Objectives: Since the 1960s Methadone Maintenance Treatment (MMT) has led to a great improvement in health status and a decline in mortality among opioid-using patients. However, more awareness has been raised by professionals worldwide to the adverse effects and safety of MMT. This retrospective longitudinal cohort study aimed to investigate the effect of long-term use of methadone on the QTc interval in a population of MMT patients.
Methods: A total of 302 patients (male 82.1%), of whom at least one electrocardiogram (ECG) was registered between 2013 and 2020, were included. The primary outcome was the QTc interval over time. A maximum of five ECGs were collected per patient. Besides, methadone dose, co-morbidity, co-medication, substance use, and laboratory tests were documented.
Results: Over four years, only random, non-significant increases of the QTc interval were found. Univariate and multivariate linear regression analysis showed a significant effect of sex, methadone dosage, use of intermediate QTc prolonging medication, and increased AST (> 70 umol/L) on the QTc interval at baseline. The latter was only shown for the univariate model.
Conclusions: Our research showed a random increase of QTc interval over time within MMT population. Potential risks factors, such as methadone dosage, treatment duration, sex, medication with QTc prolonging effects, and CYP3A4 inhibitors do influence the QTc interval. Not all risk factors could be confirmed, because of limitations.
Addiction treatment, Methadone maintenance, QTc prolongation, Electrocardiogram
Since the 1960s methadone has been used for the treatment of opioid addiction in the Netherlands. The Methadone Maintenance Treatment (MMT) has led to a great improvement in health status and a decline in mortality among patients with opioid use disorder [1-3]. However, during the last two decades, more awareness has been raised by professionals worldwide to also the adverse effects and safety of MMT. This is due to the increase of methadone-associated overdose deaths [4-6]. Methadone has typically opioid-like adverse effects, including nausea, constipation, mild cognitive impairment, sexual dysfunction, and sedation [7,8]. Besides these adverse effects, more serious risks are associated with the use of methadone. These include potential pharmacokinetic interactions with other narcotics and/or medications, respiratory depression in overdosing, and cardiac arrhythmias [9]. The latter is due to the prolongation of the computed electrocardiographic QT (QTc) interval [7,8]. The QTc interval reflects the ventricular repolarisation of the heart, after ventricular depolarisation, corrected for heart rate. An abnormal QTc interval is considered as ≥ 450 milliseconds (ms) for males and ≥ 460 ms for females [10]. If the QTc interval exceeds 500 ms the risk of Torsade de Pointes (TdP) increases which can lead to ventricular fibrillation and can result in cardiac arrest or sudden death [7]. There are several risk factors associated with the prolongation of the QTc interval, such as female sex, hypomagnesemia, hypokalemia, structural heart disease, impaired liver function, genetic predisposition for prolonged QT syndrome, and the use of other drugs with QTc-prolonging properties (e.g. psychotropics, certain antibiotics). Because of the risks of TdP, a baseline electrocardiogram (ECG) before initiating methadone, with routine follow-up, is recommended for MMT patients [7,11]. QTc interval prolongation is reversible and lowering the doses or quitting methadone will mostly restore the QTc interval [12].
Methadone is well known for its QTc-prolonging properties. Studies report prevalences of QTc prolongation varying between 8.8% and 28.9% [13-16]. However, the increased risk of sudden cardiac death remains controversial [17,18]. Several studies suggest a dose-related increase in the QTc interval for methadone-treated patients [13,18-21]. For example, Anchersen, et al. showed that 4.6% of MMT patients had a QTc interval > 500 ms and a methadone dosage of ≥ 120 mg/day, which place them at risk of TdP [13]. Although, other studies did not find an association with a dose-related increased risk [22,23]. Most of these studies reflect the risk for QTc interval prolongation only over weeks or months. However, MMT patients may stay in the treatment for many years. As a result, the clinical relevance with regard to the dose-related risk of methadone and its effect on QTc interval in relation to the duration of MMT, remains unclear.
The primary aim of this retrospective longitudinal cohort study was to investigate the effect of long-term use of methadone on the QTc interval in a population of MMT patients. The primary outcome measure was the mean QTc interval during a four-year interval. The secondary aim was to confirm existing and identify potential new risk factors for prolonged QTc interval.
