Symptomatic gastrointestinal metastases from lung cancer were considered quite rare given their low incidence, especially the duodenal location.
In this article, we report a clinical case of a patient followed for a pulmonary adenocarcinoma revealed by a duodenal metastasis. The patient was a 63-year-old female. She was admitted to the oncology department of the Ibn Rochd University Hospital for a low digestive hemorrhage ''Melena'' complicated by acute anemia. Duodenal metastasis from a primary adenocarcinoma of the lung was diagnosed following histopathological examination supplemented by immunohistochemical analysis of biopsies of the duodenal mass taken under gastrointestinal fibroscopy.
Post-mortem studies have confirmed that large cell lung carcinoma is significantly associated with gastrointestinal metastases with an incidence ranging from 30% to 75.9%. For this reason, physicians should consider secondary gastrointestinal locations if patients with lung cancer exhibit digestive symptoms and not relate this symptom to side effects of chemotherapy.
Lung cancer, duodenal metastasis, acute anemia, Melena
Lung cancer is the leading cause of cancer death worldwide [1]. This is largely because it is mainly diagnosed at an advanced stage of the disease. Lung cancer revealed by symptomatic gastrointestinal metastasis is extremely rare. Only 0.3% to 1.7% of cases have been described in the literature [2]. However, the incidence of cases of secondary digestive localizations discovered on autopsies shows that they are not uncommon as known, with an incidence varying from 4.6% to 14% [2,3].
Gastrointestinal metastases indicate advanced disease. The patient may present with a clinical picture of complication such as perforation, obstruction or gastrointestinal bleeding. In these cases, the survival rate is limited to a few weeks or a few months [4].
In this article, we report a clinical case of lower gastrointestinal hemorrhage in a 63-year-old female patient, revealing the presence of a secondary duodenal location of a primary lung cancer.
A 63-year-old woman with no smoking history was seen in our emergency department for diffuse abdominal pain, of moderate to severe intensity, accompanied by recurrent episodes of melena.
The history of his disease dates back four months before his admission to our service by the installation of daily episodes of melena associated with alternating diarrhea-constipation, all evolving in a context of deterioration of the general state of asthenia. , anorexia, and weight loss estimated at 18 kgs.
On clinical examination; the abdomen was more painful in the epigastric region without hepatomegaly, splenomegaly, or palpable mass. On pulmonary auscultation; right basal condensation syndrome was also found. Laboratory tests showed iron deficiency anemia (Hb: 3.7 g/dl, TCMH/CCMH), a very high CA 19.9 level at 15,427 U/ml, and a normal ACE level at 8.2 ng/ml. The abdomino-pelvic scanner with an injection of intravenous contrast product found a suspect wall thickening of the third duodenum associated with an infiltration of the mesenteric fat site of lymphadenopathy. A complement by a thoracic scanner was carried out objectifying the presence of
Endoscopy of the upper gastrointestinal tract showed an ulcerated and irregular mass of the second and third duodenum. Pathological analysis (Figure 1) supplemented by an immune histochemical study of duodenal biopsies documented duodenal metastasis from a primary lung adeno carcinoma CK7+, TTF1+ (Figure 2), Napsin A+ (Figure 3). However; the confirmation of primary lung cancer was retained on the anatomo pathological study of the biopsies of the mediastino-pulmonary mass carried out under a bronchoscopy.
