We present a case of a patient with post traumatic stress disorder related nightmares with REM predominant obstructive sleep apnea (OSA) who was treated with nasal expiratory positive airway pressure (EPAP) device. EPAP therapy was successful in reducing his nightmares associated with dream enactment. This case illustrates EPAP therapy may be an effective alternative therapy for nightmares in certain individuals with REM predominate sleep apnea.
Nightmares, PTSD, Dream enactment, REM sleep without atonia, Case report
EPAP: Expiratory Positive Airway Pressure; OSA: Obstructive Sleep Apnea; PTSD: Post-Traumatic Stress Disorder; RBD: REM Sleep Behavioral Disorder; RSWA: REM Sleep without Atonia
Nightmares appear in 6-10% of the US population and prevalence is higher in veterans who have suffered combat-related trauma [1]. Secondary (co-morbid) nightmares can be triggered in obstructive sleep apnea (OSA), periodic limb movements, and insomnia, and with medications especially dopamine agonists [2]. Patients with chronic PTSD are at an increased risk for altered and higher levels of REM sleep without atonia [3]. The differential diagnosis also includes confusional arousals from non-REM sleep. In any event the management should focus on reversal of poor sleep and daytime alertness.
Despite a plethora of research into RBD and OSA as distinct disorders, there is little literature on the coexistence of RBD and OSA. One study reported a number of patients with OSA experiencing similar behaviors to those seen in RBD at the termination of apneic events, suggesting that OSA can sometimes mimic RBD [4]. These patients’ RBD-like symptoms were abolished once CPAP was commenced as treatment for their OSA [5]. However, many may fail to tolerate CPAP, as the overall adherence is roughly around 30-70%, so other alternative therapies are considered [6].
Currently, there are limited options for nightmares with dream enactment; prazosin is the only FDA approved medication for PTSD related nightmares. Occasionally, adverse effects and lack of efficacy preclude its usage. In addition, nightmare restructuring therapy may be too difficult for certain veterans as it may resurface their PTSD symptoms. Moreover, certain individuals do not receive nightmare restructuring therapy favorably as they are unable to write out their nightmares due to lack time and uncomfortability. Melatonin can treat nightmares with dream enactment buy may lead to vivid dreams, intensifying an individual’s nightmare. Although clonazepam can reduce dream enactment, it may lead to dissociation in PTSD patients. Certain individuals prefer nonpharmacological therapy.
We present a unique case were an EPAP device (Bongo therapy) which is FDA approved for mild to moderate sleep apnea reduced the frequency of a veterans PTSD related nightmares by lowering his respiratory distress index during REM sleep. This case provides a bridge to future studies to see if the Bongo Device is therapeutic for nightmares associated with dream enactment in other individuals also.
Bongo Rx is a novel treatment option in the category of expiratory positive airway pressure (EPAP) device. It is FDA-cleared treatment for mild to moderate obstructive sleep apnea. It is not battery operated and Bongo Rx acts by increasing expiratory resistance which in turn generates backflow pressure that forces the upper airway to open wider [7].
We encountered a patient with PTSD-related nightmares associated with dream enactment episodes, in which the diagnostic and treatment process suggested that non-PAP management of OSA could effectively treat the condition.
A 74-year-old veteran with chronic PTSD, diabetes type 2 and mild OSA with a history of both subjective and objective dream-enactment reported by the veteran and his spouse, respectively. The veteran reported lack of efficacy and tolerability (dry mouth) from prazosin 3 mg, and regarded psychotropics unfavorably. The veteran presented to sleep clinic for symptoms of snoring, witnessed apnea and excessive daytime sleepiness. The veteran was tested with a WATCHPAT study, which showed an overall AHI 4% of 12.1/hr, with 16.4/hr during REM stage. Patient was initially started on CPAP treatment but was unable to tolerate it. Subsequently, he received Bongo Rx therapy which successfully eliminated snoring and reduced his nightmare frequency from 25 to 30 episodes per month to less than 2 episodes monthly. Over a period of 2 years the veteran lost 40 pounds, which he attributed to dental procedures. When offered retesting independent of therapy (Bongo Device), the veteran refused- “if I do not use the bongo device my nightmares resurface, I end up screaming, thrashing and striking, I still want to use the bongo device.” Thus despite weight loss, the veteran and his wife reported consistent episodes of dream enactment when he did not use the Bongo Device. Without access to the bongo device, nightmares and dream enactment episodes resurfaced generally during the second half the night. He reported rare nightmare episodes in the context of the Bongo Device.
