In Sudan, obesity is increasing at an alarming rate especially in urban areas, becoming a social and medical concern. In pregnancy, overweight is associated with high risk of maternal death and many significant complications. Varied research and papers have also reported an increased risk of abnormality in offspring of obese and overweight pregnant woman. At the same time, carrying out an ultrasound examination on obese pregnant woman is a difficult task, due to the impaired acoustic window. This study investigates the rural-urban differences in risk for birth defects rates and the associated risk factors in the Northern State - Sudan.
A sample of 700 women, were examined by using ultrasound equipment and all cases also subjected to clinical check before and after ultrasound examination. Analysis of body mass index (BMI), diet, and physical activity was studied. Body mass index (BMI) was calculated using measured height and weight, and individuals with BMI ≥ 30 kg/m2 were categorized as obese. Multiple logistic regression models were used to examine urban-rural differences after adjusting for sociodemographic, health, dietary, and lifestyle factors.
Weight, BMI, Percentage of Body fat, Waist Circumference and Waist: Hip Ratio (WHR) was significantly higher (p, 0.001) in Urban women as compare to Rural women. Compared to urban women and rural women reported the malformation categories among birth of urban women were higher than that among birth of rural women (95% confidence interval: 1.6, 1.2). Some tactile variables were not observed prior to examination and observed in most of the cases after examination. Technical and medical observations were recorded and analyzed.
The higher prevalence of overweight and obesity was found in Urban women as compared to Rural women. Malformation categories among birth of urban women were higher than that among birth of rural women (95% confidence interval: 1.6, 1.2).
Urban and rural women, Overweight/Obesity, Body fat percentage, BMI, Sudan
Obesity and Overweight are defined as excessive fat piling up that may impair health [1]. According to guidelines published in 1990 by the Institute of Medicine (IOM) and acknowledged later by the World Health Organization, a woman is defined as obese if her body mass index (BMI and calculated using the formula weight/height2) is in the range of 30.0-34.9 kg/m2 and morbidly obese if her BMI is ≥ 35.0 kg/m2 [2]. The National Institute for Health and Clinical Excellence has further sub-categorized obesity into Classes I, II and III according to the BMI range (30.0-34.9, 35.0-39.9 and ≥ 40.0 kg/m2, respectively [3]. Zargar AH, et al. (2004) announced that Obesity is a rising issue even in developing regions and is more common in women and in urban population [4]. Shah Ebrahim, et al. (2010) studied that Emigration into urban areas is related with increases in obesity [5]. Environmental and behavioral changes brought about by economic development, modernization and urbanization have been linked to the rise in global obesity [6]. Overweight and obesity are strong risk factors for birth defects and other chronic medical conditions [7-9]. The Body Mass Index (BMI), is the simple method of measure of overweight and obesity [10]. The prevalence of overweight and obesity has risen up in Sudan over the years [11] and is more common in the capital city, Khartoum where urbanization is highest [11-14]. Sudan has 20 administrative regions. The Northern State is the third largest with rapid urbanization. In Sudan, there is little available data on the prevalence of malformation categories risk factors, birth defects and its variations across compared populations. The current study therefore sought to describe the differences in prevalence of obesity and malformation categories risk factors in Sudan drawn from urban and rural settlements.
This study was conducted in two locations, Dongola and Abri, both located in the Northern State - Sudan, from January to July 2017. Dongola was classified as urban and Abri was classified as rural, based on population, settlement, location and way of life of the people. Dongola is third amongst the largest metropolitan areas of Sudan. It is the commercial, industrial and cultural capital of the Northern State. Abri is a village with a clustered human settlement, located in the Northern State.
The study was carried out as clinical experimental study in the field of allied medical science inclusive as ultrasound imaging. The study was applied among overweight pregnant women, the samples subjected for study was 700, consisting of 350 urban and 350 rural settlers were recruited via simple random sampling technique. Waist Hip Ratio (WHR) was calculated through following equations, BMI = Weight (Kg.)/(Height in cm)2, WHR = Waist Circumference in cm/Hip Circumference in cm. Body Density was calculated using 7 site formula for women and Body Density was converted into Percentage of Body Fat by using Siri's Equation where percent body fat = 100 [ (4.94/Body Density) - 4.50] [15]. Data was analyzed and statistical significance was considered at 95% Confidence Interval.