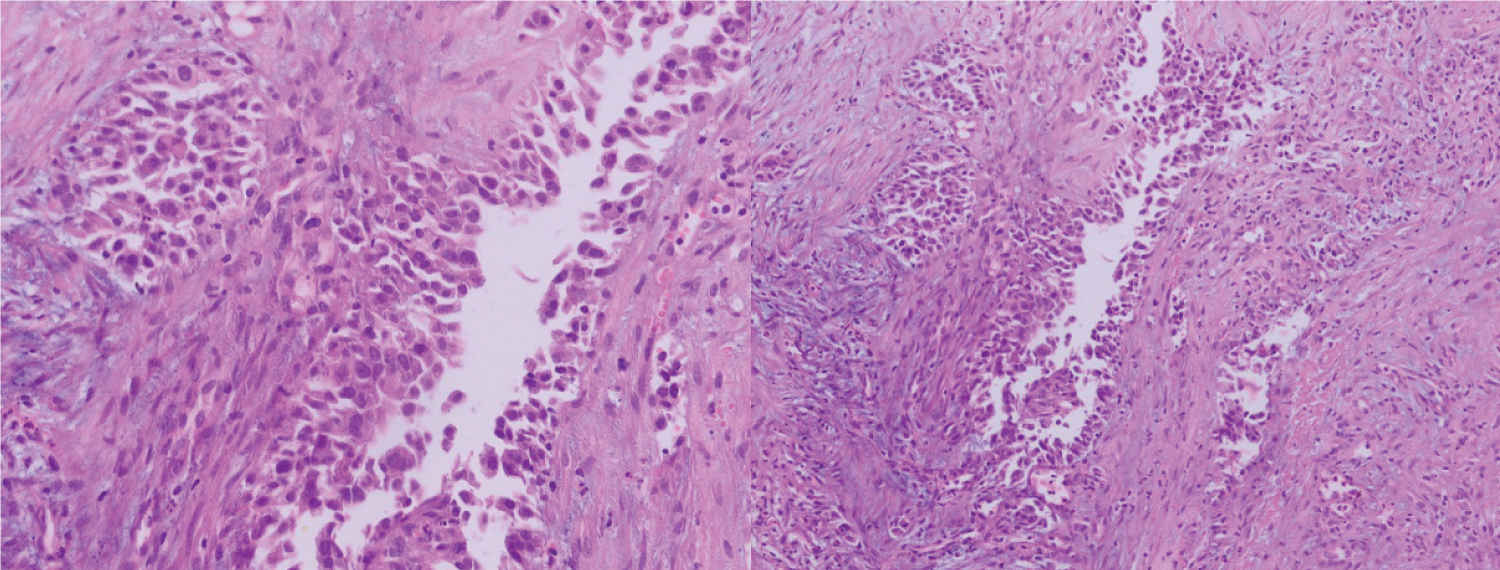 Figure 1: With standard coloration we see sheets of atypical cells with pleomorphic, hyperchromatic nuclei and abundant mitotic figures.
View Figure 1
Figure 1: With standard coloration we see sheets of atypical cells with pleomorphic, hyperchromatic nuclei and abundant mitotic figures.
View Figure 1
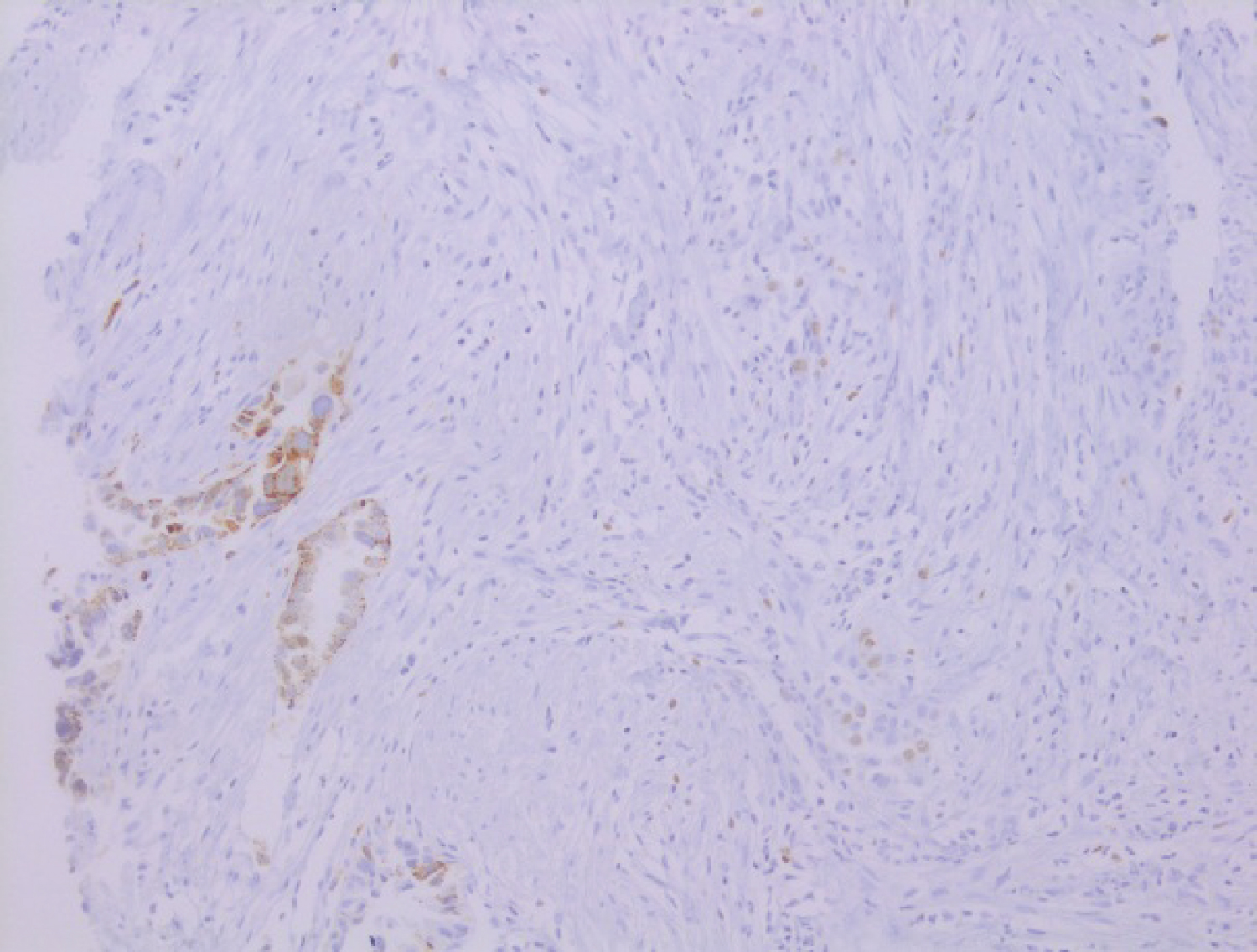 Figure 2: Napsin A +
View Figure 2
Figure 2: Napsin A +
View Figure 2
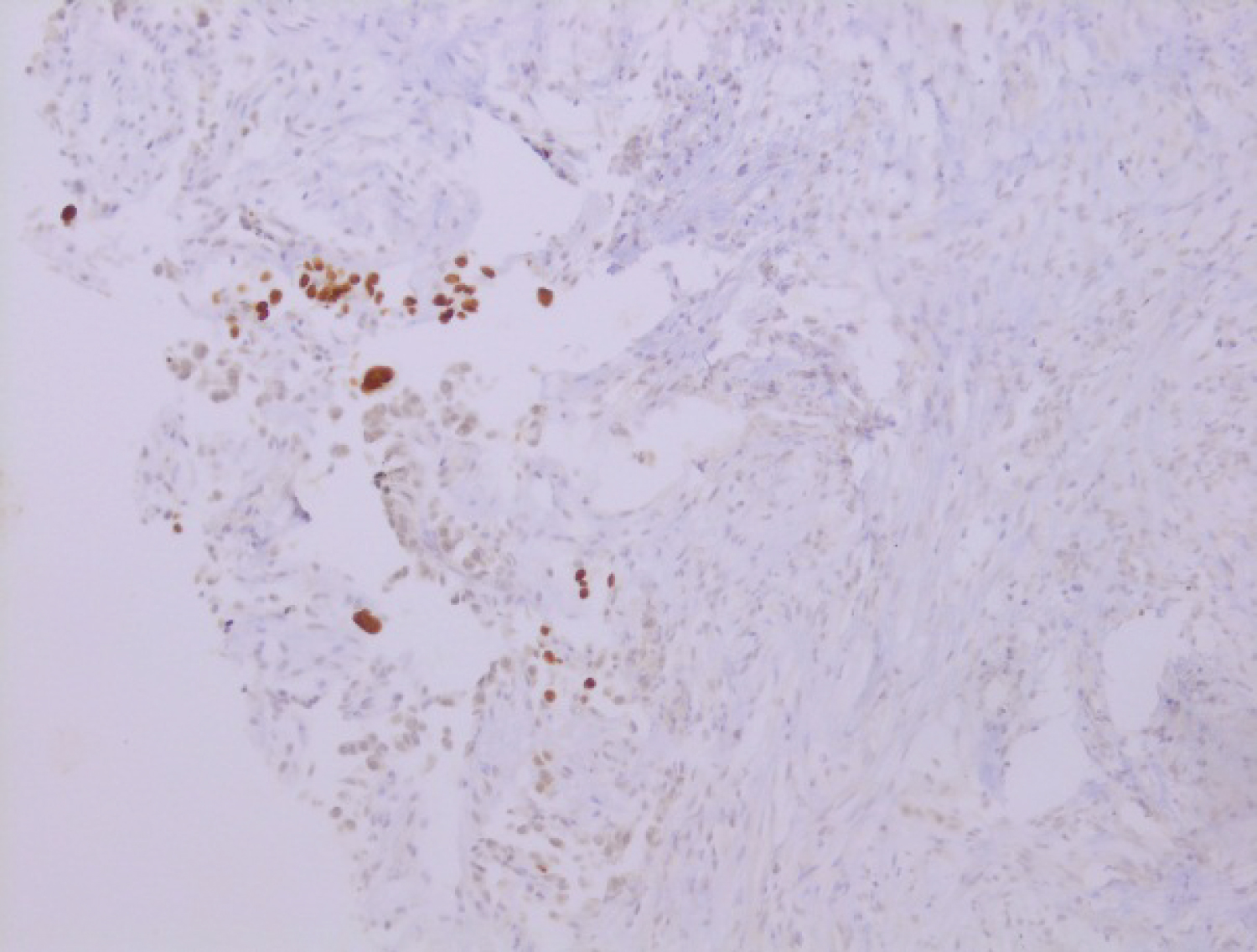 Figure 3: TTF1 +
View Figure 3
Figure 3: TTF1 +
View Figure 3
The patient was generally very impaired with a performance status greater than 2; and his clinical picture was complicated by a mesenteric infarction syndrome which could be confirmed by an angio-CT of the abdomen.
The patient was referred to the palliative care unit for adequate end-of-life support since she is ineligible for specific treatment.
The patient died 7 months after the onset of melena.
Primary lung cancer is the most fatal cancer in the world with a mortality rate varying between 18% and 23% [5,6]. This is due to the late diagnosis of this disease. It has been reported that approximately 50% of cases are diagnosed at the metastatic stage [7].
