In the current study, we report our experience with borderline ovarian tumors. We collected and analyzed retrospective data on the pathology, management, disease free survival (DFS) of patients with borderline ovarian tumors (BOT) who underwent surgical management at or were referred to department of surgical oncology, National Cancer Institute, Cairo University (NCI) from January 2013 to December 2017. This retrospective cohort study included 69 cases. The mean age of our patients at the time of surgery is 41.3 years with 52.17% of them below the age of 40. The most common stage of the disease was stage IA and only two cases developed metastasis. Serous BOT was the most common pathology followed by mucinous BOT. Bilateral tumors were found in 27.5% of cases. The most common surgical complication was ureteric injury. 4 patients underwent fertility sparing surgery via laparoscopy. 10.1% of cases received adjuvant chemotherapy. 50.7% of cases underwent fertility sparing surgery, while radical surgery was performed for 49.3%. Higher recurrence rate was found in the fertility sparing group. All patients who underwent fertility sparing surgery had normal menstrual cycle. Successful pregnancy occurred in 41.1% of patients who desired fertility after surgery. Overall disease-free survival (DFS) was 90.164 months. The most important prognostic factors were disease stage, presence of peritoneal implants and surgical approach. We concluded that borderline ovarian tumors are predominant in young females in the childbearing period. Most cases were diagnosed at stage I. Serous histology was the most common pathological subtype. Surgery either radical or fertility sparing is the main line of management. Some cases may require adjuvant chemotherapy. Recurrence rate was higher in patients who underwent fertility sparing surgery. Disease-free survival was shorter with stages higher than stage I, laparoscopic surgery and presence of peritoneal implants.
Borderline ovarian tumors (BOTs) represent an intermediate category between benign cystadenomas and invasive ovarian carcinomas. They are non-invasive neoplasms that have the capacity for intraperitoneal spread forming invasive implants [1].
Borderline tumors account for 15 percent of all primary ovarian neoplasms. However, in women below 40 years it accounts for 34% of all primary ovarian malignancies [2].
Atypical proliferative neoplasms, tumors of low malignant potential were used to refer to these groups of tumors. Currently, the term (Borderline ovarian tumors) is the most widely used term by oncologists, pathologists and gynecologists and has been adopted into the World Health Organization classification [3].
Among ovarian borderline tumors, approximately 65 to 70 percent have serous histology, and borderline tumors account for an estimated 15 to 20 percent of all ovarian serous neoplasms [4]. Mucinous tumors are the second most common histologic type of borderline ovarian neoplasm; they account for approximately 11 percent of borderline tumors.
At diagnosis, the great majority are stage I [5]. Approximately one-third of women diagnosed with a borderline ovarian tumor are younger than 40 years of age [2]. This makes issues related to ovarian function and fertility preservation of increased importance.
Most patients present with an asymptomatic adnexal mass noted either on bimanual examination or as an incidental finding on sonography. However, symptoms (e.g. abdominal/pelvic pain or dyspareunia) may occur, as with any adnexal mass [6].
The complete staging procedure for ovarian cancer includes: total abdominal hysterectomy and bilateral salpingo-oophorectomy (TAHBSO) with peritoneal washing, cytology of the diaphragm, omentectomy, and resection of grossly visible metastases. The choice of full staging or ovary-conserving surgery is controversial. Approximately one-third of borderline ovarian tumors occur in women younger than 40 years of age, and many young women desire to conserve at least one ovary to preserve fertility and/or avoid the symptoms and effects of premature menopause [4]. The disease has a good prognosis (stage I five-year survival is 99 percent) and unilateral salpingo-oophorectomy (USO) appears to be an option for women with unilateral disease [7].
This retrospective study included all patients with final diagnosis of borderline ovarian tumors (BOT) who underwent surgery at National Cancer Institute - Cairo (NCI) between 2013 and 2017. Patients who were referred to NCI after being diagnosed at other centers for follow up or completion surgery were only included if the pathology review performed at our center confirmed the diagnosis of BOT.