This is a retrospective longitudinal cohort study of all patients treated within MMT at one methadone maintenance treatment centre in the Netherlands (Mondriaan Heerlen), between 2013 and 2020. Electronic health records (EHR) were used to identify patients in MMT and collect their data between September 2020 and January 2021.
This study was exempted from the Human Subjects Act by the medical-ethical evaluation board of the Maastricht University Medical Centre+ and Maastricht University (METC 2019-1235) at 9-3-2020. Since this was a retrospective cohort study obtaining informed consent was not feasible. Given the large population which was difficult to reach, obtaining consent would require a disproportionate effort from the researcher. Collected data were pseudonymised. The study was conducted according to the principles of the World Medical Association Declaration of Helsinki.
Medical records of 321 patients receiving methadone in a MMT programme were available. ECGs were made every control visit according to the Dutch protocol of opioid maintenance treatment [11]. Patients who had at least one ECG available were included and the first ECG was defined as baseline. Patients without an ECG, no indication for methadone use, or no methadone use during the four-year period were excluded (n = 19) (Figure1). A total of 302 patients were selected for review. ECGs were made with Schiller type Cardiovit MS-2010 until 30 August 2020 and later with Cam-USB interface V2. All ECGs were reviewed by the medical doctor who provided feedback for each patient and arranged for appropriate referrals if the ECG was abnormal. QTc values were derived from the automated values reported on the ECGs. Data and patient characteristics were derived from EHRs and stored in a data extraction form in Excel 2012 (Microsoft Office 365).
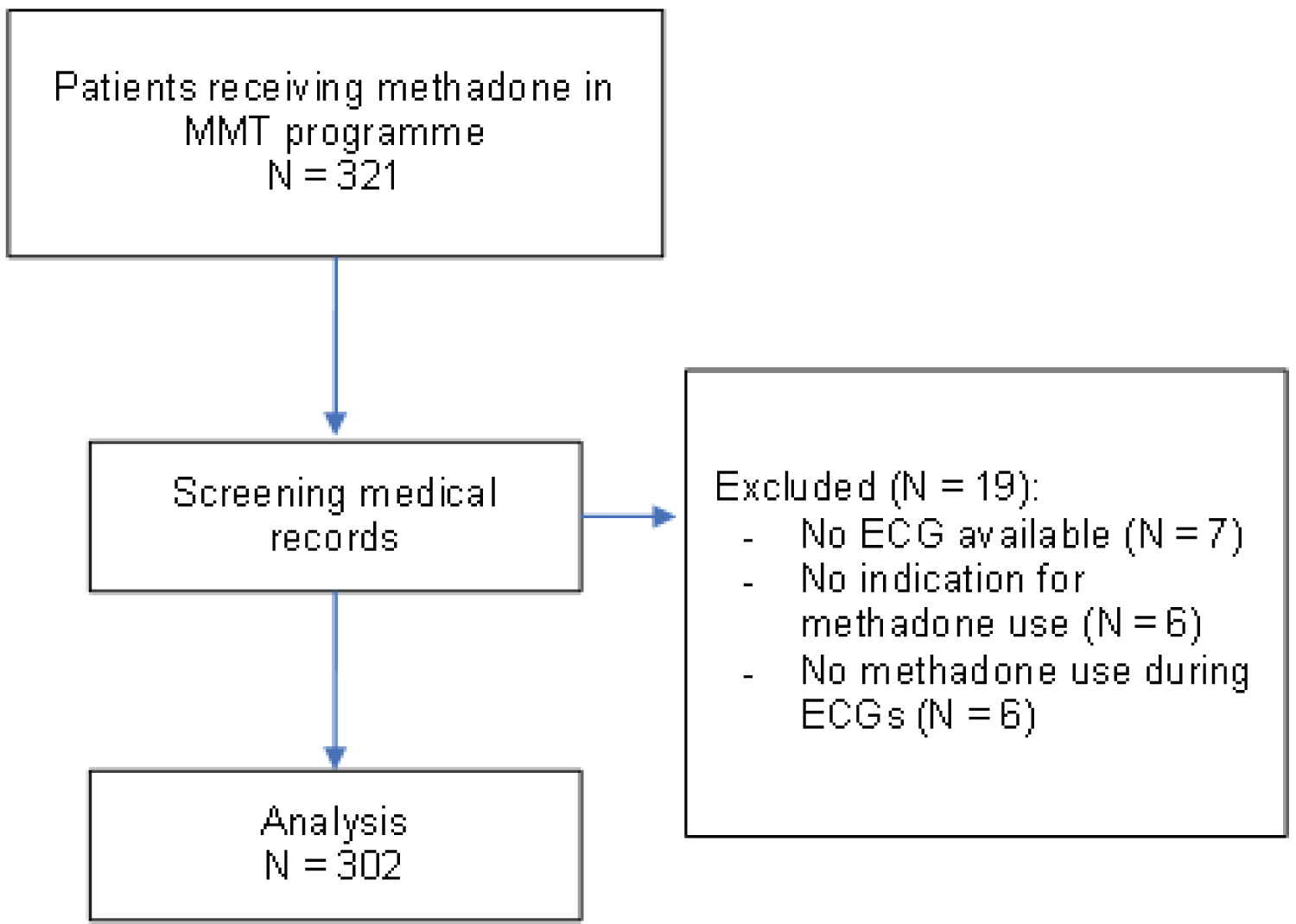 Figure 1: Flowchart of inclusion.
Figure 1: Flowchart of inclusion.
MMT: Methadone Maintenance Treatment; ECG: Electrocardiogram
View Figure 1
The primary outcome was the QTc interval at five time points (T0-T4). T0 was defined as 4 years prior to the last ECG. The first ECG within this period was defined as baseline (T0) and following annual ECGs were marked as T1, T2, T3 or T4.
All patient EHRs were reviewed for the following variables at baseline and subsequent time points; age, sex, body mass index (BMI), family history of diseases, chronic diseases, medication use, use of other narcotics, methadone dosage, and years of methadone use. When available, calcium, potassium, estimated glomerular filtration rate (e-GRF), serum creatinine levels, alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase, γ-glutamyl transferase (GGT), lactate dehydrogenase, total bilirubin, lipase, and blood glucose were also collected.
