Most childhood ailments often present with fever which account for the most common reasons why parents seek medical care for their children; particularly, the under-five children. The study aimed to assess the mothers' knowledge of fever in their under-five children and how this is managed at home.
This was a descriptive designed study that used a simple random sampling technique to select 100 participants who were mothers of under-five children who presented to the Kwahu Government Hospital, Atibie over a period of six months. A structured questionnaire comprising of close-ended questions were used to collect data. Both secondary and primary data were collected and analyzed. The primary data was analyzed using SPSS version 16.0.
The mothers described fever as hotness of body (63%), shivering (10%), child crying (8%), child being quiet (8%) and sleeping too often (10%). More than half of the respondents (57%) correctly identified the cause of fever as malaria (39%) and infections (18%). Home management of fever involved self-medications (43%), consulting herbalist (20%) as well as tepid sponging (28%) and visiting nearby hospital (62%). Mothers knowledge of childhood fever was statistically significantly associated with their age (p = 0.0001), age of the child (p = 0.04), number of children in a family (p = 0.0001), and level of education of the mothers (p = 0.0001).
Mothers described hotness of the body as fever and knew that malaria and infections causes fever among children. They consulted herbalist among other inappropriate practices in the management of fever.
Childhood fever, Knowledge, Management, Mothers, Children under five
Most childhood ailments often present with fever which account for the most common reasons why parents seek medical care for their children [1]. In the first two years of life, children generally experience between four to six febrile episodes each year [2]. Fever is a common sign of self-limiting viral infections; however they may signify serious illnesses in less than 10% of cases and bacterial infections in approximately 4% [3]. The incidence of fever as the major complaint for consultation is reported to be 122 per thousand children up to 1-year-old, and 415 per 1000 children from 1 to 5-years-old in the Netherlands [4]. Studies from the USA reported that about 30% of children seen by paediatricians in practice were as a result of fever [5].
In Africa, higher incidence of fever has been recorded in the rural part of Senegal with 20% of children getting fever every month. In Mali, prevalence of fever for a day was 6.2% in dry season and 12.8% in rainy season while in rural parts of Guinea the prevalence of fever was 23% in under-five children and in Kenya it was 6% [6]. Fever accounts for over 60% of pediatric outpatients' visits in Ghana and other Sub‐Saharan African countries [7].
Huda, et al. [8], indicated that mothers usually recognize fever by the general appearance of the child and they also determine how to treat fever in their children with self-medication [9,10]. According to Stagnara, et al. [11], most parents repeatedly treat fever in their children by self-medication before seeking the opinion of a physician. Fever is potentially harmful if inappropriately managed and it has been reported to have some potentially harmful effects if not well managed [12]. Parents need consistent evidence-based information about childhood fever management [13] which can be achieved through education about fever and improving access to primary care [14].
At The Kwahu Government Hospital at Atibie, 1034 cases of childhood fever were reported between 2014 and 2016, of which 31-43% febrile convulsion [15]. Febrile convulsion is the most common childhood fever in under five children and is one of the causes of pediatric hospital admissions in Ghana [16]. The study aimed to assess mothers' knowledge of fever and its management in under-five children in Atibie, Ghana.
A descriptive study design was adopted employing a quantitative approach. The study was carried out at The Kwahu Government Hospital. The hospital is one of two district hospitals in the Kwahu ridge area. It serves an estimated population of about 230,000 people from over 200 Communities within the district.
The data collection tool used in this study was self-designed questionnaire. A structured questionnaire comprising of close-ended questions and designed using the English Language were used to collect data. The questionnaire was divided into three sections where information was gathered on the demographics of the child and their mothers, mothers' knowledge of fever, and home management of fever. Questions related to the demographics were open-ended. For close-ended questions there were pre-determined responses for the participants to pick from. A pre-test of the questionnaires was conducted at The Kumasi South Hospital which has the same characteristics like study site. The Cronbach's Alpha test was used to measure the internal consistency of the instruments. For this study the scores obtained were 0.81 for mothers' knowledge of fever and 87 for home management of fever. The instruments were therefore deemed reliable and it was further evaluated to correct grammatical errors and typographical errors.
Data was collected within a period of 6 months (November 2016 to April 2017) which increased the possibility of having varied answers and 4 research assistants were included in data collection. A pretesting was done with a sample of the respondents before the actual administration of the questionnaires to minimize bias in the study. Questionnaires were administered to respondents by the researchers and their assistants. The questions were read out to the mothers and the interviewers entered the responses into the questionnaire. The questionnaire was also read in any other language respondents preferred and could easily understand.
The sample size was calculated using Yamane [17] formula. For this study, 90% confidence level and precision of 10% (P = 0.10) were used.
Equation;
Where n is the sample size, N is the population size, and e is the level of precision. An average of 20,000 women with children under five years report to the facility with fever annually. Therefore, this formula was applied to achieve the sample for the study.
