Background: Type 2 Diabetes mellitus is a chronic metabolic disease with significant implications on health status and quality of life (QoL) in terms of physical, social, environmental, and psychological well-being. Old age also has a significant influence on QOL, therefore, the impact of diabetes on the QOL of older persons can be more severe. In managing these older diabetics attention needs to be paid to the clinical and sociodemographic factors that may impact their QOL so that these can be modified where possible.
Aim: This study aimed to determine the clinical and socio-demographic predictors of poor quality of life among older type 2 diabetes patients attending the family medicine clinic LASUTH, in order to address the modifiable predictors.
Methodology: This was a descriptive cross-sectional study involving 384 consenting older type 2 diabetes patients recruited using the systematic random sampling method. An interviewer-administered structured questionnaire was used to gather information about their socio-demographic characteristics and clinical history. The structured WHO QoL-BREF questionnaire, the Multidimensional scale of Perceived Social Support (MSPSS), and the Morisky Medication Adherence Scale (MMAS-8) were used to obtain information for quality of life and its predictors. Glycosylated Hemoglobin (HbA1c) was also assessed. Data were analyzed using SPSS 27.
Results: About seventy percent of respondents had a poor overall quality of life. The mean QOL scores in the physical, psychological social, and environmental domains were 60.72, 55.32, 58.09, and 62.00 respectively. The identified Predictors of poor quality of life were; Average monthly income of less than 50,000 naira (OR- 2.023, p-0.009), sedentary life style (OR- 1.774, p- 0.041), presence of co-morbidity (OR- 3.442, p < 0.001), duration of diabetes less than 5 years (OR 2.632 p- 0.007), medium medication adherence (OR-1.834, p-0.045) low medication adherence (OR- 2.513, p- 0.007), as well as low and moderate perceived social support (OR 2.302, p- 0.007) and (OR- 2.192, p- 0.005) respectively.
Conclusion: Close attention should be paid to older diabetics with a duration of diabetes < 5 years who have co-morbidity, poor medication adherence, sedentary life style, monthly income < 50,000 naira, and low/moderate perceived social support, as they are more likely to have poor QOL. Modifying these factors early in their treatment is essential.
Older adults, Type 2 Diabetes, Quality of Life (QoL)
Historically the United Nations has defined an older person as anyone 60 years and above, irrespective of history or residence [1]. The World Health Organization (WHO) ascribes the age of 65 years and above to the elderly. However, developing countries including Nigeria denote the elderly as people aged 60 years and above because of their low life expectancies [2]. About 5% of the over 200 million persons in Nigeria are aged 60 years and above [3]. As of 2020, 9.4 million people were aged 60 years and older [4], women made up 46 percent of the elderly population and men made up 54 percent of that population in Nigeria [4]. This number of older adults is projected to rise to about 25.3 million by 2050 [3].
The term Diabetes characterizes a group of metabolic disorders identified by the presence of hyperglycemia in the absence of treatment [5]. The aetio-pathogenesis includes defects in insulin secretion, insulin action, or both, and disturbances of carbohydrate, fat, and protein metabolism [5], which eventually leads to significant impairments in the heart, blood vessels, eyes, kidneys, and nerves [6].
The most common classification of diabetes are; Type 1, Type 2, and Gestational diabetes [7], although, there have been recent calls to review and update the classification system for diabetes. This is because many people with diabetes do not belong to any single category, in addition there are recent advances in knowledge of pathophysiological pathways. This brought about the updated WHO classification of diabetes [5]; however, the most common is still type 2 diabetes which accounts for about 90-95% [8] of all cases of diabetes.
Diagnostic criteria for Diabetes Mellitus; Random plasma glucose value of ≥ 200 mg/dl (≥ 11.1 mmol/l) or Fasting plasma glucose value of ≥ 126 mg/dl (≥ 7.0 mmol/l) or 2- h oral glucose tolerance test (OGTT) value in venous plasma ≥ 200 mg/dl (≥ 11.1 mmol/l) or HbA1c ≥ 6.5% (≥ 48 mmol/mol Hb) [9].