The incidence of gastrointestinal metastases has been the subject of speculation as it was initially considered extremely rare. However, autopsy studies have found that these secondary lesions may be more common than previously thought.
In the clinical setting, the incidence of symptomatic gastrointestinal metastases from primary lung cancer is 0.3% to 1.7% [2,8]. While in various postmortem studies, these secondary lesions were not really uncommon. According to Antler, et al. [9], Yoshimoto, et al. and Mc Neill, et al. [10] the rate of gastrointestinal metastases is 14%, 11.9% [3] and 16.4% respectively. This comparison between post-mortem cases and clinical cases confirms that gastrointestinal metastases from primary lung cancer are not uncommon as reported in the literature [2]. This clinical underestimation is certainly due to the fact that patients as well as physicians often confuse gastrointestinal discomfort with the side effects of chemotherapy.
Lung cancer metastases can be observed throughout the digestive tract such as the ileum (44%) [11], esophagus (6.3%), small intestine (2.6 %), colon (0.7%) [7], exceptionally the duodenum [12].
In some series; large cell carcinoma was significantly associated with gastrointestinal metastases with an incidence ranging from 30% to 75.9% [3,11]. For this reason, physicians must take this metastatic localization into consideration in the face of any digestive symptomatology.
Abdominal pain is the most common uncomplicated clinical symptom, observed in 50% of cases [13,14]. However, the most common complicated symptom is bowel obstruction [13,15]. Finally, acute digestive hemorrhage can be observed in the form of melena in case of secondary localization in the stomach or duodenum as in our case.
The management of the disease is based on the early discovery of gastrointestinal metastases for an appropriate local treatment before the deterioration of the general condition of the patient since the physical capacity of the patient is one of the factors determining the therapeutic approach.
Patients with intestinal metastases from lung cancer have a very poor prognosis [16]. Median survival does not exceed six months after detection of gastrointestinal metastases according to the largest series published in the literature [7,17,18].
In primary non-small cell lung cancer with metastasis to the gastrointestinal tract, the prognosis is still poor because the majority of cases are diagnosed at a late stage. Therefore, early detection is essential even before clinical symptoms appear; thanks to close monitoring. Thus, these lesions could be investigated and appropriate treatment should be attempted.