N = 20,000
n = 100
In selecting the sample, a simple random sampling technique was applied. This method selected by chance or none zero selection of mothers of children under five years. The number of mothers with under five children who visited the facility were counted each day and based on the numbers for the day, random numbers from a prepared random number table was assigned to them. After that, 5 random numbers were selected each day of data collection within six (6) months till the sample size was attained.
The data was analyzed using SPSS version 16.0 and presented using both descriptive and inferential statistics displayed in frequency bar graphs and tables. The use of mean, standard deviation, frequency and percentages constituted the descriptive aspects of the statistics employed for the analysis of data. Mean, standard deviation, frequency and percentages were used in describing the demographic data. Chi-square tests were used to assess association between Age of mother, Age of child, Marital status, Number of children, Level of Education, Number of children under five years and knowledge of fever.
A verbal informed consent was sought before administration of the questionnaire. Verbal consent was taken from respondents because a good number of them could not read or write. The process was approved by the ethics committee after explaining why such approach was used. Approval was sought from the administrators of the hospital before the facility was used and also ethical clearance was obtained from the committee on Human Research Publications and Ethics (CHRPE) of the Kwame Nkrumah University of Science and Technology before the study was carried out.
Table 1 shows Characteristics of the study sample and majority of the mothers were 19-24 years old (56%), married (54%), and had only one child (84%). Majority of the children were 3-4 years old (60%). The mean age of the mothers was 31.36 ± 7.97 years, while the mean age for the children was 2.08 ± 1.12 years.
Table 1: Characteristics of the study sample. View Table 1
Description of fever by mothers as shown in Figure 1 suggests that most mothers (63%) described hotness of the body of a child as fever. Others described it as shivering (10%) as well as quietness of baby (8%), baby crying (8%) and baby sleeps often (10%).
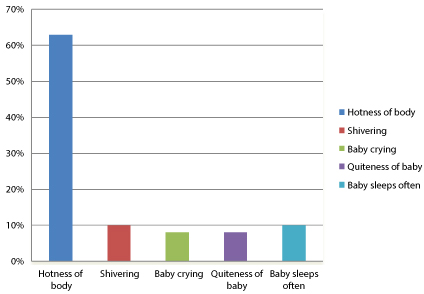 Figure 1: Description of fever.
View Figure 1
Figure 1: Description of fever.
View Figure 1
Respondents shared their views on what causes fever as displayed in Figure 2. From their responses, some said it is caused by infections (18%) but most of the mothers (39%) were of the opinion that fever was cause by malaria. Others also mentioned overeating (6%) as well as evil spirits (11%).
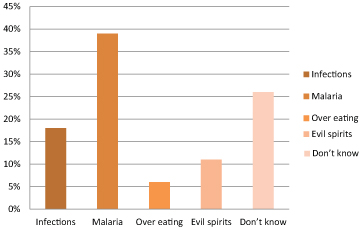 Figure 2: Causes of fever.
View Figure 2
Figure 2: Causes of fever.
View Figure 2
From the Table 2, the level of mother's knowledge about fever differed significantly with demographic characteristics such as Age of mother (p = 0.0001), Age of child (p = 0.04), Number of children (p = 0.0001) and Level of Education (p = 0.0001).
Table 2: Mothers demographic characteristics and knowledge of fever. View Table 2
Figure 3 shows mothers fever management practices. From the figure, visiting nearby clinic/hospital, tepid sponging as well as giving children medication when they had fever were some of the frequently used fever management practices among mothers.
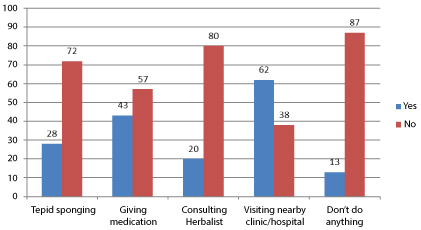 Figure 3: Fever management practices.
View Figure 3
Figure 3: Fever management practices.
View Figure 3
Figure 4 displays Medications for treating fever among mothers. The figure shows that more than half of the respondents had administered herbs (65%), paracetamol (71%) and chloroquine (62%) as medication to manage fever.
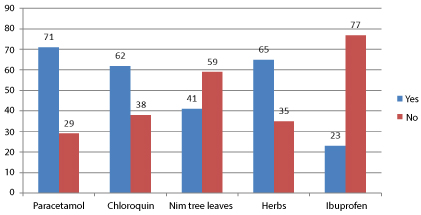 Figure 4: Medications for treating fever.
View Figure 4
Figure 4: Medications for treating fever.
View Figure 4
This study examined the knowledge and management of fever among mothers with children under five years. The study assessed the mother's knowledge on fever, the causes of fever and various management practices. The findings revealed that, more than half of the mothers described fever as hotness of the body. This indicates that hotness of the body was usually attributed to fever in the study location. This supports the findings of Oshikoya and Senbanjo [7] who reported that most of the mothers (83.3%) perceived fever as the hotness of the whole body of the patient.