The study adopted three conditions for the selection of samples:
a. Overweight and obese for pregnant women.
b. Immaculate record from hereditary diseases.
c. Immaculate record from congenital anomalies in previous fetuses.
To achieve these objectives, the research was carried out at Obstetrics and Gynecology Clinic with the supervisor of specialist Obstetrics and Gynecology. Samples were subjected to clinical and technical survey. Later, the medical and technical survey will be reveal in Tables below. To find the pressure change, reflected and transmitted power through uterus and abdominal fats (lipid) the following numerical impedance values were used Z1 = 1.38 × 10-5 rayl, Acoustic impedance for fat Z2 = 1.6 × 10-5 rayl, Acoustic impedance for soft tissue [16].
The samples subjected for survey was 700, sample were selected according to the following equation:
[17]
N is the population size (total number of pregnant women); e = 0.05: the level of precision when this formula applied.
population size = 4000
50 cases withdrawal from the study, means remains 350
population size = 3600
10 cases withdrawal from the study, means remains 350
Data analysis was performed using SPSS version 20. To investigate the birth defects affecting factors, logistic regression model was used to measure the crude odds ratio (OR) of birth defects occurrence for each of the independent variables. Multiple Logistic Regression (MLR) by backwards method was used to control the confounders; the independent variables with P value < 0.2 in the univariate analysis were entered in the MLR model. The results are expressed as OR with 95% confidence interval (CI). Significance level was adjusted as < 0.05.
During selection of samples from the study community, the researcher did not find among the pregnant women at that time:
1. Pregnant women - BMI 18.5 - 25 [Normal (healthy weight)]
2. Pregnant women - BMI 16 - 18.5 [Underweight]
3. Pregnant women - BMI 15 - 16 [Severely underweight]
Author justify this methodology choice for this selection of cases, according to the above reasons, also, the researcher's view; these classes that do not exist in the study negatively effect on the results.
The ultrasound examination for overweight pregnant women was done by using the ultrasound system with the following specification the model of ultrasound system used for the following survey was CX50 Women's Health (PHILIPS) as shown in Figure 1 from operation manual.
 Figure 1: Ultrasound system (PHILIPS). Source: PHILIPS CO.
View Figure 1
Figure 1: Ultrasound system (PHILIPS). Source: PHILIPS CO.
View Figure 1
Overweight is defined as a BMI of 25 or more, thus it includes pre-obesity defined as a BMI between 25 and 30 [18] and obesity as defined by a BMI of 30 or more [19]. Table 1 refer to the ultrasound examination was conducted for the first time in the eighth week of pregnancy to estimate the range of time that has passed since pregnancy, also examination was conducted in the 20th week of pregnancy to check the abnormalities and third examination was conducted in the 30 week of pregnancy to check growth.
Table 1: Ultrasound examination information. View Table 1
Table 2.
Table 2: Risk related to obesity in pregnancy. View Table 2
During the study period a total of 700 live born singleton infants were included in the group. Congenital heart defects were the most common malformation subtype (38.7%) followed by malformations of the diaphragmatic hernia (37.4%), limb reduction defects (12.7%), Hypospadia (6.9%), anorectal atresia (4.3%, Table 3). These findings are in good agreement with previously studies (see Table 4 in discussion).
Table 3: Association of maternal prepregnant body mass index with selected birth defects. View Table 3
Table 4: Epidemiological studies demonstrating an increased risk of congenital anomalies in the offspring of obese/overweight women (Obesity defined as BMI > 29.9 kg/m2 and overweight as BMI = 25.0-29.9 kg/m2). View Table 4
Table 3 shows the frequency of malformation categories findings for this study by clinical survey and after increased birth delivery. Also, metabolically healthy obese (MHO) and metabolically healthy overweight (MHOW) are studied to determine the progress rates phenotype to type 2 diabetes (T2D), and the results of this was found that the obesity was a risk factor for T2D. The metabolically health status as shown in Figure 2.