Good glycemic control which is defined as HbA1c < 7.0% in the general populace is fundamental in diabetes care [10,11]. This includes the elderly population.
Risk factors for type 2 diabetes include; weight gain, inactivity, family history, ethnicity, age, hypertension, gestational diabetes, polycystic ovaries, and dyslipidemia [12]. Complications include cardiovascular disease, neuropathy, retinopathy, and nephropathy [13]. A study by Huang, et al. reported that among older adults with diabetes, cardiovascular complications followed by hypoglycemia were the most common nonfatal complications [14]. The study concluded that the duration of diabetes and advancing age independently predict diabetes morbidity and mortality rates [14].
The World Health Organization (WHO) defined Quality of Life (QoL) as individuals’ perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, standards, expectations, and concerns [15].
In patients with diabetes, multifactorial reasons result in lower scores of QOL including comorbidities like hypertension, coronary artery disease, arthritis, glaucoma/cataract, hypercholesterolemia, and bladder outlet obstruction in men [14,15]. As well as being expensive to control and treat, diabetes also has a deleterious effect on the quality of life (QoL) of the older adults [16].
Personal characteristics such as age, gender, education, and occupation; disease characteristics such as age at onset, duration of illness, type of diabetes, treatment regimen, complications, and lifestyle characteristics such as dietary habits, smoking behaviour, physical inactivity, and exercise are common predictors of QoL [17]. A study conducted in southwestern Nigeria reported that psychological and social relationships are the most important predictors of QoL for this population [18]. In addition, uncontrolled T2DM is linked with poorer QoL and health status of patients [19].
Although physical health is generally regarded as significant for QoL, other domains viewed as integral to QoL, especially in the elderly are psychological well-being, social relationships, independence, mobility, and environmental safety [20,21]. This broad range concept implies identifying psychosocial variables (e.g., patient empowerment, knowledge of DM, medication adherence, monthly income, social support) that are associated with QoL and these factors could be influenced by age, gender, body mass index (BMI), and co-morbidities (sociodemographic and clinical characteristics) [20].
Several local studies have been done looking into the quality of life of diabetic patients but there is a paucity of data as regards the older diabetics, hence this study was carried out to determine the clinical and sociodemographic predictors of poor quality of life among older type 2 diabetics attending family medicine clinic LASUTH, who are a significant group worthy of attention in our environment.
This cross-sectional study was carried out at the family medicine outpatient clinic of The Lagos State University Teaching Hospital (LASUTH) between June 10 th and September 9 th , 2022. Three hundred and eighty-four consenting older adults with T2DM were drawn from the following clinics under the Family Medicine Outpatient Clinics (Care of the older persons’ clinic, Chronic medical disorder clinic and the Lifestyle medicine Clinic). Ethical approval was obtained from the Health and Research Ethics Committee of LASUTH with HREC number: LREC/06/10/1772. The participants were provided with both written and verbal information regarding the study. Informed consent forms were signed by the study participants and they were free to withdraw from the study at any time.
The inclusion criterion included; Older persons aged 60 years and above with T2DM diagnosed ≥ 6 months at presentation and consented to participate in the study. Exclusion criteria; (a) Patients with impaired cognitive functioning who found it difficult to give accurate answers, (b) Patients who require emergency care or who were too ill to participate. The following demographic, clinical and anthropometric information was collected; age, gender, education, monthly income, level of physical activity, duration of illness, treatment type, and level of physical activity. Interviewer based questionnaires containing items on, quality of life, perceived social support, and medication adherence were also obtained. Capillary blood samples were obtained using lancet needles to prick the thumb to determine the glycosylated hemoglobin (HbA1c). The blood samples were analyzed using the Clover A1c machine, which has been validated by the International Federation of Clinical Chemistry. HbA1c values of < 7% was taken for good glycemic control while HbA1c of ≥ 7% is poor glycemic control.