The study included 69 patients. Of those, 41 patients had their primary surgery at our center, while 28 patients were referred from other hospitals after primary surgery. Patients who were lost to follow up within less than one year of primary surgical intervention and those with incomplete medical records were excluded from the analysis. Data were retrieved from patients’ medical records.
The patients were staged following the International Federation of Gynecology and Obstetrics classification (FIGO staging 2009). Institutional review board approval was obtained before data collection.
Statistical analysis was performed using Statistical Package for Social Sciences (SPSS) version 23.Comparisons between two groups for normally distributed numeric variables were done using the Student’s t-test while for non-normally distributed numeric variables, comparisons were done using Mann-Whitney test. Chi square or Fisher’s tests were used to compare between the groups with respect to categorical data, as appropriate. Kaplan-Meier method was used to estimate recurrence free survival. Predictor and prognostic variables were related to survival using log rank test. All tests were two-sided. P-values < 0.05 was considered significant.
Disease-free survival (DFS) was defined as the time from the date of primary surgery to the detection of recurrence or the latest observation. Overall survival (OS) was defined as the time from the date of primary surgery to death or the latest observation.
The mean age of included patients at the time of diagnosis was 41.3 ± 17.00 years; 36 of these patients (52.17%) were younger than 40-years-old. The youngest and oldest patients were aged 14 and 69 years, respectively (Table 1).
Table 1: Demographics and preoperative data. View Table 1
The majority of the patients (64 patients) had stage I disease at diagnosis (92.7%). Only one patient had stage II disease (1.2%), while 3 patients were diagnosed at stage III (3.4%). Only one case was diagnosed as stage IV (1.2%). Bilateral synchronous tumors were present in 19 cases (27.5%) (Figure 1).
