High-flow nasal cannula oxygen therapy (HFNC) has revolutionized the treatment of patients with respiratory failure in different settings. Several mechanisms of action explain us why HFNC has become a first line therapy for these patients. Some authors have referred to the adverse effects that can occur when we use HFNC and its limitations. However, there are numerous aspects that we should consider when prescribing this treatment and that are not documented in the literature to date. In a Task Force carried on by International High-Flow Network members in Madrid, the things that should be taken into account when put a patient on HFNC were addressed. We will discuss in this article aspects related to the device, oxygenation, humidification, tubing, nasal cannula, alarms and finally, those related to the patient who receive the treatment.
High-flow nasal cannula oxygen therapy (HFNC) is an innovative respiratory support for critically ill patients with acute hypoxemic respiratory failure [1-5]. Moreover, recent studies suggested that HFNC is effective in hypercapnic patients with a stable status [6-8]. Its effectiveness in patients with different severity levels has facilitated its use in multiple areas of the hospital (emergencies, critical areas, ward...) [9-10] and there are already experiences of its use at home [11]. It consists in the administration of a gas flow that exceeds the patient's peak inspiratory flow, above 30 L/min in adults, heated to 37 ºC and with a humidity of 100% [12]. Although HFNC is not a mechanical ventilation system, it is considered more and more as a respiratory support system [13].
The mechanisms of action of the HFNC are multiple, highlighting its ability to increase alveolar recruitment, improve the ventilatory pattern, generate a positive expiratory pressure (PEEP) and produce dead-space CO2 washout [14]. By providing the gas breathed at 37 ℃ and 100% humidity, the HFNC is better tolerated and more comfortable for the patient [15]. It has been proven that when the patient breathes with a closed mouth, the pressure achieved is optimized, maximizing the dead-space CO2 washing effect if the patient breathes with an open mouth [16]. These HFNC effects have placed this therapy in the first line of treatment of patients with hypoxemic respiratory failure and as a main alternative in patients with hypercapnic respiratory failure when they do not tolerate noninvasive ventilation (NIV), reject it or is contraindicated and when NIV fails in patients not subsidiary of intubation and invasive ventilation [17-18].
The evidence for HFNC use in adults has increased exponentially year after year since the publication of the first study in 2008 [19]. Some authors have referred to the adverse effects that can occur when we use HFNC and its limitations [20]. However, there are numerous aspects that we should consider when prescribing this treatment and that are not documented in the literature to date. The fact that in the end the patient receives the therapy through a nasal cannula does not mean that the patient is not critical or does not require monitoring [21]. We should not trivialize HFNC therapy. In a Task Force carried on by International High-Flow Network members in Madrid, the things that should be taken into account when put a patient on HFNC were addressed. Many of the comments herein are the result of the experience of Task Force members. We are going to refer mainly to the Airvo 2 device (Fisher & Paykel, Auckland, New Zealand) because it is the most used device in our daily practice in the hospitalization and emergency facilities, also being used in critical areas. The integrated flow generator delivers a wide flow range (10-60 L/min for adults' patients) and no wall air supply is required in the AIRVO 2. The high-flow devices that generates the flow through oxygen and air intakes to the wall, such as the Opti flow (Fisher & Paykel, Auckland, New Zealand), can pose significantly different problems by not integrating turbine, although many of the comments here are applicable.
We will review the main aspects to consider and potential problems that we can find when we use the HFNC (Table 1). We will discuss the aspects related to the device, oxygenation, humidification, tubing, nasal cannula, alarms and finally, those related to the patient who receive the treatment.
Table 1: Aspects to be consider when put a patient on HFNC. View Table 1
This, which seems obvious, is a very important aspect. The adequate selection of the flow and FiO2 that the patient needs is key to achieve the proposed objective.
- Flow: It has been recommended in the literature to start with low flows (30-35 L/min) and to go up as tolerated by the patient [22]. However, Mauri, et al. [23] have shown that the flow that achieves the greatest effect on the mechanisms of action of the HFNC is 60 L/min. That is, if we want to optimize the alveolar recruitment, the dead-space CO2 washout, the PEEP or the decrease in airway resistances, we should apply 60 L/min, especially in situations of acute respiratory failure, where the most important thing is improve the patient as quickly as possible. These authors always recommend that if the patient tolerate it, we should start therapy at 60 L/min.