The World Health Organization Quality of life (WHOQOL) - BREF Questionnaire. It is an abbreviated 26-item version of the WHOQOL-100. It is a validated tool for assessing the quality of life with good internal consistency (Cronbach alpha 0.72 to 0.82) [22]. The WHOQOL-BREF has four domains scores and two individually scored items about individual overall perception of quality of life and health (Q1 and Q2).
The four domains that were assessed are physical, psychological, social relationship and environment domains, including the two individual scores on the perception of quality of life and health. Thereafter the overall mean score was computed. The raw score was calculated by straight forward summative scaling of the consistent item of the domain. These raw scores were transformed to a linear scale of 0-100 where 0 is the worst score possible and 100 best score possible [23].
Poor Quality of Life in this study were those who scored below 70% in a domain while those who scored 70% and above were categorized as having a good QOL [18].
The Multidimensional Scale of Perceived Social Support (MSPSS) comprises of 12 items rated on a 7-point Likert scale (response form ranges from, 1 = very strongly disagree to 7 = very strongly agree). The MSPSS assessed satisfaction with social support from family (FA), Friends (FR), and significant others (SO) [24]. Each domain is divided by 4. In this approach any mean scale score ranging from 1 to 2.9 is considered low support; a score of 3 to 5 were considered moderate support; a score from 5.1 to 7 is considered high support [24].
The total MSPSS was computed using the 12 questions with minimum and the maximum score for each question being 1 and 7 respectively and a total possible score range from 12 to 84. The categorization of the overall perceived score is as follows: Low, medium and high perceived support, which has been reported to have high internal consistency with Cronbach’s alpha of 0.86 [24].
Morisky Medication Adherence scale was used to assess the patient's experience with medications during the last two weeks before answering the questions. It is an eight item structured, self-reported questionnaire. The instrument was selected for use because it has been validated in Nigeria with Cronbach’s alpha of 0.83. The response categories are “Yes” or “No” for items 1 to 7. The questions are reverse-coded (Yes = 0, No = 1) except for item 5 (Yes = 1, No = 0). Item 8 has a 7-point Likert response from never/rarely to always. A score of 8 signifies high adherence, 6- < 8 signifies medium adherence while < 6 signifies low adherence [25].
Data entering, cleaning, and analysis was done using the Statistical Package for Social Sciences (SPSS) version 27. Mean and standard deviation was used to present normally distributed continuous data. Frequency, percentages, and charts were used to present categorical data. Chi-square was used in bivariate analysis to access the association between categorical variables. Quality of life was the dependent variable while the independent variables were clinical and sociodemographic predictors. The level of statistical significance was set at a p-value < 0.05.
Type 2 DM in this study refers to a patient with presence of a prior history of usage of oral hypoglycemic agents or usage of a combination of insulin and the oral hypoglycemic agents [26].
Older type 2 Diabetics in this study refers to T2DM patients that are 60 years and older and who have been diagnosed to be diabetic for at least six months, receiving treatment and follow-up care at the family medicine clinic LASUTH.
Poor Quality of Life in this study refers to those who scored below 70% in overall score of the WHO QoL tool, while those who scored 70% and above were categorized as having a good QOL [9].
Clinical characteristics of interest: Glycaemic control, Medication adherence, Disease characteristics (duration of illness, co-morbidities, treatment type), Body Mass index (BMI), and Physical activity.
Socio-Demographic characteristics of interest: Age, Gender, Educational level, Perceived social support, and monthly income.