The veteran agreed to evaluate if the presence of sleep disordered breathing mattered, with one night in the context of Bongo Device, and one night independent of the Bongo Device, both nights tested negative for sleep disordered breathing, however in the context of the Bongo Device (Table 1) his REM AHI was 0, REM RDI was 0, overall AHI 0.7 (Table 1 and Figure 1).
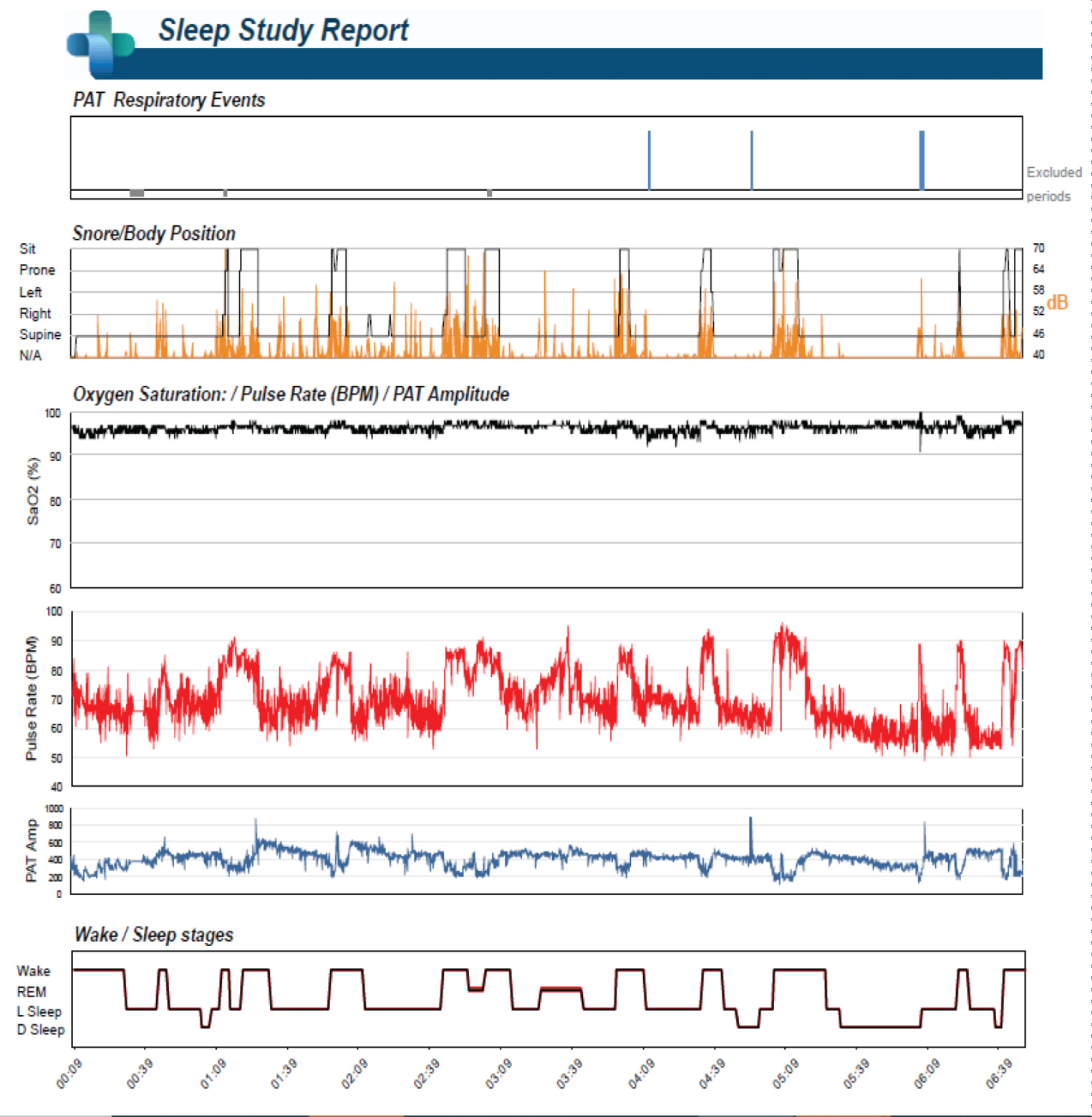 Figure 1: w/EPAP device.