The use of other narcotics was specified in categories; daily, weekly, less than weekly, never, or unknown. The use of medication was specified in categories of CYP3A4 inductor or -inhibitor, and QTc prolonging medicine with high, intermediate, or low potential prolongation effects [9,24]. The medications that are known for these effects are represented in Supplemental File 1 and Supplemental File 2. Narcotics were specified as amphetamines, illegal use of benzodiazepines, cannabis, cocaine, alcohol, heroin, other opioids, and tobacco. Illicit drug use was based on voluntary reporting.
If patients left the MMT programme, subsequent data were marked as missing data. Also, if patients were suspected of extra use of (illegally gained) methadone prior to an ECG, the dosages of methadone at that time point were not reliable and marked as missing data.
Descriptive data are represented as mean ± standard deviation and categorical data as frequency (percentage). Missing data are reported, not imputed. At baseline methadone users and non-methadone users, patients new in MMT, were described and during follow-up time points, only patients using methadone were represented. For the primary outcome, the longitudinal effect of methadone on QTc interval, due to the high number of missing data at follow-up time points, was summarized using descriptive statistics. In addition, using General Linear Model repeated measures ANOVA, the annual QTc values from T0-T4 were compared using the data of the patients with QTc data available of all five time points. Furthermore, the QTc interval was divided into three categories; normal (< 450 ms for males, < 460 ms for females), prolonged (≥ 450 -< 500 ms for males, ≥ 460 -< 500 ms for females), and dangerously prolonged (≥ 500 ms for males and females) [10].
For the secondary aim, linear regression analyses were performed to determine whether any potential predictive factors influenced the QTc interval. The dependent factor was QTc interval in ms, and the independent factors were age, sex, BMI, family history of cardiac diseases, diabetes mellitus, methadone dosage, cocaine usage, laboratory results, and medication. Only complete cases were analysed and due to limited accessible data of laboratory values only GGT and AST were used.