- FiO2: Another important aspect is the adequate regulation of FiO2. The HFNC is not strictly a novel oxygen therapy system [17,24]. Although the name may induce misunderstandings, administering high flow is not synonymous to administering a high FiO2. The Airvo 2 turbine, for example, can generate 60 L/min of flow although we do not add oxygen to the circuit. Therefore, we can apply HFNC safely in hypoxaemic and hypercapnic patients, following international recommendations to achieve SpO2 of 94-98% in the former and 88-92% in patients at risk of hypercapnic failure, adjusting a correct FiO2 [25].
A problem to be taken into account in critically ill patients is how to interpret the PaO2/FiO2 assessment because there is no information about the real PEEP that the HFNC can generate. In the classification of Berlin [26], acute respiratory distress syndrome (ARDS) has been classified as mild, moderate and severe, depending on the degree of hypoxemia (PaO2/FiO2) presented with a minimum PEEP of 5 cm of water. By not knowing the real PEEP achieved in the HFNC, we can make mistakes when classifying the patient with ARDS, labeling patients with mild ARDS as more severe.
We should not place the patient on HFNC therapy immediately after switching on the device. When we assemble the equipment, and turn it on, we should wait a few minutes until the device reaches the programmed temperature and degree of humidification. Its immediate use can cause discomfort to the patient, who begins to receive a high flow of cold and dry gas. This could be the reason why he does not tolerate the technique.
We should not block or insert anything inside the ventilation slots. The Airvo 2 integrates a turbine responsible for generating the selected flow. The room air enters through a subsequent ventilation slot that must be open and clean. It is an error to cover it with rags, towels or gauze, or to place the equipment stuck to the wall or to the bed. These measurements are applicable to the air inlet of all high flow devices.
The filter must be clean, and we should respect the maintenance program of the manufacturer and thus avoid failures in the air intake to the turbine due to obstruction. When this occurs, the equipment may not be able to reach the programmed flow, with the corresponding alarm appearing (Figure 1).
 Figure 1: A dirty filter can compromise the efficiency of the turbine.
View Figure 1
Figure 1: A dirty filter can compromise the efficiency of the turbine.
View Figure 1
The equipment must be disinfected after use with each patient. For this, the manufacturer provides a special tube that, once placed correctly, activates a countdown of one hour when turning on the device, which automatically turns off once disinfected (Figure 2). The incorrect placement of the tube or the non-disinfection of the equipment after its use, are errors that we must avoid.
 Figure 2: Fisher & Paykel desinsection tube placed in right position.
View Figure 2
Figure 2: Fisher & Paykel desinsection tube placed in right position.
View Figure 2
We should not trust when we use HFNC, but above all we should be very cautious in critical patients. In these patients, a cut in the power supply can cause a serious health problem. The absence of a battery prevents the device from being used in in-hospital patient's movements (radiology, for example), unless it is connected to an external battery. Moreover, patients cannot go to the toilet unless they interrupt therapy, which is not always possible. It is something that we must consider if the patient cannot stop the treatment. Upcoming versions of Airvo will include internal battery bypassing this problem.
When applying HFNC we have to select the flow and the FiO2 required by the patient. The O2 intake of the Airvo 2 is located on the right side of the device. This does not have a mixer but informs the FiO2 that we are administering the patient according to the flow of O2 that we provide. The O2 can come from a conventional flowmeter, recommended when we want low FiO2 as is the case of hypercapnic patients. It can also come from a high-flow flowmeter with direct intake to the wall, recommended in patients requiring high FiO2. We should not forget in this case, connect the high-flow flowmeter to the O2 outlet of the Airvo 2, an error that we have sometime seen and that causes not to achieve the desired FiO2 despite increasing the flow in the flowmeter (Figure 3).
