed [17,18]. In addition to associated morbidities, the cost of this surgery makes it a less preferable option.
Tonsillectomy performed by radiofrequency ablation (RFA) reduces tonsillar tissue by thermonecrosis. Tissues surrounding dual needle electrodes (bipolar RFA) are heated to the extent of thermal injury (65-100 °C) resulting in precise vascular contraction, thrombosis, ischemia, and inflammation [19]. Ultimately, the healing process leads to fibrosed tissue and decreased volume. The scar tissue is unable to relax appropriately and tongue collapse during sleep is reduced. Because local anesthesia is sufficient for this procedure, it conveniently allows for outpatient treatment, though multiple treatments may be required. Despite improving airway obstruction, scarring of the BOT can negatively impact swallow as the tongue loses ability to propel the bolus properly. Kato, et al. reported that RFA of the tongue base was associated with odynophagia in 10% of encounters, dysphagia in 17.9% of encounters, and globus sensation in 23.6% of encounters, and noted increased odds of postoperative globus sensation relative to other BOT interventions by fivefold [20]. Negative effects on long-term speech and swallow function have also been reported [21].
Coblation (cold ablation) of the lingual tonsil is accomplished with radiofrequency electrosurgical ablation at a controlled temperature of approximately 60 °C. These conditions are believed to reduce thermal damage to surrounding tissue, yet preserve coagulation capability, theoretically resulting in less postoperative pain and hemorrhage. However, there have been reports of up to 22.2% secondary hemorrhage with coblation tonsillectomy in adult patients [22]. Furthermore, when compared to traditional tonsillectomy, Bäck, et al. found that coblation tonsillectomy did not have any significant advantages and resulted in similar postoperative morbidity [23]. Other disadvantages, specifically, meticulous hemostasis necessary for endoscopic visualization and postoperative taste disturbances, have been documented [24].
Satisfactory results, both short-term and long-term, with CO 2 laser lingual tonsillectomy were first described by Krespi, et al. in 1989. With findings of decreased postoperative hemorrhage and pain, no incidence of postoperative airway obstruction, as well as no disturbances in taste nor incidence of immediate or long-term voice alteration, the authors concluded laser surgery to be effective and safe for lingual tonsil management [25].
The CO 2 laser has only one chromophore-water. Therefore, tonsillar tissue, which is relatively rich in water, readily absorbs the radiant energy produced and is efficiently attenuated [26]. Positive outcomes with CO 2 laser utilization are speculated to be a resultant of minimal energy transmission to nearby tissue, providing accurate and predictable tissue reduction. Furthermore, the laser seals lymphatic vessels and nerve endings, contributing to decreased postoperative pain and edema [25]. Decreased pain is also supported by the findings of Randive, et al. who demonstrated a significantly improved analgesic profile with laser tonsillectomies [27]. Moreover, Karaman, et al. reported advantages with CO 2 laser when compared to electrocautery in BOT surgery, including decreased operation time and intraoperative bleeding, quicker return to oral feeding, shorter inpatient duration, as well as better patient reported comfort and functional outcomes [28].
The experience described here with CO 2 laser lingual tonsil reduction in obstructive sleep apnea patients has also been encouraging. In this feasibility study, there was no incidence of postoperative hemorrhage or postoperative airway obstruction. At time of discharge, all patient diets remained free of modification. There were no significant changes in EAT-10 or RSI scores. Though the study was limited by a small sample size, the data suggests safety of this intervention and points toward the possibility of performing CO 2 laser lingual tonsil reduction with no significant adverse impact to the subjective swallow function. To determine the true efficacy of this procedure, a large, multi-center, double-blinded randomized control trial is suggested for further investigation and comparison.
The results of this feasibility study indicate that the use of CO 2 laser is a safe and effective method of lingual tonsil reduction in the patient with mild to moderate sleep apnea. Historically there has been major hesitation to address the lingual tonsil due to the perceived risk of postoperative dysphagia development. The data presented coupled with minimal to no significant changes in EAT-10 or RSI scores demonstrated that CO 2 laser reduction of lingual tonsil does not have a negative impact on subjective swallow function. Moreover, it can safely be done in conjunction with other procedures for OSA including septoplasty, inferior turbinate reduction, tonsillectomy, adenoidectomy and uvulopalatopharyngoplasty. While safety has been established, the true efficacy of this procedure and comparison to other methods of lingual tonsil reduction remains to be determined in larger future studies.
This work did was not supported by any funding.
This work was performed at Stanford University.
All of the above authors have seen and approved the manuscript.
The authors do not have any conflict of interest to declare.