A p -value < 0.05 was considered statistically significant. For the linear regression analyses assumptions of normal distribution were assessed using the Shapiro-Wilk test, multicollinearity using the Variance Inflation Factor (VIF) and Tolerance. Analyses were performed using SPSS version 25 (IBM, Armonk, New York, United States).
The demographic and medical characteristics at baseline for patients in MMT (n = 302) are represented in Table 1. The patients were mostly male (82%) with a mean age of 47.7 ± 9.3 years. Forty patients (15%) were new to the MMT programme and 61% of the patients were more than five years in MMT. The mean QTc interval was 427.5 ± 25.9 ms and only two patients had a dangerously prolonged QTc interval of ≥ 500 ms at baseline. The mean dosage of methadone was 53.7 ± 27.9 mg, but individual dosages were wide spread (1.3-180.0 mg/day). Fifty-one percent of the patients still used heroin, 36% cannabis and 90% smoked tobacco in addition to their maintenance treatment. Ten percent of the patients had a family history of cardiac diseases and 24% had cardiac diseases themselves. More than one-third of the population (37%) were diagnosed with hepatitis C and 36% suffered from pulmonary diseases most likely to be Chronic Obstructive Pulmonary Disease (COPD).
Table 1: Baseline demographic and medical characteristics. View Table 1
Of all 302 patients included, there were 41 patients with five ECGs, 75 with four ECGs, 78 with three ECGs, 67 with two ECGs and 41 with one ECG, respectively. QTc interval results are presented in Table 2, which provides an overview of the variance of QTc during four years (T0-T4) for all the patients in MMT. At T0 the mean QTc interval is represented for patients with (n = 262) or without (n = 40) the use of methadone and for T1-T4 only for patients using methadone at the time of the ECG. The mean methadone dosage fluctuates between 53.7 mg (T0) and 59.8 mg (T4). As shown in Table 2, the mean QTc interval of the patients using methadone over the five time points varies between 429.4 and 436.8 ms. Over the four years, the number of patients who had a prolonged QTc (≥ 450 ms for males, ≥ 460 ms for females) varies between 12.5% (T4) to 23.8% (T3) and varies between 0.6% (T2) to 2.4% (T3) with a QTc dangerously prolonged (> 500 ms for males and females).
Table 2: Mean QTc during four years for patients in MMT. View Table 2
Table 3 shows the mean QTc of MMT patients who had five ECGs (n = 36 (41 minus 5 because of ECG available however missing data on methadone use at T1-4)) made during the study period. The mean QTc interval at baseline was 425.3 ms and 431.8 ms after four years. During this four-year period, 5.6% to 19.4% of MMT patients had prolonged QTc (≥ 450 ms for males, ≥ 460 ms for females) and 0% to 2.8% of the patients had a dangerously prolonged QTc (> 500 ms for males and females). As displayed in Table 3, the QTc prolongation was not significant.
Table 3: Mean QTc during four years for patients in MMT with five ECGs available (n = 36). View Table 3
Univariate and multivariate linear regression analyses were used to determine potential predictors of the QTc interval, as shown in Table 4. Due to the amount of missing data, it was not possible to include the QTc data of the follow-up time points (T1-T4) and not all the potential predictors were added to the analysis. In this model, B means the increase or decrease of QTc interval in ms and the displayed constant (intercept) in the multivariate model is the baseline QTc time at T0. The univariate model in Table 4 (n = 274) presents an influence of sex ( p < 0.001), which indicates that the female sex is associated with a higher QTc interval of 14.12 ms. As expected, there was also an influence of methadone dosage ( p < 0.001) and the use of an intermediate QTc prolonging medicine ( p < 0.002) on the QTc interval at baseline. Finally, the effect of increased AST (> 70 umol/L) and treatment duration stands out in this table and strongly influences the QTc interval with 15.93 ms ( p 0.012) and 7.32 ms ( p < 0.001) respectively.
