Pulmonary colloid adenocarcinomas are uncommon tumors individualized as a distinct entity in the histological classification of World Health Organisation of lung tumors characterized by extensive pool of extracellular mucin distending and destroying alveolar walls. We herein report a case of a 63 year-old active man smoker who presented with a worsening dyspnea. A chest computed tomography scan showed a highly suspected irregular nodule of 23 mm in the left-upper lobe. The patient underwent a left-upper lobectomy. Gross examination showed a tan-white cystic nodule measuring 2 cm in greatest dimension filled with gelatinous materiel and microscopic examination revealed an invasive adenocarcinoma with pool of extracellular mucin distending alveolar spaces and destructing their walls. Immunohistochemically, the tumors cells showed diffuse staining for CK7, CDX2, MUC2, MUC5 and focal staining for CK20 and TTF-1. These findings were consistent with the diagnosis of primary pulmonary colloid adenocarcinoma.
Colloid, Adenocarcinoma, Lung, Immunohistochemistry
The 5th edition of World Health Organisation of lung neoplasm has individualized colloid adenocarcinoma as rare entity among invasive pulmonary adenocarcinomas with distinct clinicopathological and histopathological features [1]. It was previously called with a plethora of different names: Mucinous cystadenoma [2,3] mucinous cystic tumor [3,4] adenocarcinoma arising in a mucinous cystadenoma [2,4,5] pulmonary mucinous cystic tumors of borderline malignancy [6] and mucinous cystadenocarcinoma [3].