View Figure 1
Figure 1: w/EPAP device.
View Figure 1
Table 1: Results w/EPAP device. View Table 1
Independent of Bongo therapy (Figure 2) his REM AHI was 3.7, REM RDI 3.7 overall AHI 2.2 (Figure 2) possibly indicating the Bongo Device is leading to less REM disruption or possibly less RSWA. Figure 2 (without Bongo Device) (Table 2).
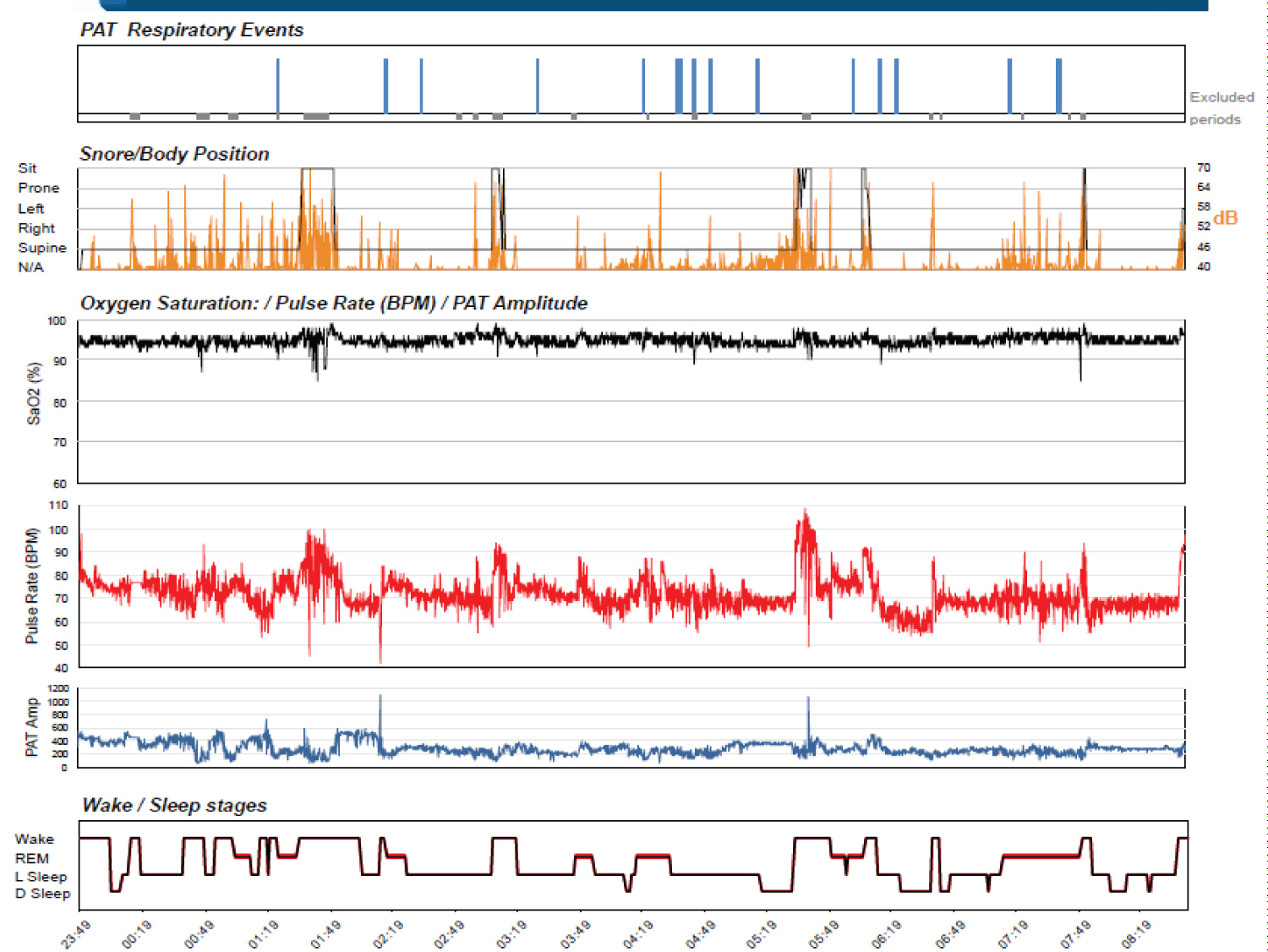 Figure 2: Without EPAP therapy.