Table 4: Linear regression analysis for associated factors of QTc at baseline. View Table 4
The results of the multivariate model, also shown in Table 4, indicate a significant influence by sex ( p = 0.006), methadone dosage ( p < 0.001), the use of CYP3A4 inhibitor ( p = 0.049), and the use of an intermediate QTc prolonging medicine ( p = 0.005). In this model, the predictors of diabetes mellitus and laboratory outcome measures were not analyzed due to the lack of power (n = 122). The assumptions for linear regression analyses concerning normal distribution and multicollinearity were met (data not shown).
The primary aim of this retrospective longitudinal study was to determine the effect of methadone on QTc interval over a four-year period in MMT patients. Unfortunately, due to the missing data longitudinal analysis of QTc interval at different time points as planned was not possible. Our results showed only random/accidental increases in mean QTc interval over the four-year period. The data of the 36 patients with five ECGs available during follow-up also showed a random increase in mean QTc interval over time but no significance was established. The secondary aim of this study was to identify or confirm risk factors which potentially influence the QTc interval during this four-year period. Due to the missing data on the subsequent time points (T1-T4), the analyses are limited to the baseline data. The most important findings were a significant relationship between methadone dosage and QTc interval ( p < 0.001) and between duration of the treatment and QTc interval ( p < 0.001).
Our study could not contribute to the confirmation of several other studies that presented the relation between QTc interval and methadone over time [17,18,22,23,25,26]. Fareed, et al. showed that 41% to 56% of MMT patients had a QTc > 450 ms and < 500 ms and 4% to 10% of patients had at least one ECG with a QTc > 500 ms over a time interval of 5 years [25], a statistically significant prolongation from baseline ( p < 0.0001). Our study could not confirm these results and only show a random increase of the QTc interval over time. However, these negative results should be interpreted with caution due to the small sample size and lower mean dosage of methadone 54 mg (± 28).
Our study found that methadone dosage influences the QTc interval. The evidence presented by other studies [13,27] remains controversial on the effect of methadone dosages on the risk of QTc interval prolongation, as already stated in the introduction. It must be noted that Ehret, et al. also found a significant dose-effect of methadone on QTc interval prolongation, but QTc interval prolongation, as well as TdP, occurred with relatively low doses of methadone, 30 mg/day and 40 mg/day respectively [18]. Conversely, Fareed, et al. and Lin, et al. showed no association between methadone dosage and QTc interval [22,25]. Our results showed a significant relationship between the methadone dosage and QTc interval, however, it is questionable if this is clinically relevant. For example, if we use the regression coefficient to project QTc change per milligram of methadone, a patient with a baseline QTc of 415 ms would need to be on a methadone dose greater than 140 mg (men) or 136 mg (woman) daily to exceed the upper limits of QTc threshold; or greater than 340 mg (men) or 296 mg (woman) daily to exceed dangerously prolonged QTc. While the literature remains controversial, and our findings might not be clinically relevant, it must be interpreted with caution due to the possible life-threatening risks, small sample sizes and limited follow-up.
Besides methadone dosage, also other risk factors that might be associated with QTc prolonging effects were assessed. Important findings of the linear regression models were the significant influence of sex, the use of an intermediate QTc prolonging medicine, duration of treatment, and increased AST on the QTc interval at baseline. The multivariate model suggests that these variables have a similar effect as methadone, a prolongation of the QTc interval. This effect was not seen for the other potential predictors. Other studies also confirmed these potential risk factors [18,20-22,28].
Females are associated with a greater risk of developing drug-induced TdP compared with males, as shown by Makkar, et al. [28]. They performed a literature review and showed that women made up 70% of the 332 reported cases of cardiovascular-drug related TdP. The pathophysiological reason for this sex difference remains unclear. Our study confirms the influence of sex on the baseline QTc interval.
Besides sex, ageing may also influence QTc over time as presented by Rabkin, et al. [29]. They showed that prolonged QTc time is more present in older individuals within the non-addictive study population, especially among participants above 80-years-old. This study did not take this into account because of the lower mean age (47.7 years) within the population, but the increase of QTc while ageing should be considered.