A total of three hundred and eighty-four (384) type 2 DM respondents were recruited from the Family Medicine clinics into the study over a period of three months. They were aged 60-92 years [mean 68.64 ± 7.2 years] and there were more females [n = 260 (67.7%)] than males [n = 124 (32.3%)] respondents with a female-to-male ratio of 2.1:1. About one-third (31.0%) of the respondent had secondary education while about half (51.0%) were married. About three-quarters were Christians (74.2%), while 71.4% were of the Yoruba tribe. About one-third (36.7%) had an average monthly income of 50,000 to 100,000 naira, almost half (40.1%) spent over 200,000 naira on drugs in the last year, while about half (49.7%) of the respondents had high overall perceived social support. Other details of the sociodemographic characteristics are displayed in Table 1.
Table 1: Socio-demographic characteristics of participants. View Table 1
Almost half (46.9%) of the respondents have had diabetes for over 10 years. Over nine tenth (92.7%) of the respondents were non-current smokers at the time of the interview while almost three-quarters (74.7%) did not consume alcohol. Almost two-thirds (65.8%) of the participants were sedentary. More than four-fifths (83.3%) of the respondent were on oral medications alone while over three-quarters (79.4%) had co-morbidity. Hypertension was the commonest co-morbidity recorded (63.3%). About two-fifths (42.2%) were overweight. About half (50.5%) of the study participants had poor glycaemic control, in addition almost half (44.6%) of the respondents had high medication adherence. Other details of the clinical characteristics are displayed in Table 2.
Table 2: Lifestyle and clinical characteristics of participants. View Table 2
The overall mean QOL score was 63.37 ± 10.6. The mean QOL scores in the different domains are also shown. The QOL of respondents in different domains was also classified into good or poor QOL. Table 3 shows the details.
Table 3: Quality-of-life scores using the WHO QOL BREF. View Table 3
From Table 4, and Table 5, respondents with average monthly income < 50,000 naira were 2 times (OR- 2.023, p-0.009) more likely to have poor quality of life, those who had sedentary life style were about 1.8 times (OR -1.774, p-0.041) more likely to have poor quality of life, those with presence of co morbidity were three and half times (OR- 3.442, p < 0.001) more likely to have poor quality of life. Also those with duration of diabetes < 5 years were 2.6 times (OR 2.632 p- 0.007) more likely to have poor quality of life, those with low medication adherence were two and half times more (OR- 2.513, p- 0.007) likely to have poor quality of life. While those with low and moderate perceived social support were 2.3 times and 2.2 times respectively (OR 2.302, p- 0.007) and (OR- 2.192, p- 0.005) more likely to have poor quality of life.
Table 4: Relationship between quality of life and socio-demographic/ lifestyle characteristics. View Table 4
Table 5: Relationship between quality of life and clinical characteristics. View Table 5
Diabetes, generally speaking, brings about poor physical, social, environmental, and psychological health, which leads to limitations in physical functioning and mental health, lowering the QOL among older adults [27]. Several studies have revealed that the QOL in “older adults with diabetes” is reduced compared to non-diabetics [20,28,29]. As the world’s diabetic and aging populations have grown in recent years, the requisite for health upgrades and planning to improve all aspects of life in this group of individuals has become paramount [30,31]. This peculiarity tends to decrease the ability of the older adult to remain independent in both basic and instrumental activities of daily living [32]. It is, therefore, necessary to recognize the consequences of having the additional diagnosis of diabetes in this age group.
The sociodemographic characterization revealed a higher predominance of female older persons, those aged < 70 years, who were married, had at least a primary school education, a low income and spent more on drugs and investigations. Similar results were found in other studies in relation to age, gender, education, and income [29,33-35]. This is in contrast to findings by Lima, et al., in brazil who found higher preponderance of male participants, unmarried and illiterates among older T2DM patients.
