Leiomyosarcoma is a rare lesion and its localization to the vagina extremely rare. We report two cases of primary leiomyasarcoma of the vagina, involving the posterior wall, in a 46-year-old woman and a 56-year-old woman, describing their histomorphological and evolutionary characteristics, with review of the literature.
Leiomyosarcoma, Vagina, Histopathology
The female genital tract can be the site of malignant tumors at different levels, mainly in the cervix and the endometrium. The vagina is rarely involved, accounting for only 1-2% of cancers of the entire female genital tract [1], and sarcomas are equally rare, constituting only 2% of malignant tumors of the vagina although the dominant type is leiomyosarcoma [2]. Although cases of primary leiomyosarcoma of the vagina are rare, they have been reported in the world literature [3,4] and even in Africa [5,6]. In the Congo, no case has been documented, and we report two cases of primary leiomyosarcoma of the vagina, one of which is recurrent and metastatic, and the other of incidental discovery on histopathological study, and review the literature.
It concerned a 46-year-old female patient who presented with a perineal-vaginal mass. This mass was located on the posterior wall (Figure 1) and had been evolving for two years. She had undergone multiple consultations in peripheral hospitals and medical offices in the city of Brazzaville under circumstances that are not well understood. However, she reported that the mass had been removed on two occasions, without any anatomical-pathological analysis on each occasion, and that it had recurred on both occasions. The recurrence of the mass for a third time was the reason for her consultation at the