Concurrent use of other medicines that are known to prolong the QTc interval may also increase the risk of QTc interval prolongation and therefore TdP. The main cause of QTc interval prolongation involves the human ether-a-go-go-related gene (hERG) and the subunit of the voltage-gated potassium channel (mostly found in the myocardium) for which it encodes. These channels cause the repolarization of the heart and abnormalities in these channels lead to prolonged action potentials that are expressed as long QT interval on the ECG [21]. Using other medicines that potentially block or intervene the hERG channels may increase the risk of individuals developing TdP or prolongation of QTc interval. Our study showed that medicines with intermediate potential prolonging effects had a significant influence on the QTc interval. Medicines with lower potential prolonging effect revealed not as risk factor. Unfortunately, the impact of medicines with high risk of prolongation of the QTc interval could not be assessed since they were not used within this MMT population. Prescribers of these medications should always be aware of this potential effect.
Methadone is metabolized by the liver through cytochrome P-450 (CYP) isoenzymes and is strongly protein bound. Medicines that interfere with pathways may increase the level of plasma methadone [20]. Ehret, et al. support these results and found an association between long QTc interval and CYP3A4 inhibitors and abnormal liver function [18]. We found a decreasing effect on the QTc of the CYP3A4 inhibitor. We have no explanation for this. A CYP3A4 inhibitor would increase methadone plasma levels by decreasing methadone metabolism. Perhaps low patients numbers or comorbidities may play a role.
Our study, possibly as a result of missing data, could not confirm the influence of other variables, such as cardiac diseases, hypokalemia, use of cocaine, and diabetes on the QTc interval as confirmed in other studies [18,21,22]. Although we could not confirm all potential risk factors, clinicians still need to be aware of them and advise the patient on potential risks.
The study had some limitations, including a retrospective design and many missing data. Retrospective cohort studies cannot demonstrate causality, therefore limiting the generalizability of the findings. Furthermore, it does not allow us to assess the change in QTc interval in a strictly pre- versus post methadone matter. The missing values led to information bias regarding relevant factors on QTc interval, such as some laboratory results. Additionally, the missing data could not be imputed because for some variables the number of imputed data would outweigh the number of original data. The use of two types of ECG devices could also influence the collection of QTc interval, however they were regularly calibrated. Another limitation of the study is the adherence of the patient group. This led to the fact that follow-up did not occur yearly, and routinely scheduled appointments had to be rearranged. As a result, only 36 patients had all five ECGs made and longitudinal multivariable analysis, including all potential predictors, was not possible. The data on other illicit drug use relied on voluntary reporting and not urine drug screening tests, which makes it less reliable.
On the other hand, to our knowledge this is the only study with a larger sample size that followed the QTc interval over an extended period (four-year interval). The population that is investigated and included is representative of the population within MMT programs.
MMT is the most effective treatment for patients with opioid use disorder. The Dutch protocol of opioid maintenance treatment recommends an ECG before the start of the treatment and one month after. The ECG needs to be repeated when the stable methadone dosage is achieved, with dosage adjustments above 100 mg of methadone, or when the patient has unexplained seizure or syncope [11]. This study supports the Dutch protocol as there was no prolongation of QTc interval shown over the years and no clinically relevant dose-dependent increase of QTc was found. However, the quantity of influence of potential risk factors on QTc interval remains unclear, and our evidence is limited due to information bias. Therefore, potential risk factors need to be continually evaluated by clinicians and we would recommend maintaining the current recommendation of regular ECGs if risk factors are present within a patient. To improve patient information about the risks of methadone on arrhythmias and TdP more data need to be established.
Implication for further research. A longitudinal multi-centre study assessing QTc interval and associated factors is needed to establish the potential risk of methadone in MMT and to assess additional potential risk factors such as age, associated with methadone use.
Our longitudinal research showed a random increase of QTc interval over time within MMT population, which supports the Dutch protocol of MMT. Potential risks factors, such as methadone dosage, treatment duration, sex, medication with QTc prolonging effects, and CYP3A4 inhibitors do influence the QTc interval. A prospective longitudinal multi-centre study assessing QTc interval and associated factors is needed to establish the potential risk of methadone in MMT.
Local funding only.
None.