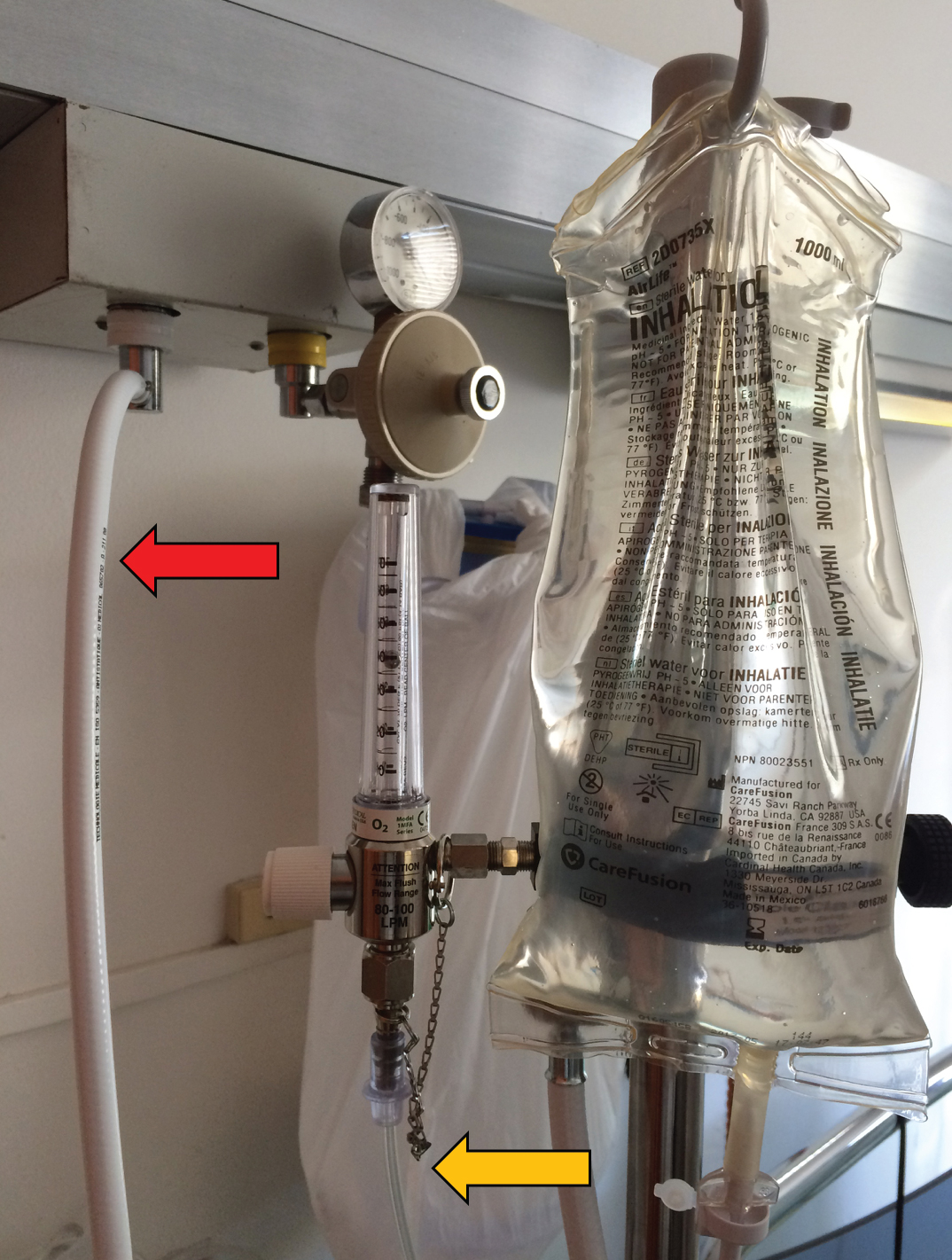 Figure 3: The O2 can come from a conventional flowmeter, recommended when we want low FiO2 as is the case of hypercapnic patients (orange arrow). It can also come from a high flow flowmeter with direct intake to the wall, recommended in patients requiring high FiO2 (red arrow). We should not forget connecting the right O2 tube to the O2 outlet of the Airvo 2.
View Figure 3
Figure 3: The O2 can come from a conventional flowmeter, recommended when we want low FiO2 as is the case of hypercapnic patients (orange arrow). It can also come from a high flow flowmeter with direct intake to the wall, recommended in patients requiring high FiO2 (red arrow). We should not forget connecting the right O2 tube to the O2 outlet of the Airvo 2.
View Figure 3
When adjusting the oxygen level from the source, it may take a few minutes until the correct FiO2 is displayed on the device's display.
Airvo 2 has an internal menu where we can select temperature, flow and FiO2 alarms. For example, if we do not want a certain FiO2 to be exceeded, we can select it from the inside menu. Each time this FiO2 is reached, a high FiO2 alarm will sound. You should think about this possibility if the device alarm sounds repeatedly and all is working apparently normal. If this occurs, change the threshold of it. Another aspect related to the FiO2 alarm is that it cannot be completely canceled, being its limits 21 and 100%. When we want to manage a FiO2 of 100%, the alarm will sound continuously. It is advisable to maintain a FiO2 lower than 100% to avoid this alarm.