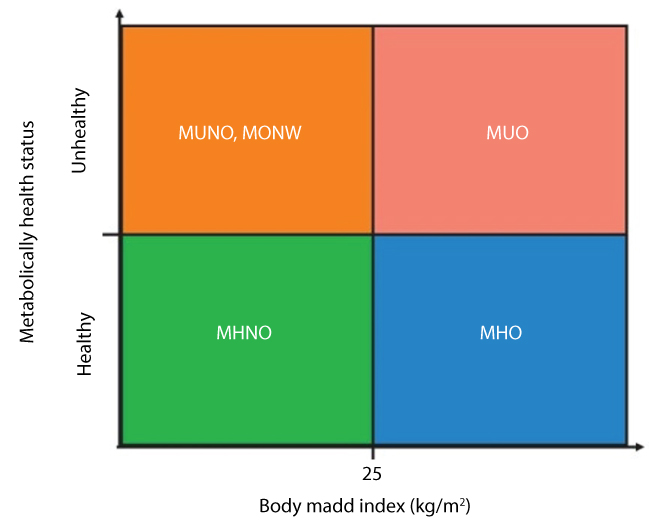 Figure 2: The metabolically health status.
View Figure 2
Figure 2: The metabolically health status.
View Figure 2
This research indicates that considerable temperature rise (6 ℃) may take place in a very short exposure time (0.25 minute) which may cause biological hazard. Table 5 shows the degree of biological hazard when embryonic/fetal temperature rise above 37 ℃ [26]. Table 6 shows the clinical side effect observed while ultrasound examination such as heating, headache and vomiting for the frequencies 3.5 and 6.5 MHz in the attenuation rate range (0.44-0.97).
Table 5: Degree above normal 37 ℃. View Table 5
Table 6: Clinical side effects. View Table 6
Overweight, Obesity in pregnancy are all related with an increased hazard of great maternal and fetoneonatal complications [27]. Obesity in women is related with a most incidence of amenorrhea. Most miscarriage in overweight and obese women undergoing in vitro fertilization procedures is at least threefold higher than it is in non-obese ones [25]. In addition, obesity and overweight in pregnancy have been related with an increased hazard of hypertensive complications, diabetes, thromboembolism and, consequently, of maternal mortality [27]. Adverse fetoneonatal effects of maternal obesity contain increased hazard of prematurity, macrosomia and stillbirth, congenital anomalies and neonatal death. As seen in Table 2, women in the urban region had significantly higher measures of all selected variables (p < 0.05). These findings are in good agreement with previously reported above. Several epidemiological studies have explained an increased incidence of congenital anomalies in the offspring of obese pregnant women. In case-control study [20], the authors explained that the neonatal incidence of a series of malformations was significantly increased in women with BMI > 30 kg/m2. These anomalies inclusive central nervous system malformations and neural tube defects (NTD), ventral wall anomalies conotruncal heart defects and other intestinal defects. Although other studies have not found such an association [21,23], a new meta-analysis reviewed all available data published in peer reviewed journals since 1980 and showed that the unadjusted odds ratios for an NTD affected pregnancy were 1.22 (95% CI, 0.99-1.49), 1.70 (95% CI, 1.34-2.15), and 3.11 (95% CI, 1.75-5.46) among overweight, obese and morbidly obese women, respectively, compared with women of normal weight [24]. Another multicenter case-control study showed a weak to average positive association of maternal obesity with seven of 16 categories of birth defect and a strong inverse association with gastroschisis [25]. In this study, the malformation categories for which the odds ratios were increased in overweight and obese women were: congenital heart disease, diaphragmatic hernia, anorectal atresia, hypospadia and limb reduction defects. The odds ratios for heart defects were also significantly increased in overweight women. Additional evidence of an increased hazard of congenital anomalies in the offspring of obese and overweight women as long as by various studies explained such an association [20-24]. It is important to confirm that there are other worthy studies, not listed in Table 4, that failed to explained any correlation between pregnant women being obese/overweight and increased hazard of malformations in the offspring. However, the amount of epidemiological studies showing such an association is large, as evident in Table 4. During the study period a total of 700 live born singleton infants were included in the group. Congenital heart defects were the most common malformation subtype (38.7%) followed by malformations of the diaphragmatic hernia (37.4%), limb reduction defects (12.7%), Hypospadia (6.9%), anorectal atresia (4.3%, Table 3). These findings are in good agreement with previously studies.