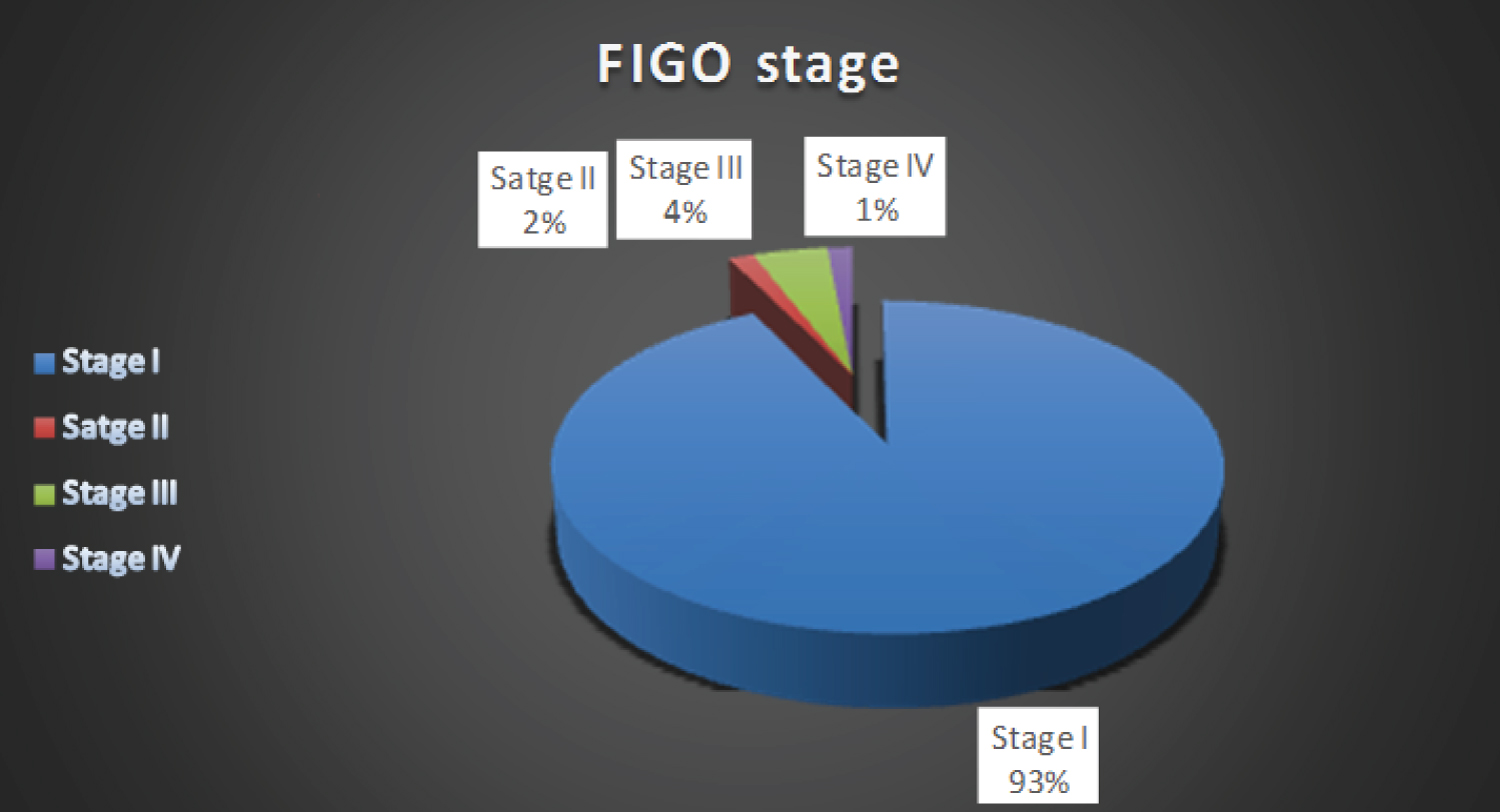 Figure 1: FIGO stage percentages.
View Figure 1
Figure 1: FIGO stage percentages.
View Figure 1
The size of the tumor was estimated using the maximum tumor diameter in centimeters according to the final pathology report. The mean maximum tumor diameter for the involved patients was 16.6 ± 8.2 cm.
The most common histological subtype was the serous subtype. It was found in 39 patients out of a total of 69 patients included in the study (56.5%). The mucinous histology was found in 22 patients (31.9%) representing the second most common subtype. Other less common subtypes included endometroid, sero-mucinous and transitional cell type (Brenner's tumor).
On reviewing surgical pathology reports, it was found that 43 patients had papillary projections inside the tumor (62.3%), while 8 patients had micro invasive foci representing 11.6%.
All the 69 cases underwent surgery; 65 of them through laparotomy and 4 through laparoscopic approach.
Considering patient age, disease stage and the desire of the patient to preserve fertility, Conservative (Fertility-sparing) surgery was performed in 35 patients (50.7%) with preservation of the uterus and at least one ovary, while radical surgery was performed in 34 patients (49.3%) in the form of TAH-BSO.
Moreover, analyzing the type of surgical procedure, about half of our patients underwent total abdominal hysterectomy with bilateral salpingo-oophorectomy (TAH-BSO) as a radical procedure. The rest of the patients underwent fertility sparing procedures including unilateral salpingo-oophorectomy (USO), unilateral cystectomy, bilateral cystectomy, USO with contralateral ovarian cystectomy. The most commonly performed fertility sparing procedure was unilateral salpingo-oophorectomy representing 24.6% of all procedures.
Regarding staging status, 8 patients (11.6%) underwent complete staging including peritoneal washing and/or biopsies, pelvic and para aortic sampling/lymphadenectomy and omentectomy. 22 patients (31.9%) underwent incomplete staging while 39 patients (56.5%) underwent only ovarian surgery without staging.