A proportion of the respondents of this study were of the view that fever is caused by overeating (6%) as well as evil spirits (11%). This suggests that there are several misconceptions about the causes of fever. Similarly, Taveras, et al. [14] reported that Latino parents were more likely to believe that certain Latino folk illnesses (mal de ojo, empacho (indigestion or GI malaise) and mollera caida) causes fever. Mal de ojo occurs when a person with "strong eyes'' intentionally or unintentionally looks at a child while Mollera caida or fallen fontanelle is believed to occur when the breast or bottle is removed too rapidly from an infant's mouth or when the infant is bounced or tossed around. The misconceptions about the causes of fever may be attributed to socio-cultural believes.
In another study, Huda, et al. [8] reported that majority of respondents (81.6%) believed that teething causes fever in children. However, we observed that most of our respondents (39%) identified malaria as the commonest cause of fever in children.
The age of mother, age of child, number of children and level of education were found to be significantly associated with mothers' knowledge of fever. The significant association of mothers' knowledge of fever and their level of education corroborates other studies from different populations [18-22].
In our study, the proportion of mothers who will administer medication for fever in their children was 43%. This was far lower than the 88% reported in Australia and even far lower than the 94% reported in France [11,13]. The percentage gap in the medication use may be due to their location and access to drugs and to some extent their knowledge in other methods of managing the condition. A number of the respondents in the study reported that fever was caused by spirits. It is likely that these people may focus management on dealing with the spirit behind the sickness. Regarding use of medications to treat fever, antipyretics such as paracetamol and Ibuprofen were used. Health professionals frequently recommend treatment regimens for children with fever that either combine or alternate paracetamol and ibuprofen [23,24]. However, the consequences of under- and over-treatment with antipyretics including mucosal lesions, gastrointestinal discomfort such as dyspepsia, and severe gastrointestinal complications such as perforated ulcer, gastrointestinal bleeding has been reported [25].
Furthermore, the findings that Paracetamol and chloroquine were also medications used by some of the mothers to manage fever is consistent with other studies who found most mothers managing fever with paracetamol [11,26]. This indicates that these medications are the easiest to access either through over the counter drug sellers or the environment. Ibuprofen was mentioned by a small number of respondents. However, in the study of Stagnara, et al. [11], ibuprofen was one of the medications mentioned most often by respondents for managing fever.
Also, more than half of the respondents had applied herbal concoctions to treat fever in their children. Herbs have potentially unexpected effects such as toxicity [27]. An interaction may involve having the herb component to cause an increase/decrease in the amount of drug in the blood stream [28,29]. The high rate of the use of herbal concoctions may be due to the fact that the study was conducted in a peri-urban area where most mothers are not highly educated, poor and may not have access to health facilities as compared to those in the larger cities.
It is appropriate to present a febrile child to the hospital or a physician, 62% of the respondent's in this study presented a febrile child to the hospital/clinic. A higher proportion of mothers (85.7%) in a study on knowledge and management of fever among Moroccan parents consulted the general practitioner or paediatrician when fever persisted [30]. The reason behind the number of people visiting hospital or a physician when their child had fever may probably be due to the preference for expert management.
The study made use of 100 respondents from the study area based on the sampling formula and framework selected. Only those mothers who already had access to health care were sampled. Those without access may have less fever knowledge and be at greater risk for adverse outcomes. A larger proportion of respondents may provide the kind of information that is representative of the actual situation. Also, the illiteracy level in the study area made it difficult to recruit respondents for the study since most of them were not used to participating in such studies and did not know its relevance.
In this descriptive study, mothers described hotness of the body as fever and perceived malaria as the major cause of fever among children. The fever management practices frequently utilised by the mothers included tepid sponging, applying herbal concoction as well as giving children medication and visiting the hospital/clinic. Most of the mothers administered herbs, paracetamol and chloroquine as medication to manage fever. The age of mother, age of child, number of children and level of education were found to be significantly associated with mothers' knowledge of fever. Based on the findings, it is recommended that The Ministry of health should intensify education on childhood fever and channel it through the print, community information centres and electronic media to inform mothers on issues related to causes, early and late signs and management of fever. Parents should also be educated on the effect of fever, especially if not managed on time; highlighting the importance of early management that has to do with fever. Public Health nurses should intensify campaigns on fever to eliminate the negative religious-cultural perceptions and believes mothers attached to fever and its causes.
The conception and design as well as data collection of the study were taken care of by the first, second and third authors (R. Anokye, R. Amihere and PA) The secondary data compilation and review of the literature was done by the first author. The fourth author (AE) read the entire manuscript and improved the write-up. All the authors contributed to the data analysis, design and preparation of the manuscript. All authors read and approved the final manuscript and have all agreed to its submission for publication.
We wish to express our profound gratitude to the staff of the School of Nursing, Garden City University College as well as staff and management of The Kwahu Government Hospital and all mothers who participated in this study. We further wish to thank all who have contributed to knowledge in the area of fever among children as well.