gynecology department of the Brazzaville University Hospital. No lesions in the uterus were noted throughout the investigations. An excision of the mass was again performed, and the specimen was sent to the Anatomy and Cytology Pathology laboratory, in 3 nodular, well-limited fragments, measuring respectively cm, 2 cm and 5 cm in long axis. These fragments were of firm and elastic consistency. On section, the slices were super imposable, whitish, fleshy, and fasciculated. Hemorrhagic remodeling was noted. On microscopic examination, the tumor was a malignant sarcomatous proliferation, with obvious smooth muscle differentiation, made of spindle-shaped cells, arranged in intersecting bundles, with marked cyto-nuclear atypia, and showing nuclear pleomorphism, associated with significant mitotic activity. Note the presence of areas of hemorrhagic suffusion and necrotic changes (Figure 2). The diagnosis of a conventional high grade primary leiomyosarcoma was retained. The evolution was marked by the evolutionary resumption of the mass, complicated by genitourinary fistula, then very quickly it progressed to a poly metastatic state, notably to the lung and liver. A chemotherapy treatment was proposed in oncology after a multidisciplinary consultation meeting, according to the AI protocol (Adriamycin and Ifosfamide) in first line, without success. The patient died 8 months after the diagnosis was made in a picture that is not elucidated to us.
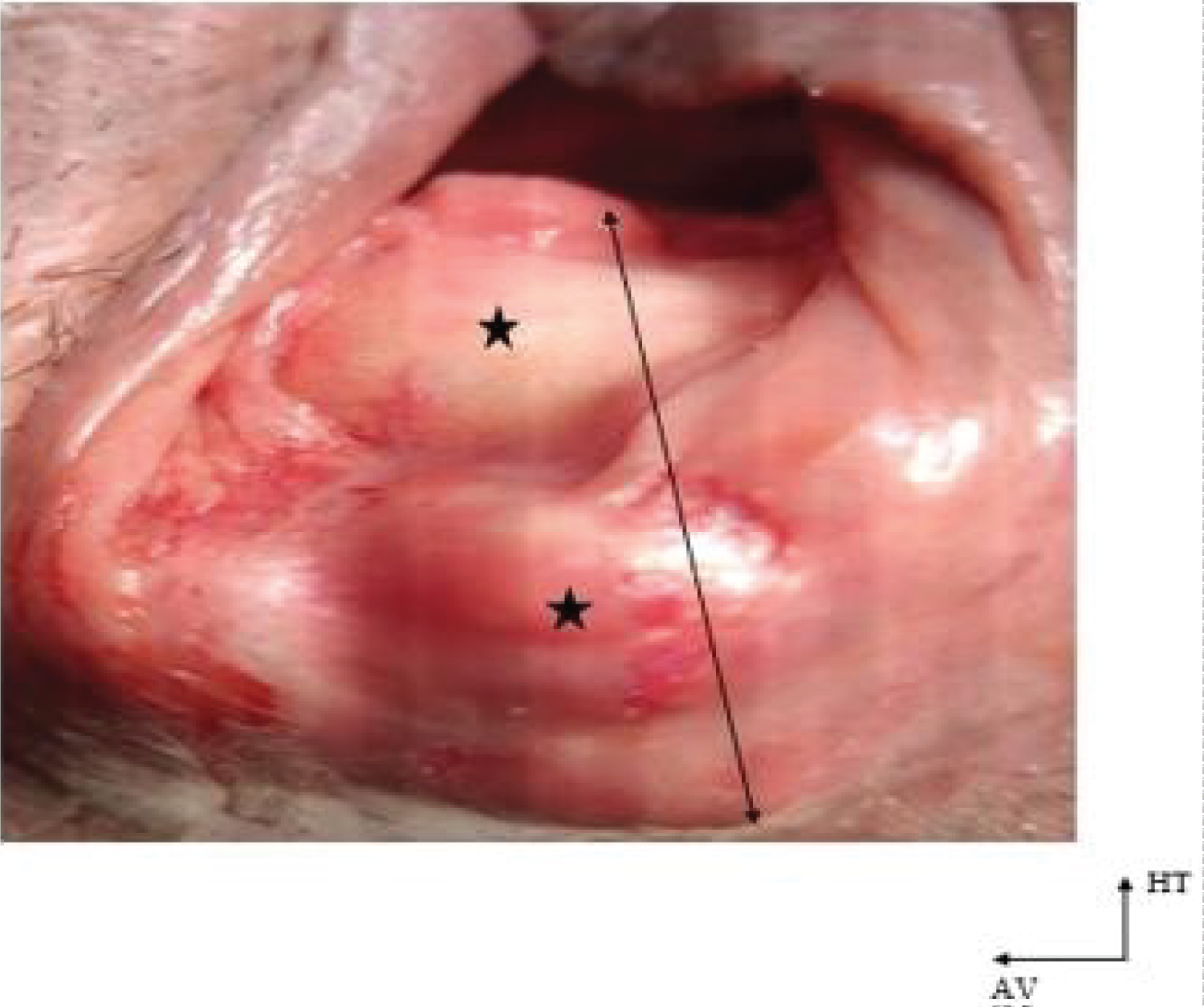 Figure 1: Macroscopic illustration of case N°1
Figure 1: Macroscopic illustration of case N°1
A bilobed nodular mass (★) is seen, occupying the whole posterior wall of the vagina (arrow), bleeding slightly on contact.