Peritoneal implants were identified in 6 cases (8.7%), they were all biopsied and they were pathologically proven to be positive in 5 cases.
Omentectomy was performed for 27 patients representing 39.1% of the total number of cases in our study. Of these 27 patients, only 3 had histologically proven omental deposits.
Appendectomy was performed as part of the staging procedure for 6 cases. None of them had appendiceal involvement.
Pelvic lymphadenectomy or sampling was done in 8 cases only as part of the staging procedure. The median number of lymph nodes removed was 3 ranging from 2 to 18 lymph nodes.
Frozen section examination was performed in 3 cases (4.3%) and in two of them it was suggestive of borderline tumor. In the third case, the frozen section assessment was inconclusive (Table 2).
Table 2: Operative & pathological characteristics. View Table 2
Intra-operative and postoperative complications were encountered in 9 patients representing 13% of cases. The most common complication was ureteric injury (33.3% of all complications). Other complications included bladder injury, intra-operative severe hemorrhage, burst abdomen, tubo-ovarian abscess and port site tumor implantation. Only one case died because of a surgical complication few days after the surgery due to massive intra-operative hemorrhage.
5 cases had a residual tumor after the primary surgical intervention (7.2%). Four out of those five cases were referred to our center for further management after the primary surgery. The management was in the form of completion surgery for three cases and chemotherapy for the fourth case. One case underwent the primary surgery in our center and had a residual because the procedure was aborted due to massive intra-operative hemorrhage. Unfortunately, the patient died few days later in the surgical ICU.
Seven cases received adjuvant chemotherapy (stage Ic and above) representing 10.1%. The chemotherapeutic regimen was Taxol-Carboplatin for all of them for 3 to 9 cycles.
Local recurrence occurred in 14 cases representing 20.3% of all cases. Surgical management was performed for all the local recurrences except for one case who lost follow up after the diagnosis of recurrence.
Surgery was performed for 13 cases with local recurrence. 7 recurrences had a borderline pathology which is similar to the original pathology (53.8%). However, 6 cases (46.2%) had a recurrence in the form of invasive carcinoma.
Only two patients developed metastatic disease (2.9%). In both case, Lung was the site of metastasis.
We next analyzed the patients by dividing them in to two age groups according to the median age (< 40 vs. ≥ 40) (Table 3). All parameters were comparable between the two groups except for the type of surgery performed. For patients below the age of 40 years, 31 out of 36 cases had conservative surgery (86.1%), while only 5 cases had radical surgery.
Table 3: Characteristics of patients based on age group. View Table 3
On the other hand, radical surgery was done for 29 out of 33 patients aged 40-years-old or above (87.9%). Four cases (12.1%) of this age group underwent conservative surgery.
The results of the multivariate analyses of DFS and OS are shown in Table 4. The overall median disease-free survival (DFS) for all patients was 90.164 months.
Table 4: OS, DFS and the relation between different factors and DFS. View Table 4
Significant prognostic factors that had an impact on DFS were as follows:
FIGO stage at diagnosis: Median DFS for stage 1 patients was 90.164 months, while this was 5.033 months for higher stages at diagnosis (P value = 0.016).
FIGO stage at diagnosis: Median DFS for stage 1 patients was 90.164 months, while this was 5.033 months for higher stages at diagnosis (P value = 0.016).
Peritoneal implants: Patients who had peritoneal implants detected during surgery (whether invasive or not) had shorter DFS (9.243 months) compared to those who didn't have peritoneal implants (90.164 months). P value = 0.001.
Factors that didn't prove to affect DFS include patient's age, type of surgery, staging status, histological type of the tumor, presence of micro invasion and omental deposits.
BOTs are classified as a separate entity within ovarian malignancies because of their atypical properties. They represent about 15% of ovarian malignancies.
About one-third of women diagnosed with a borderline ovarian tumor are younger than 40 years [2]. The mean age of our patients at the time of surgery was 41.3 years with 52.17% of them below the age of 40.