A majority (70.1%) had poor overall QOL in this study. This is in contrast to a Saudi Arabian study by Alghamdi, et al. who found high overall QOL among older adults with T2DM [36]. Factors that could have influenced the higher value of overall poor quality of life in this study include duration of illness < 5 years, sedentary life style, presence of co-morbidity, and poor medication adherence, which have all been found to be significant predictors of quality of life [20,37]. In this study the highest domain score was found in the environmental domain, this is in contrast to the findings by Santos, et al. in a cross-sectional study in Brazil among elderly individuals with DM living in both urban and rural areas. It was reported that the social relationship domain had the highest QOL scores in both the rural and urban areas [38]. This could have been because the Brazilian study was a community-based study that included a rural setting where there was likely a communal relationship that will lead to an increase in social connectedness (Figure 1).
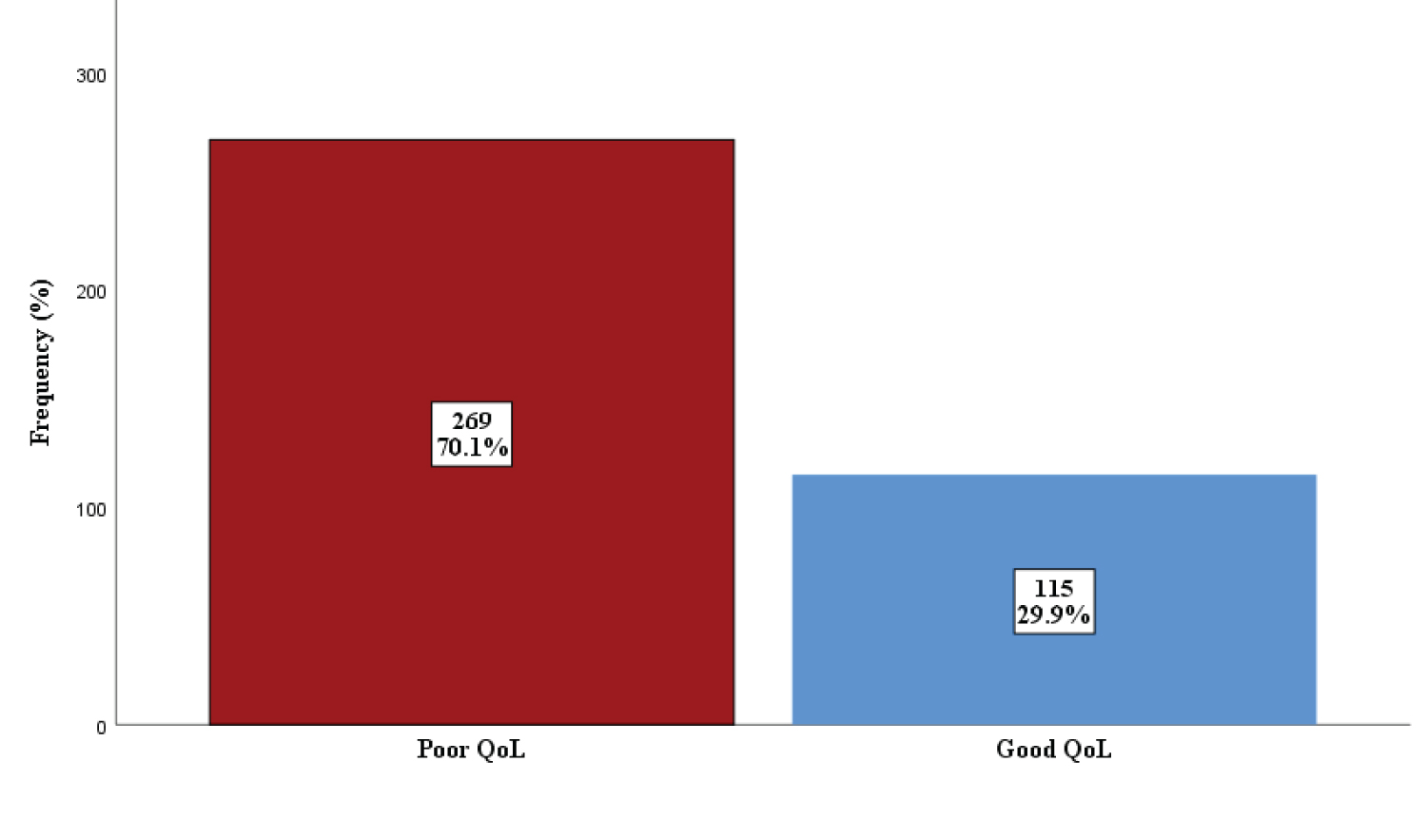 Figure 1: Overall quality of life using WHO QOL BREF.