View Figure 1
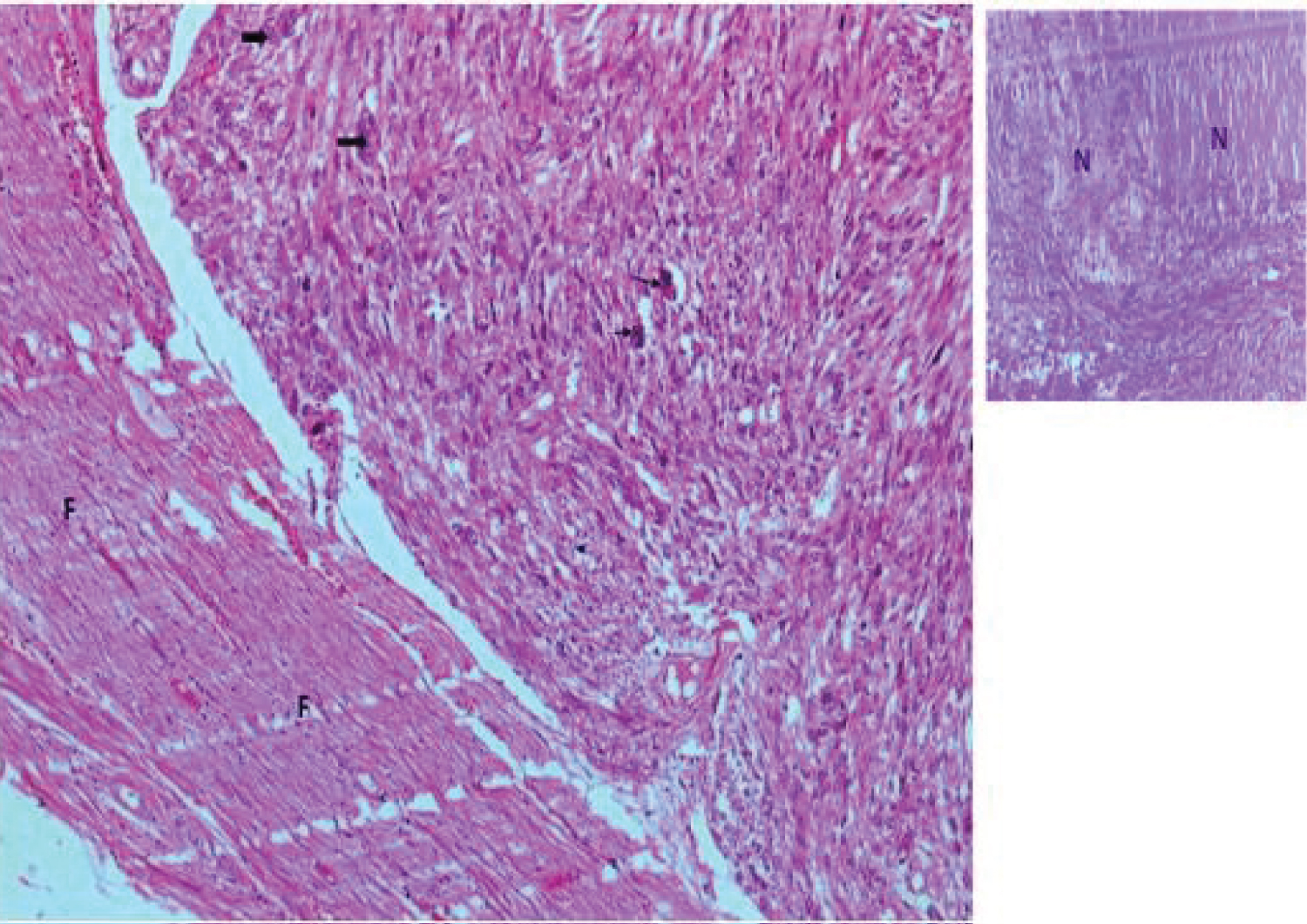 Figure 2: Histological illustration of case 1 (HEx10)
Figure 2: Histological illustration of case 1 (HEx10)
A sarcomatous tumor proliferation is observed, made of leiomyocytes sometimes showing marked cytonuclear atypia (large black arrow), and abnormal mitoses (small black arrow).The tumor appears well limited and circumscribed by a band of fibrous tissue (F). Note on some fields areas of necrosis (N).
View Figure 2
It concerned a 56-year-old female patient, followed in a private clinic in Brazzaville for a nodular mass, well limited, evolving for 6 months. It was a mass located at the posterior wall of the vagina, clinically benign, which justified an excision. This exeresis was performed and the material was sent to the laboratory of Anatomy and Cytology Pathology in two fragments of 2.5 and 4 cm, well circumscribed, with whitish, fleshy fasciculated slices of section. On microscopy, it was fortuitously a malignant sarcomatous tumor proliferation with smooth muscle differentiation also evident, consisting of atypical leiomyocytes with quite high mitotic activity, organized in intersecting bundles (Figure 3). Areas of tumor necrosis should be noted. The evolution remains to be monitored after concerted therapeutic decision. The result was made available.