The CA 125 tumor marker does not appear to be useful in the detection of a borderline ovarian tumor. Almost half of all patients have a normal CA 125 level [8]. In our study, 46 patients had their blood tested for CA 125 level before surgery. The marker was normal in 30.4% of cases (about one third).
The majority of cases are diagnosed at stage I. As an example, in one literature review including 948 cases, Tinelli, et al. found that 70 percent presented as stage I, 10 percent presented as stage II, 19 percent presented as stage III, and less than 1 percent presented as stage IV [9]. In our study, the majority of patients (64 patients) had stage I disease at diagnosis (92.7%). Only one patient had stage 2 disease at diagnosis (1.2%), while 3 patients were diagnosed at stage 3 (3.4%). Only one case developed metastatic disease (1.2%).
Serous borderline neoplasms are the most common histologic subtype representing approximately 65 percent of borderline ovarian neoplasms [10]. Mucinous tumors are the second most common histologic type; they account for approximately 11 percent of borderline tumors [5]. In our study, the most common histological subtype was the serous subtype. It was found in 39 patients out of a total of 69 patients included in the study (56.5%). The mucinous histology was found in 22 patients (31.9%) representing the second most common subtype. Other less common subtypes included endometroid, sero-mucinous and transitional cell type (Brenner's tumor).
For patients with peritoneal implants, those with invasive implants appear to have a higher relapse rate (> 50%) [11]. In our study, peritoneal implants were identified in 6 cases (8.7%), they were all biopsied and they were pathologically proven to be positive in 5 cases. Patients who had peritoneal implants detected during surgery (whether invasive or not) had shorter DFS (9.243 months) compared to those who didn't have peritoneal implants (90.164 months).
On reviewing surgical pathology reports, it was found that 43 patients had papillary projections inside or on the surface of the tumor (62.3%), while 8 patients had microinvasive foci representing 11.6%.
Frozen section is commonly performed intraoperatively in suspected BOTs and the information is used to help determine the extent of the surgical procedure. A meta-analysis of 18 studies on the diagnostic accuracy of frozen section results of ovarian pathology found generally good sensitivity (65 to 100 percent) and excellent specificity (> 99 percent) when compared with the final histologic diagnosis [12].
In our study, frozen section examination was performed in 3 cases only (4.3%) and in two of them it was suggestive of a borderline tumor. In the third case, the frozen section assessment was inconclusive.
The overall risk of recurrence after conservative surgery for BOTs ranges from 7 to 30 percent [7], while recurrence risk after radical surgery is about 6%. Recurrences typically show borderline histology, not invasive carcinoma [13]. In our study, local recurrence occurred in 14 cases representing 20.3% of all cases. Surgery was performed for 13 cases with local recurrence since one case lost follow up after diagnosis of recurrence. 7 recurrences had a borderline pathology which is similar to the original pathology (53.8%). However, 6 cases (46.2%) had a recurrence in the form of invasive carcinoma.
Statistical analysis of our patients showed that local recurrence rate was higher in patients who underwent fertility sparing surgery than those who underwent radical surgery (31.4%. for fertility sparing surgery Vs. 8.8% for radical surgery).
Laparoscopic approach is feasible and safe for management of borderline ovarian tumors. However, cyst rupture was more likely and complete staging is less likely with laparoscopic surgery than laparotomy, but there is no difference in recurrence rate [14]. In our study, only 4 patients were managed laparoscopically representing 5.8%. All of them underwent fertility sparing surgery. 3 of those patients developed local recurrence. Hence, recurrence rate after laparoscopic surgery was 75%. On the other hand, local recurrence in 11 cases out of 65 patients who under went open surgery representing 16.9%. However, if a larger number of patients were managed laparoscopically, this would have provided a better sample size and more valid results.