Figure 1: Overall quality of life using WHO QOL BREF.
When classified into good (i.e. ≥ 70%) or poor (< 70%), 70.1% of respondents had poor QOL while 29.9% had good QOL.
View Figure 1
In this study QOL was associated with age (p-value 0.030), educational level (p-value 0.007), monthly income (p-value 0.018), perceived social support in the friends’ subscale (P = < 0.001), and overall perceived social support (P = 0.004). However, only an average monthly income of < 50,000 naira, and moderate and low overall perceived social support were independent predictors of poor QOL among the sociodemographic predictors. An average monthly income of < 50,000 Naira was an independent predictor of poor QOL in this study. This is in contrast to a cross-sectional Hospital based study by Moghaddam among elderly patients with T2DM in Iran. It was reported that economic status was not a statistically significant predictor of QOL [39]. This may be because, in the latter study, more than half (65.4%) had an economically independent income. The low (OR 2.302, P- 0.007) and moderate (OR 2.192, P- 0.005) overall perceived social support were found to be independent predictors of poor QOL in this study. This is similar to findings in a Cross-Sectional study in Iran by Hekmati among elderly patients with Diabetes. It was reported that there was a significant correlation between Social Support and different aspects associated with QOL [40]. In addition, here in the southwest of Nigeria, Awobiyi, et al. conducted a community-based cross-sectional study on Perceived QOL and Social Support received by older adults, it was reported that there was a significant difference in QOL between those who lived with people (93.8%) compared with those who lived alone [41].
In this study there was a significant relationship between duration of illness of < 5 years, sedentary life style, presence of co-morbidities, medium and low medication adherence, and poor quality of life. This is similar to the findings in various studies conducted both locally and internationally [20,37,42]. The presence of co-morbidities was the most significant predictor of poor QOL in this study. A similar finding was reported in a hospital-based cross-sectional study by HV Nguyen among elderly patients with diabetes in Vietnam. It was reported that there was a significant association between QOL and several co-morbidities (e.g. hypertension) [43]. This may be because in both studies a higher number of respondents had a duration of diabetes greater than 5 years and 10 years, predisposing them to a greater risk of co-morbidity. In this study duration of diabetes of < 5 years was associated with poor quality of life which is similar to an Ethiopian study by Wonde, et al. who reported that the duration in months in which patients stayed with DM for more than 59 months was found to be a significant factor that improved the quality of life [44]. This could be because patients who have had the disease for a short time have had less time to learn/experience how to manage the newly evolving process, which consequently predisposes them to a lower QOL. On the other hand, longer disease duration may have allowed patients to learn more about the medications used for therapy and gain more confidence in themselves. In this study, unsurprising, it was found that 76.7% of those with low medication adherence had poor quality of life and it was also an independent predictor of poor QOL. A Saudi Arabian cross-sectional hospital-based study by Khayyat, et al. concluded that irrespective of the type of long-term condition, adherence status was found to be an independent predictor of all QoL domains [45].
This study being a cross-sectional hospital-based study was subject to some limitations. The various significant associations between the variables tested in this study were not necessarily causal. Only a prospective or randomized controlled study can confirm the causal relationship between these variables.
The present study is pertinent as it can guide health professionals who work mainly in primary care in the control and prevention of diabetes complications in older persons. Care for such older persons should be organized to promote a better QoL as the main predictors of quality of life in older diabetics have been identified.