View Figure 2
Figure 2: Without EPAP therapy.
View Figure 2
Table 2: Results w/o EPAP therapy. View Table 2
The veterans anxiety dreams associated with enactment are most likely attributed to his PTSD, given his nightmares predominately have a military theme, and because of the repetitive nature of these dreams, they were attributed to some unresolved conflicts or repressed wishes. Given his nightmares are associated with dream mentation with a recollected narrative, confusional arousals and night terrors are a low pretest probability.
It is plausible the veteran is experiencing PTSD with REM sleep without atonia (RSWA). Patients with chronic posttraumatic stress disorder (PTSD) are at increased risk for altered REM sleep without atonia [8].
Literature suggests individuals with chronic PTSD, either alone or with REM sleep behavior disorder (RBD), have significantly higher levels of RSWA compared to controls. In addition, higher levels of RSWA were found in the participants with both PTSD and RBD than in those with PTSD only [9]. Although no in laboratory PSG was completed, the veteran reports nightmares which occur during both the first and second half of the night, which are intermittently associated with dream mentation, with variable next day recall suggesting there may be an overlap of both conditions, there appears to similar phenotype between the two conditions, it has not determined if both conditions have the same pathophysiology as both PTSD and RBD may lead to degenerative conditions.
We hypothesize the Bongo Device is decreasing the intensity and frequency of the veterans nightmares associated with dream enactment by limiting REM sleep disruption and promoting REM homeostasis through attenuating respiratory events [10], consistent with the report by Iranzo, et al. who reported that severe OSA can imitate RBD symptoms, and showed these phenomena could be successfully treated by CPAP. This suggests true RBD could be exacerbated by OSA. However, it is reasonable to suggest that RBD symptom improvements may have been due to a reduction in pseudo-RBD behaviors associated with concomitant OSA.
We hypothesize that BongoRx showed similar pathophysiology in our presented patient which act to improve sleep fragmentation and decrease arousal from sleep and sleep disruption. Although this patient had overall mild sleep disordered breathing, his OSA severity during REM sleep is elevated and the repeat WATCHPAT study showed that REM AHI was significantly reduced after BongoRx therapy. BongoRx generates intraluminal pressure which stabilizes the collapsible segment of the upper airway, even if it would not have collapsed enough to be counted as an apnea or hypopnea (thus aiding pathologies such as sleep apnea and upper airway resistance syndrome). Additionally, the Bongo device may also reduce dream enactment behaviors in patients with concomitant OSA is by reducing sleep fragmentation. Our report is based on symptoms and we admit subjects are unable to distinguish which of their symptoms are caused by RBD and which symptoms are the results of OSA-related pseudo-RBD. More testing of the patient if consented would include spectral densities of REM EEG in RBD, as well as arousal non-atonic REM and video recordings.
Our report underscores the importance of recognizing parasomnia, creating a differential diagnosis, and treating disrupted REM sleep in veterans with PTSD nightmares. Future studies are needed to replicate these results. We postulate that at least in some patients, targeting and effectively treating predominately REM related OSA or REM related UARS in CPAP intolerant patients with alternatives like the Bongo Device may lead to secondary resolution of elevated PTSD related nightmares with or without dream enactment. From the veterans perspective, he reports the bongo device is an easy and effective way to address his nightmares, he notes being appreciate the VA has this therapy available as it is not covered by insurance.
None of the authors display any conflict of interest nor any financial support.