In our study, bilateral synchronous tumors were present in 19 cases (27.5%), while 50 cases had a unilateral tumor (72.5%).
Oophorectomy on one side and cystectomy on the other is the usual treatment approach for bilateral BOTs. However, some studies suggest that an ultra-conservative approach using bilateral cystectomy was found to be effective and had better fertility outcomes [15].
In view of the relatively common involvement of both ovaries at the same time, we believe that thorough pre-operative radiological evaluation and careful intra-operative examination of the other ovary to exclude synchronous contralateral tumor is crucial before performing a conservative procedure.
In our study, intra-operative and postoperative complications were encountered in 9 patients representing 13% of cases. The most common complication was ureteric injury (33.3% of all complications). Other complications included bladder injury, intra-operative severe hemorrhage, burst abdomen, tubo-ovarian abscess and port site tumor implantation. These complications were not fatal except for one case who died because few days after the surgery due to massive intra-operative hemorrhage.
Intra-operative identification of ureters is key to prevent injury. Safe specimen extraction after laparoscopic surgery is very important to prevent port site implantation.
Omental biopsy or omentectomy is recommended as part of staging procedure for BOTs [16]. In our study, omentectomy was performed in 27 patients and pathological examination revealed metastatic deposits in 3 of them. Patients with positive omental deposits had a shorter DFS (5.003 months) but the difference was not statistically significant.
Some studies recommend performing appendectomy for mucinous tumors [16]. However, appendectomy was performed for 6 cases in our study and none of them had appendiceal involvement. We agree with the literature advocating appendectomy for mucinous tumors to exclude occult primary appendiceal neoplasm with ovarian metastasis.
Lymph node involvement has low prognostic value in cases of borderline ovarian tumors. As a result, pelvic lymphadenectomy is not routinely recommended [17]. In our study, pelvic lymph node sampling or dissection was performed in 8 patients. Specimen examination revealed negative lymph nodes in all of them. Thus, we recommend pelvic lymph node sampling only if suspected nodal involvement is suspected intra-operatively.
In our study, 5 cases had a residual tumor after the primary surgical intervention (7.2%). Four out of those five cases were referred to our center for further management after the primary surgery which was in the form of completion surgery for three cases and chemotherapy for the fourth case. One case underwent the primary surgery in our center and had residual because the procedure was aborted due to massive intra-operative hemorrhage. Unfortunately, the patient died few days later in the surgical ICU. We recommend surgery as a first line management of residual disease following primary surgery.
Adjuvant chemotherapy is recommended for BOTs if invasive peritoneal implants are present. The recommended regimen is intravenous carboplatin with either docetaxel or paclitaxel (the same regimens used with low grade serous ovarian carcinoma). In our study, 7 cases received adjuvant chemotherapy in the form of Taxol-Carboplatin. All cases with stage 1c or higher received adjuvant treatment.
Serous borderline tumors recurrences are usually of borderline pathology or low-grade serous carcinoma. In rare cases, a serous borderline tumor may recur as a high-grade serous carcinoma [16]. Recurrent mucinous BOT sare usually related to an incompletely resected mucinous border line tumor and does not include an invasive component. Surgery is the main line of treatment for recurrent BOTs [18]. In our study, 14 cases developed local recurrence. 13 of them underwent surgery as a management for the recurrence. All recurrences were managed via open approach except for one case who underwent laparoscopic ovarian cystectomy.
On pathology review of recurrent cases, 7 cases had a borderline pathology and 6 cases had an invasive recurrence.
Borderline ovarian tumors are predominant in young females in the childbearing period. Most cases were diagnosed at stage I. Serous histology was the most common pathological subtype. Surgery either radical or fertility sparing is the main line of management. Some cases may require adjuvant chemotherapy. Recurrence rate was higher in patients who underwent fertility sparing surgery. Disease-free survival was shorter with stages higher than stage I, laparoscopic surgery and presence of peritoneal implants.