When disconnecting the patient from the HFNC, temporarily or permanently, we should not forget to connect the conventional oxygen therapy modality that we want to maintain (nasal cannula, venturi mask, O2 attached to ventilator...) to the correct flowmeter. Sometimes we have several O2 outlets on the wall and we can put the patient connected to one that is not working (Figure 4).
 Figure 4: This patient has several O2 supply possibilities to be treated: a) Cannula nasal; b) Venturi mask; c) High flow nasal cannula; d) Nebulizer; and e) Noninvasive ventilation mask, f) Two double flowmeter, g) A ventilator, too many tubes, several possibilities to make a mistake.
View Figure 4
Figure 4: This patient has several O2 supply possibilities to be treated: a) Cannula nasal; b) Venturi mask; c) High flow nasal cannula; d) Nebulizer; and e) Noninvasive ventilation mask, f) Two double flowmeter, g) A ventilator, too many tubes, several possibilities to make a mistake.
View Figure 4
Lastly, like any device that uses oxygen, care must be taken with the risk of fire. It is unnecessary to say that neither health care professionals nor patients should smoke in the presence of a patient with HFNC.
High-flow equipment requires water for the humidification of the breathing gas. The water must be sterile water or water for inhalation. Saline or glucose solutions should not be used and thus avoid damage to the device (manufacturer's recommendation).
It is recommended to use plastic bags instead of glass bottles. The latter can generate interruptions in the filling circuit of the humidifier vessel due to surface tension phenomena, which would give rise to specific alarms (manufacturer's recommendation).
It is important to maintain open the cap that comes with the Airvo 2 consumables next to the connection with the water bag, to avoid vacuum phenomena inside the bag and hindering the filling of the humidifier chamber. If we work with other manufacturers, we must observe the established recommendations to avoid this problem.
We should avoid that the device runs out of water, replacing the bag when necessary and being alert to possible obstructions in the circuit.
In this regard, it is important to assemble the consumable elements in a right way to give stability to the connection of the water inlet tube in the humidifier chamber and to avoid undesirable obstructions that hinders the filling of the chamber (Figure 5).
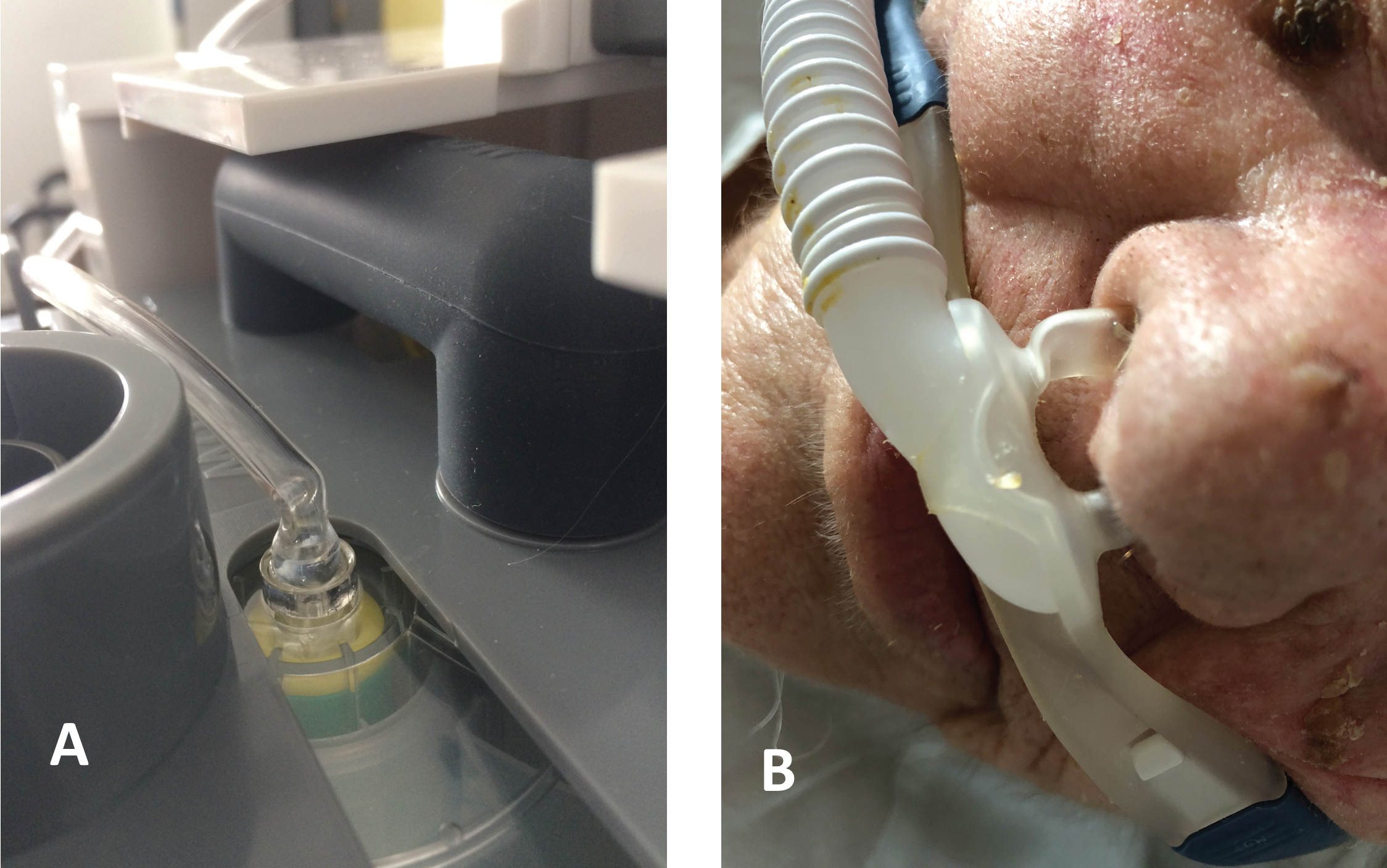 Figure 5: a) Obstruction near the humidifier chamber; b) Obstruction of the nasal cannula. We should be vigilant to these problems.
View Figure 5
Figure 5: a) Obstruction near the humidifier chamber; b) Obstruction of the nasal cannula. We should be vigilant to these problems.
View Figure 5