This tumor account for less than 0.24% of all primary lung carcinomas [6] and constitute a challenge for the pathologist who must rule out other differential diagnosis. Immunohistochemistry plays a major role for both diagnostic and prognosis.
A 63-year-old man, an active smoker 50-pack-year with a history of chronic obstructive lung disease presented with one year worsening dyspnea. Chest X-ray showed opacity of left upper lobe. Bronchoscopic findings were unremarkable. Lung function testing registered obstructive ventilator defect. Chest computed tomography scan showed a highly suspected perifissural nodule of 23 mm in the left-upper lobe. The nodule was irregular with spiculated contours and a central necrosis (Figure 1). The patient underwent a left-upper lobectomy. Gross examination showed a tan-white cystic nodule measuring 2 cm in greatest dimension filled with gelatinous materiel on the cut surface. Microscopic examination revealed an invasive tumor arranged in acinis and papillary structures which are dissected by pool of extracellular mucin distending alveolar spaces and destructing their walls (Figure 2). They were covered by a pseudostratified columnar epithelium consisted of well-differentiated tall mucinous columnar cells with mild to moderate cytologic atypia (Figure 3). The fibro-inflammatory stroma contains multiple multinucleated giant cells phagocyting the mucin. Immunohistochemically, the tumors cells showed diffuse positive staining for CK7, CDX2, MUC2, MUC5 and focal staining for CK20 and TTF-1. These findings were consistent with the diagnosis of primary pulmonary colloid adenocarcinoma. The patient had an uneventful postoperative course. The patient is asymptomatic for two years after the operation.
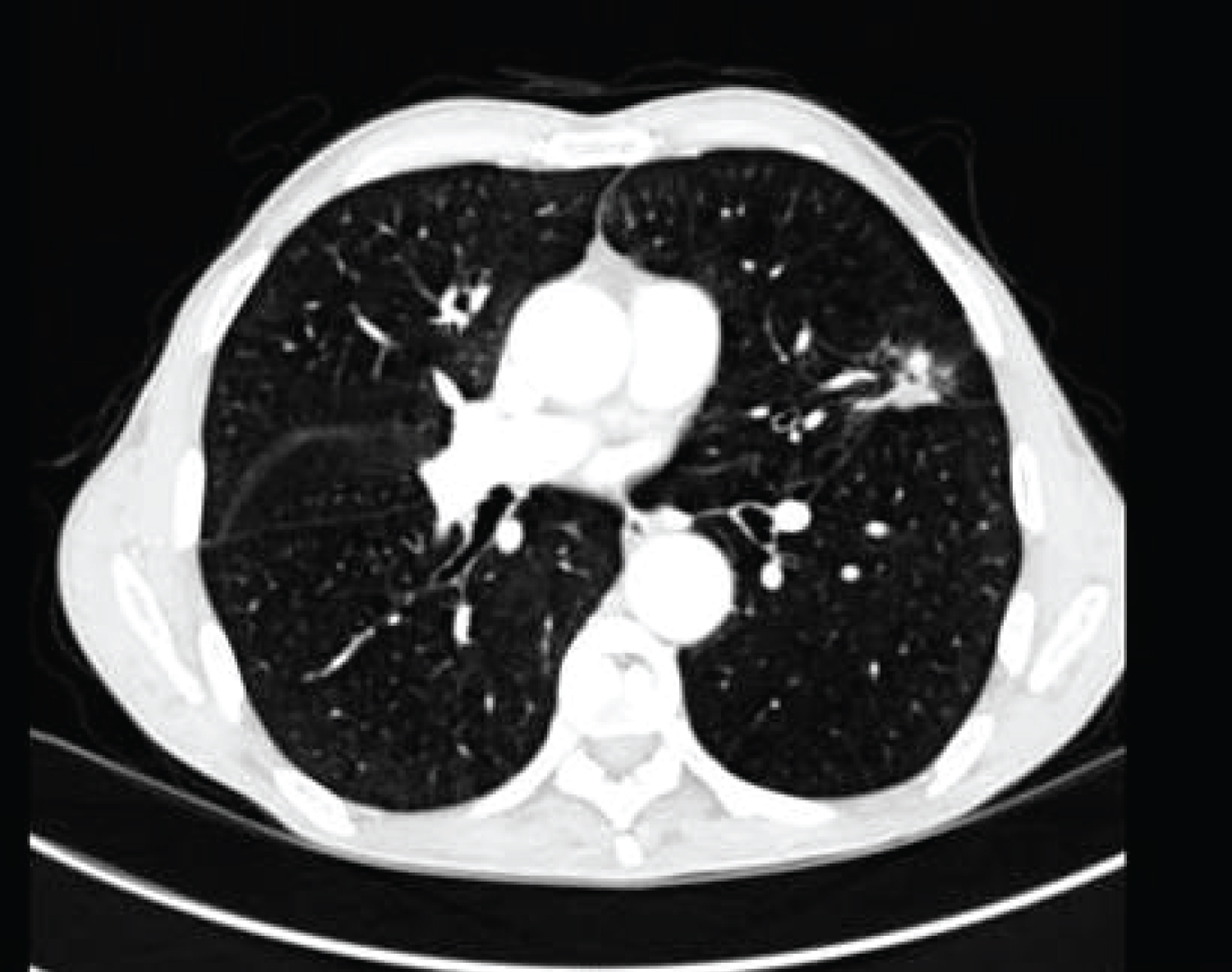 Figure 1: Chest computed tomography showing an irregular speculated mass in the left-upper lobe.
View Figure 1
Figure 1: Chest computed tomography showing an irregular speculated mass in the left-upper lobe.
View Figure 1
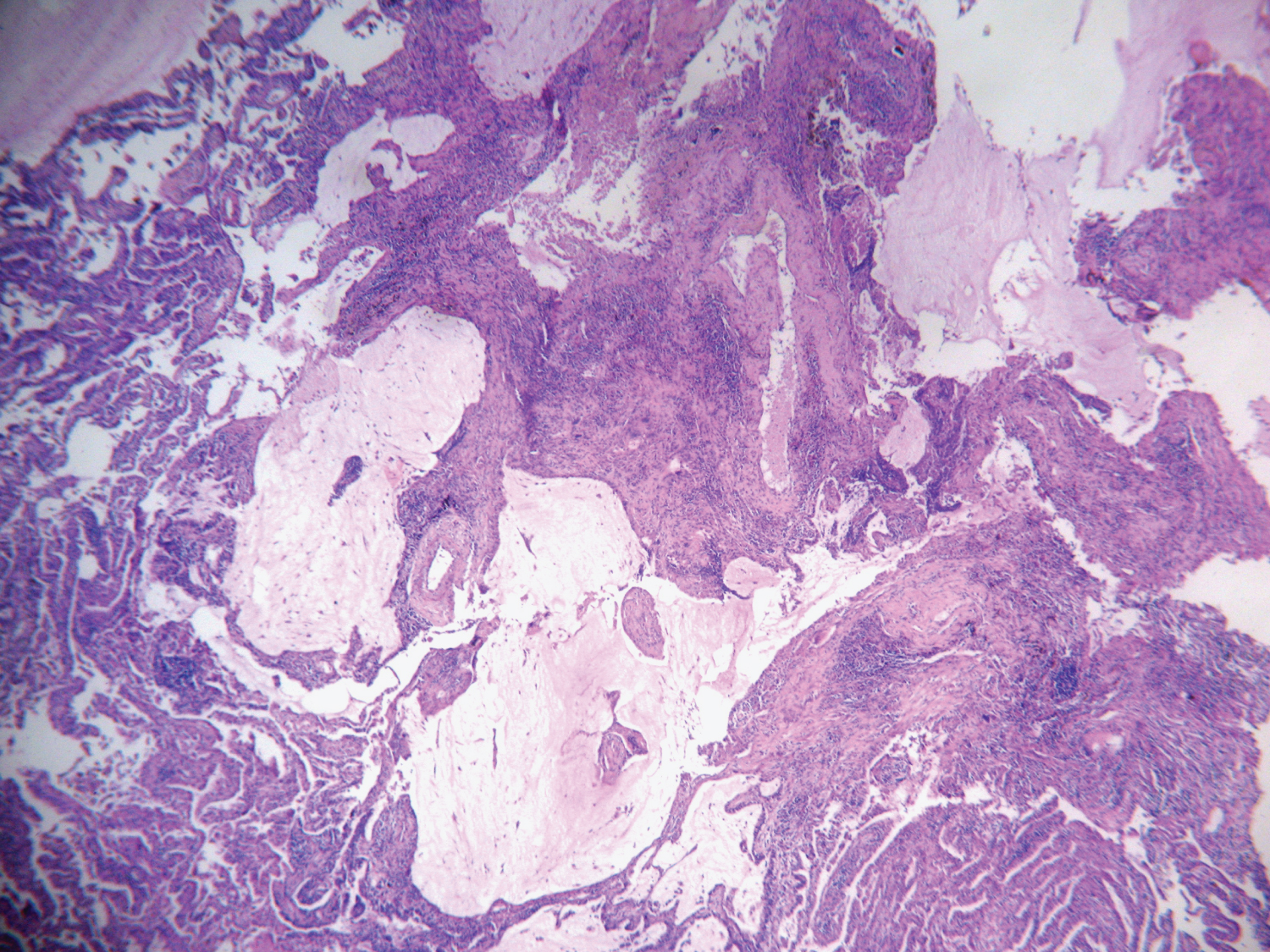 Figure 2: Tumor is arranged in acinis and papillary structures which are dissected by pool of extracellular mucin distending alveolar spaces and destructing their walls.
View Figure 2
Figure 2: Tumor is arranged in acinis and papillary structures which are dissected by pool of extracellular mucin distending alveolar spaces and destructing their walls.
View Figure 2
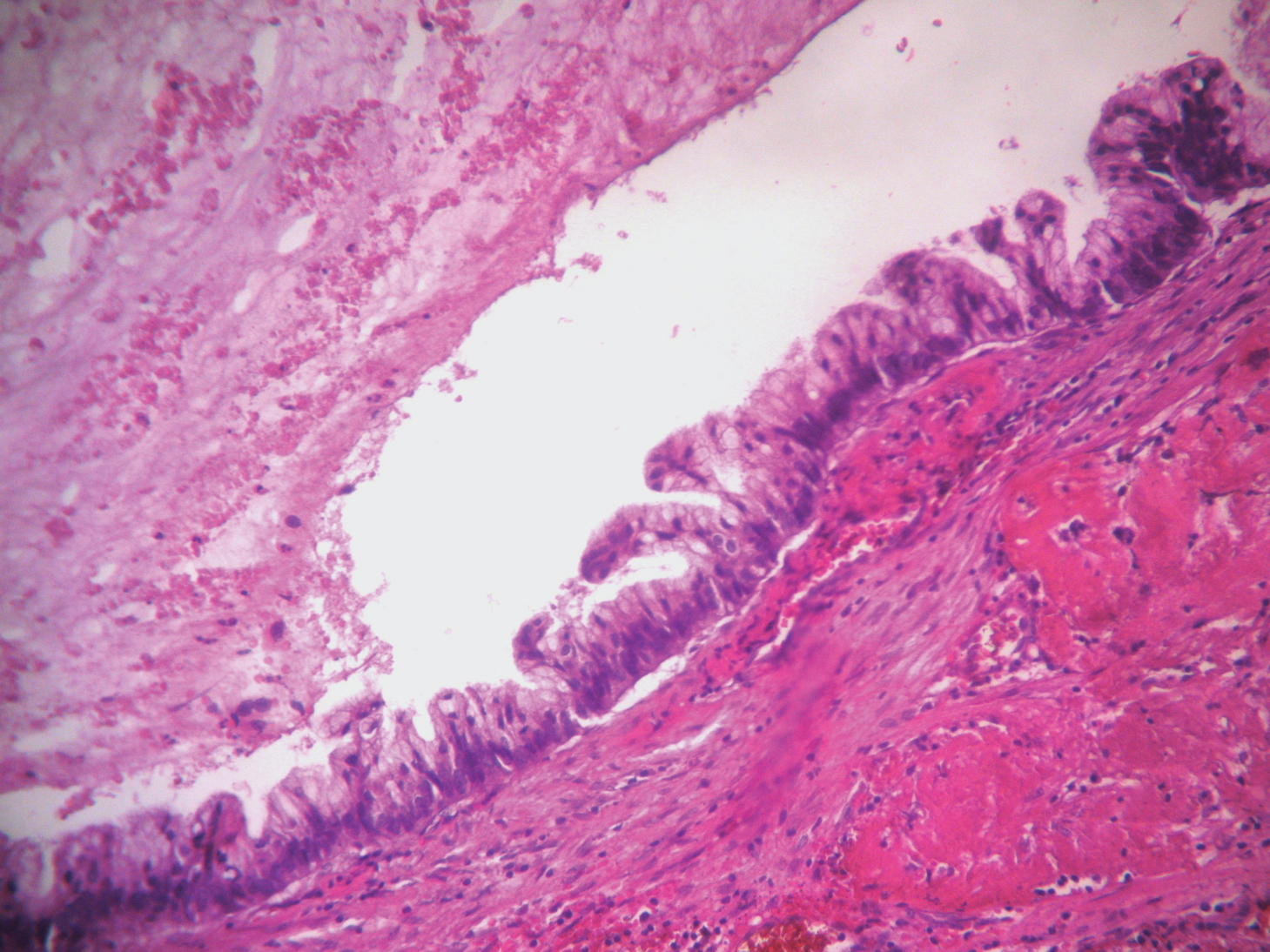 Figure 3: The acinis are lined by a pseudo stratified columnar epithelium consisted of well-differentiated tall mucinous columnar cells with mild to moderate cytologic atypia.