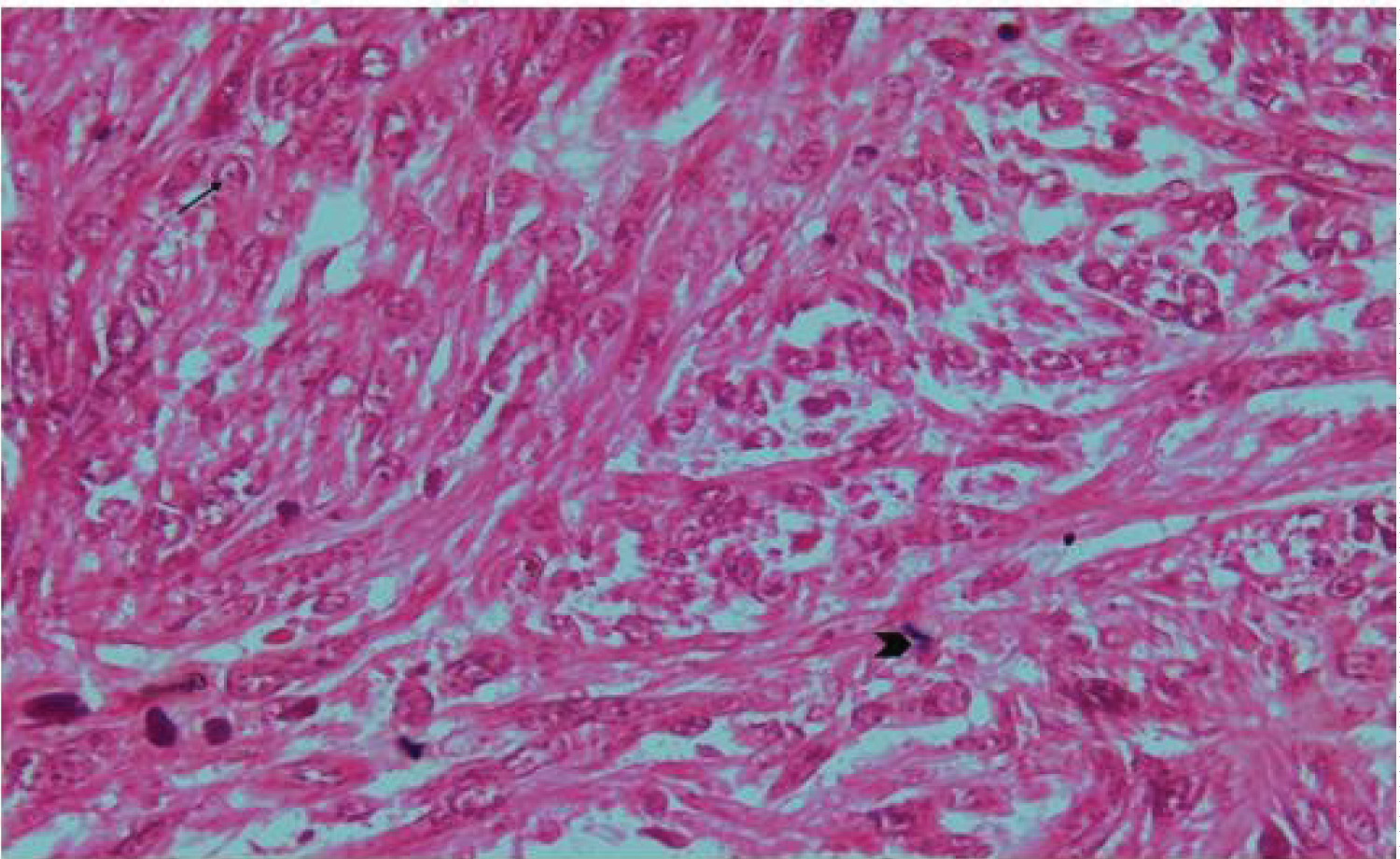 Figure 3: Histological illustration of cases 2 (HEx20).