A number of theories have been put forward to explain the increased incidence of malformations in the offspring of overweight and obese women. The metabolic abnormalities of obesity, which include increased serum insulin, triglycerides, uric acid and endogenous estrogens, may have the same teratogenic 'fuel‐mediated' effect as maternal insulin‐dependent diabetes [28]. Chronic hypoxia and hypercapnia have also been considered as additional teratogenic factors in obese pregnant women. Obesity is associated with pre‐existing diabetes mellitus, but most studies demonstrating an increased risk of congenital anomalies in obese women have adjusted their odds ratios for diabetes. Finally, another possibility is that the folic acid supplementation dose usually considered adequate to reduce the incidence of NTD in the normal‐weight pregnant woman might be insufficient in the obese pregnant woman, due to lower gastrointestinal absorption and higher metabolic demands [28]. This hypothesis is supported by a case-control study on birth defects which demonstrated a daily intake of 400 µg folate to be protective against NTD in infants of women with a body weight ≤ 70 kg but not in infants of women weighing > 70 kg [28]. This concept is confirmed by another study demonstrating lower serum folate levels in women of childbearing age with a higher than normal BMI, even after control for intake [29]. The fact that insulin resistance triggers hyperinsulinemia, and that hyperinsulinemia in turn causes insulin resistance, makes the above conundrums even more interesting. Mechanisms whereby insulin secretion is enhanced in obesity need further exploration. Adipocytes may signal directly to beta cells to regulate insulin secretion [26], and therefore could drive hyperinsulinemia independent of blood glucose levels. In any case, opportunities abound for further exploration of the molecular mechanisms whereby chronic hyperinsulinemia modulates pathways that may lead to insulin resistance, such as adipose whitening and inflammation. Table 3 shows the frequency of malformation categories findings for this study by clinical survey and after increased birth delivery. All mechanisms implicit related between overweight/obesity and birth defects are unknown. Our study was to explore this association further by investigating the 700 samples in Urban - Rural. In generally, findings show risks associated with obesity and the studied birth defects. Body fat distribution has been identified as a risk predictor for other diseases. Interestingly, weight gain around the waist (abdominal adipose tissue accumulation) has been related with diabetogenic and inflammatory metabolic pathogenesis [30]. Thus, this finding may offer a guide to underlying mechanisms for the associations of obesity with birth defect risk. Obstetric Ultrasound biological effect and safety were talked by Stephen Bly and Michiel c. van [31]. They found that the obstetric ultrasound should be as low reasonably achievable because of the potential for tissue heating when the thermal index exceeds 1. They also recommended that while imaging the fetus in the first trimester, Doppler and colour Doppler should be avoided. Stephen and Michiel in their study attached the Table that relates the exposure duration to the temperature rise. Table 5 shows the degree of biological hazard when embryonic/fetal temperature rise above 37 ℃ [32]. These values are a compromise between conclusions of the National Council on Radiation Protection and the World Federation for ultrasound in Medicine and Biology. As urbanization continues to reach many communities in Sudan, there is a possible risk of a modulation in lifestyle. This may outcome in changes congenital Malformation risk factors, which may reduce the quality of life and increase the rates of premature deaths. In this study, the differences in prevalence of obesity and congenital Malformation risk factors was described. Results showed that indices of obesity and congenital Malformation were higher in birth urban residents.
The prevalence of obesity was higher in urban than in rural residents. Urban women had lower intake of fiber and fruits and higher intake of sweetened beverages. Compared to urban women and rural women reported the malformation categories among birth of urban women were higher than that among birth of rural women at 95% Confidence Interval. Higher level of obesity, physical inactivity, and poor diet among urban residents and the persistent higher risk of obesity among urban women call for more research into 'obesogenic' environments in urban Sudan. Effective programs are needed to help urban residents reduce high risks for obesity and unhealthy lifestyles. Weight, BMI, Percentage of Body fat, Waist Circumference and Waist: Hip Ratio (WHR) was significantly higher (p, 0.001) in Urban women as compare to Rural women. Compare risk factors by settlement (rural or urban) was studied. Participants in the urban area were more likely than rural residents. Maternal sociodemographic properties and life style behavior are associated with increased risks of maternal obesity and overweight during pregnancy. Together maternal, overweight and obesity are related with increased hazards of maternal and childhood health outcomes. In the future strategies, focused on pre-pregnancy BMI (means follow up BMI for women before pregnant), are needed to progress maternal pregnancy outcomes and health of offspring. However, fetal medicine experts and fetal medicine doctors, have a duty to draw the attention of healthcare professionals, patients, lawyers, insurers and health policy makers to yet another negative and costly effect of the irreversible and mounting wave of obesity: a significant reduction in the detection rate of congenital anomalies at the mid trimester screening ultrasound examination.
The authors declare that there are no personal, organizational or financial conflicts of interest.