View Figure 3
Figure 3: The acinis are lined by a pseudo stratified columnar epithelium consisted of well-differentiated tall mucinous columnar cells with mild to moderate cytologic atypia.
View Figure 3
The first case of colloid adenocarcinoma was reported by Graemes cook, et al. in 1991 [6], since 76 cases were reported in the literature. There were 41 women and 35 men with extreme ages between 35 and 86 years and a mean of 63.7 [2,4-16]. Most of patients were asymptomatic with the lesion incidently discovered on chest X-ray [8,11]. The other presented with respiratory symptoms as cough, chest pain or dyspnea [11]. Mostly patients were active smokers [2,5,8,9,13,14,11,12,15]. Radiologically, the tumour presented typically as a solitary peripheral well-defined, partly lobulated, homogeneous and low attenuated lesion with focal mural or septal enhancement on computed Tomography [2,14]. Macroscopically, colloid adenocarcinoma presented as a solitary peripheral variably circumscribed, unencapsulated nodule with a soft gelatinous well-demarcated with uni to multilocular formation and cystic change may be observed. Tumor size ranges between 1.4-15 cm with mean of 6.5 cm [1,2,6,8-15].
Histologically, colloid adenocarcinoma is characterized by the presence of large lakes of extracellular mucin filling the alveolar spaces and destroying their walls, showing an overtly invasive growth pattern into the alveolar spaces. [1]. The tumor cells consist of foci of cuboidal to tall columnar cells with globlet-like features growing in lepidic fashion. Tumor gland may float into the mucoid materiel. Epithelial pseudostratification of nuclei may be observed with minimal nuclear atypia and the mitotic rate is low. Inflammatory infiltrate with histiocytes and giant cell reaction to mucin may be observed [1,9,17,18]. Colloid adecnocarcinoma is rarely mixed with other adenocarcinoma subtypes, more than 50% of the tumor should have colloid pattern to establish the diagnosis of colloid adenocarcinoma [1].
The most important differential diagnoses of colloid adenocarcinoma are mucinous metastatic adenocarcinomas from the gastrointestinal tract, breast, ovary and pancreas. The clinical context and the expression of CK7, CDX2, Muc2 and weak and focal expression of CK20 and TTF-1 on immunohistochemical study raise the diagnosis of primary pulmonary colloid adenocarcinoma [1,8-10,16]. It is reported that the prognosis is better in patient with CDX2/MUC2 positive expression than in those with CDX2/MUC2 negative expression [8]. In the present case, the patient is an active smoker man who presented with a solitary nodule of 2 cm. On immunohisochesmistry tumor cells expressed CDX2, MUC2 and MUC5.
Colloid adenocarcinoma are considered as a tumor with low-grade malignancy [10] with relatively favorable prognosis after complete surgical resection [1]. Few authors underwent wedge resection with careful surveillance since it was an incidental discovery. The presence of signet-ring cells and a non colloid component signifies worse prognosis with reccurence and metastasis [1].
We presented a unique case of colloid adenocarcinoma which is a rare neoplasm that can be discovered incidentally or may be symptomatic. It is considered as low-grade tumors that can recur locally and might have distant metastasis. Pathologists should consider this entity and rule out secondary metastasis from the gastrointestinal tract and discern it with invasive mucinous adenocarcinomas using a panel of antibodies including CK7, CK20, CDX2, TTF-1, MUC2 and MUC5.