Figure 3: Histological illustration of cases 2 (HEx20).
We see a tumor proliferation made of spindle-shaped cells, arranged in bundles, with atypical nuclei sometimes nucleolated (black arrow). Note the presence of mitotic figure (>).
View Figure 3
Leiomyosarcoma is a malignant mesenchymal tumor developed at the expense of smooth muscle. As such, its preferential location in the genital tract is the uterine body, particularly in the myometrium because of its histological structure composed essentially of smooth muscle, where it represents 1.3% of all cancers and 40 to 50% of sarcomas [7]. The average age is often between 45 and 55 years [8]. It is both a rare and aggressive tumor with high recurrence rates, and an often unfavourable prognosis even if it is confined or well circumscribed [9]. It is often diagnosed incidentally and correct diagnosis is hampered by equivocal features similar to those of the much more common benign uterine fibroids, and therefore the seriousness of the situation is often not quickly appreciated [9]. Hence the need for an anatomical-pathological study of samples, even if they appear to be purely leiomyomatous, in order to make a diagnosis as early as possible, and at a distance from a metastic state, which in the event of a malignant lesion is often frequent [10]. If the uterine body, as indicated above, is the preferred site, cases of vaginal localization have been reported in the literature [3,11], including multi-recurrent cases [4,10], with the same histological and evolutionary characteristics as their counterparts of uterine localization described above.
The cases we report involved this location, i.e., the vagina, at its posterior wall in a 46-year-old and a 56-year-old lady, corresponding to the average age according to the literature, i.e., between 45 and 55 years [8]. The microscopic semiology was typical and the diagnosis was made based on two main microscopic elements, namely smooth muscle type differentiation and nuclear pleomorphism, although an immune histochemical study if performed, through smooth muscle tissue markers such as Actin smooth muscle (AML), or caldesmone, would have been of an equally decisive contribution. Moreover, the presence of mitotic activity and tumor necrosis constituted a histological argument of tumor aggressiveness.
The first case was also remarkable for its multi-recurrence character, corroborating the data in the literature concerning the evolutionary description of this lesion [11]. It was also metastatic in the months following the diagnosis with a death occurring in the same year (8 months later). The evolution towards a metastatic state validates the aggressive character of this lesion as reported in the literature and the occurrence of death in the same year also validates the thesis of its poor prognosis, given that the 5-year survival of leiomyosarcoma is estimated between 25 and 40% and death occurs on average 8 months after the appearance of the first symptom [12]. This fatal evolution can be explained both by factors related to the lesion, in particular its aggressive character which led very quickly to a metastatic stage, and by factors related to the patient, in connection with his psycho-affective state and a possible lack of therapeutic compliance in spite of chemotherapy.
The second case was of fortuitous discovery since clinically the aspect appeared rather benign. This fortuitous if not accidental discovery is also reported in the literature, where it is pointed out the equivocal character similar to that of benign fibroids [9]. Although the diagnosis was made early in a patient supposed to be in a non-metastatic state, tumor necrosis and a rather important mitotic activity were found, which suggest an aggressive character of the tumor and thus an unfavourable evolution if an adequate treatment is not rapidly undertaken in order to improve the survival of this patient.
We have reported here two cases of a rare lesion, leiomyosarcoma, in an equally rare location, the vagina. It was a very aggressive and devastating lesion, which in its evolution can be multi-recurrent and poly-metastatic, punctuated also with other complications such as a recto- genital fistula. Moreover, although these are only two cases, it is a demonstration and an interpellation on the indispensable character of the anatomopathological study of any exeresis even if the benignity of the lesion seems clinically evident, in order not to make lose a chance of prolongation of survival to a patient.
We can also foresee through these two cases a wider study on sarcomas of the vagina in general, by integrating immune histochemical and molecular aspects.