The tube of the high-flow device incorporates a gas heating system inside it to avoid condensation phenomena. This is achieved, generally, with an electrical resistance. We should check that it works correctly and that the proper temperature is maintained in the tube. In the event of rupture or damage in the tubing heating system, which may occur in patients with prolonged use of the HFNC, we should proceed to replace it.
We should also pay attention to the appearance of breaks in the tube, which would generate an undesirable leak.
It is very important that the tubing is always below the patient. In this way, we avoid that water condensation, if it occurs, can enter the airway. Moreover, we prevent pressure injuries in the nasal mucosa and obstructions of the flow, secondary to undesirable upper traction of the nasal cannula.
It is necessary to avoid that the weight of the tube falls on the nasal cannula. We should prevent it from hanging between the device and the patient's face, using the anchor pieces provided by the manufacturer to the clothes or the sheets, freeing the patient of this weight. As a rule, it is important to take the necessary precautions, so the tubing is not a discomfort for the patient.
The nasal cannulas are a very important piece in the HFNC therapy. They are the element that contacts the patient and must allow the supply of programmed flow. There are different sizes approved by the manufacturer to generate nasal flow according to the reduction of the radius in the circuit that occurs when passing from the tube to the cannulas. The pressures that are achieved when administering HFNC depend on two factors: The flow and the size of the nasal cannula [27-28]. It has been demonstrated that when we use larger nasal cannulas, the occlusion of the nasal passages is greater and higher pressures are achieved in the nasopharynx. On the contrary, when we use cannulas that occlude less than 50% of the nostrils, the pressure that is obtained is lower. The smaller the section of the nasal cannula, the greater the pressure that will be reached in the nasopharynx (Pressure × Speed must be kept constant, simplified Bernoulli principle) and that this will also depend on the anatomy of the nasopharynx itself [29]. We should select the correct nasal cannula for our patients based on tolerance and objectives.
The nasal cannula must be suitable and recommended by the manufacturer for your equipment. Sometimes nasal cannulas are not compatible with the tube and we can see how doctors have used adhesive tape to join them.
Poor placement can cause blockage of the cannula if its tip contacts the nasal mucosa or injuries due to rubbing or decubitus. This can be a cause of patient complaints, bleeding or alarm signal due to cannula obstruction.
It must be borne in mind that in the HFNC the patient is supplied with a humidified and hot gas. This can cause vasodilation of the nasal mucosa and problems of abundant mucus or aqueous rhinitis, which can compromise the tolerance and effectiveness of the technique. It is important to maintain an adequate nasal hygiene, with periodic cleaning of the mucus or even having to use topical corticosteroids to control rhinitis if it appears. Nasal mucus can cause blockage of the cannula.
The nasal cannulas have a pad to improve patient comfort and are attached to the patient's head by a harness. Like non-invasive ventilation, when HFNC therapy is prolonged for extended periods of time, it is possible that decubitus ulcers are generated inside nasal cavities, in the occipital region or in the auricle. This may be important if the patient presents abnormalities or previous surgeries on the face, nose or airways, that prevent proper adjustment of the nasal cannula. We should be alert to this possible problem and prevent it with appropriate actions on the harness and the position of the nasal cannulas, even if necessary using hyperoxygenated fatty acids in the decubitus areas.
As we have said, the Airvo 2 incorporates an internal menu where we can select temperature, FiO2 and flow limits, which will make the alarm go off if they are exceeded. It is important to check these limits in case alarms are triggered by excess or defect of these variables.
The devices can emit alarms for not being able to reach the prescribed flow or temperature, due to lack of water in the humidifier chamber, due to excess or defect of FiO2 or flow, due to leakage and internal failure, mainly. If any of these alarms appear, all the aspects referred above must be checked until the cause of the alarms is found.
HFNC is mainly used in patients suffering of acute respiratory failure. These are patients with increased respiratory work and dyspnea. Although the HFNC delivers a high, humidified and heated flow, this is not always an advantage. The patient sometimes regrets receiving a lot of heat and air flow that initially bothers him. In the Task Force member's experience, the most common complaints of patients are the following:
1. Nose: Too much pressure, what displeases and irritates the nostrils. Disturbances that may be aggravated if rhinitis, nasal mucus or epistaxis appears, as discussed above.
2. Paradoxical suffocation: The patient can paradoxically refer "suffocation" due to the intense arrival of constant air associated with difficulty in expiration because of its resistance to airflow.
3. Chest pressure: In the same sense, there are patients who experience discomfort due to chest pressure.
4. Understanding high-flow therapy: The patient does not understand the concept of high-flow therapy because he believes that the treatment is not useful if the air comes out through the mouth. The importance of proper health education is also crucial in high-flow therapy.
5. Mobility: Other complaint, which also occurs with NIV, is the need to be connected to this treatment constantly. That is, there is a limitation when the patient wants to move, including going to the bathroom, worsening their quality of life and decreasing their autonomy.
6. Noise: As an external device that generates a high flow, it causes a noise that can be annoying especially if we put high O2 flow in the flowmeter, which is uncomfortable for the patient. Kubo, et al. [30], have demonstrated that the noise level of HFNC/Venturi could be reduced by attaching an intake filter.
7. Claustrophobia: Some patient complains of claustrophobia.
8. Intolerance: Together, it may happen that due to the reasons previously exposed, the patient presents intolerance and rejects the technique.
9. Pneumothorax: HFNC should not be applied if untreated pneumothorax. The risk of barotrauma is probably lower with HFNC than with non-invasive ventilation or mechanical ventilation after endotracheal intubation. The role of HFNC in the development of pneumothorax is difficult to determine and the few cases reported are related to postoperative patients, without being able to determine if the type of patient could be the true determinant of this complication [20,31]. By the contrary, HFNC has been shown to be useful in patients with pneumothorax [32]. As with non-invasive ventilation, HFNC should not be applied to patients with untreated pneumothorax.
In conclusion, HFNC therapy is not as simple as it seems, and many things have to be taken into account when we put a patient on this therapy. We should pay attention to aspects related to the device, oxygenation, humidification, tubing, nasal cannula, alarms and finally, those related to the patient who receive the treatment. We can be in front of a device with the latest technology, however it can fail. As we can see, HFNC is not just a device to turn on and off. The training of health professionals is essential to ensure the proper use of the technique and patient safety. Adaptation and training are also necessary for the patient and the caregiver in cases of long term HFNC prescription. This review aims to highlight some of the innumerable aspects that we should not forget when treating patients with HFNC and have interest in clinical practice. Training is necessary because the devil is in the detail.
Authors declare do not have any conflict of interest related to the publication of this manuscript. They have not received any amount of money, and do not have any grant or sponsor for writing it.