Background: Varicella Zoster Virus (VZV) is a ubiquitous virus and is causing both diseases of varicella and herpes zoster. VZV reactivation may lead to neurological complications, including transverse myelitis. However, transverse myelitis caused by VZV reactivation is rare in immunocompetent patients.
Case presentation: We reported a case of transverse myelitis caused by VZV in an immunocompetent young patient. A 42-year-old man was presented to the Neurology department in June 2019 with the complaints of cutaneous rash, lower limbs weakness and anal and urinary incontinence. The neurological manifestations occurred at twelve days after cutaneous rash. Spine MRI showed extensive intramedullary T2 hypersignal of C6 to C7. White blood cell showed hyperleucocytosis. Cerebrospinal fluid (CSF) showed leukocytosis (40 cells/µL) with increased levels of protein (1.134 g/l). CSF culture for bacteria and fungi were negative. The patient was treated with oral acyclovir, corticotherapy and functional rehabilitation. Complete recovery occurred after 4 weeks of treatment.
Conclusions: Transverse VZV myelitis in an adult immunocompetent patient following cutaneous rash is extremely rare in our context. Clinical outcome was favorable after recommended dose of acyclovir, corticotherapy and rehabilitation.
Myelitis, Varicella-Zona virus, Immunocompetent, Burkina Faso
VZV: Varicella Zoster Virus; MRI: Magnetic Resonance Imaging; DNA: Deoxyribonucleic Acid; PCR: Polymerase Chain Reaction; CSF: Cerebrospinal Fluid; MADRS: Montgomery Asberg Depression Rating Scale; HIV: Human Immunodeficiency Virus; IgG: Immunoglobulin G; CD4: CD4 T Lymphocytes
Varicella Zoster Virus (VZV) is a ubiquitous virus and causes both diseases of varicella (primary infection) and herpes zoster (reactivation) occur commonly throughout the world [1]. Varicella is highly contagious; it is most commonly seen in children under the age of 10 years in countries where live-attenuated varicella vaccine is not routinely administered [2]. Adults and immunocompromised patients are more prone to severe infections than healthy children [3]. VZV induced neurological complications are reported as 0.1-0.75% [4]. Among them, cerebellar ataxia and encephalitis are seen frequently while transverse myelitis, Guillain-Barre syndrome, meningoencephalitis are rarely observed [5]. However, transverse myelitis is one of the rarest complications, particularly in immunocompetent patients [6,7]. The frequency of transverse myelitis during or after varicella infection is 0.3% [8]. The most reported complications due to varicella infection in the Middle East were Central Nervous System (CNS) involvements followed by skin diseases, varicella pneumonia, and gastric diseases [9,10]. Previous studies in African setting, notably in Sudan [11], Burkina Faso [12] and Guinea [13] had reported few cases of myelitis, meningoencephalitis and stroke as neurological complications of VZV. In this study, we describe a rare case of transverse myelitis caused by VZV to emphasize the possibility of its occurrence in an immunocompetent subject.
A 42-year-old man was presented to Neurology department of Yalgado Ouedrago University Hospital in June 2019 with the complaints of cutaneous rash, lower limbs weakness and anal and urinary incontinence of 17 days duration. He had sudden onset of generalized pruritus with vesicular eruption disseminated throughout his face, extremities and trunk, but sparing the palms of hands, soles of the feet. The bursting of the vesicles was associated with a high fever 39 °C. Fifteen days later, he felt muscular weakness of the two lower limbs, a decrease in the sensitivity of the lower limbs going back to the thorax and a urinary and anal incontinence. The patient had no known previous history of chickenpox and had never a chickenpox vaccination. Additionally, his wife and daughter developed chicken pox, 2 weeks before disease onset. On admission, the patient had a body temperature at 37.7 °C, a blood pressure at 120/60 mmHg with a heart rate of 90 beats per minute and a respiratory rate of 19 cycles per minute. His weight has been estimated at 60 kg. He was fully conscious, oriented; fundi were normal and cranial nerves intact. Upper limbs were normal. Neurological examination revealed severe weakness of the lower limbs (medical research council (MRC) grade 0/5). Ankle and knee jerk reflexes were abolished bilaterally, without Babinski sign. Furthermore, decreased sensation to touch was noticed with T7 sensitive level bilaterally. Vibration, temperature and pinprick sensations were also diminished in lower limbs. There were no signs of meningitis and cerebellar involvement. Dermatologically, there were macular scarred lesions, hyper pigmented, with a hyperpigmented peripheral halo of rounded shape. These lesions vary in size from 2 to 6 mm, well limited with a regular border, with a smooth surface, sometimes isolated, sometimes grouped in a cupboard scattered over all the integuments (Figure 1). Elsewhere, the lymph nodes were free and there were no sphincter disorders. Cervical MRI showing extensive intramedullary T2 hypersignal of C6 to C7. There was no enhancement on T1 after gadolinium injection and Fat saturation. The remainder of T2 hyper signals is related to a truncation artifact. The spine MRI was considered normal (Figure 2 and Figure 3). A clinical diagnosis of transverse myelitis was made. Cerebrospinal fluid (CSF) was clear, colorless and showed leukocytosis (40 cells/uL), increased levels of protein (1.134 g/l) and normal glucose at 2.3 mmol/l (random blood sugar 4.55 mmol/l). CSF culture for bacteria and fungi were negative. The VZV PCR in the LCR could not be performed. The hemogram showed a hemoglobin level at 12.7 g/dl, white blood cells at 7830/mm3 and a platelet level at 362000/ml and a C-reactive protein at 44.81 mg/l. Renal function tests, liver function tests and urinalysis were all normal. He was negative on HIV testing with CD4 count at 1643 cells/mm3. The varicella etiology was finally retained. Methylprednisolone intravenously 120 mg per day during three days was started 5 days after admission and continued with prednisolone tablets 60 mg per day during 20 days. Oral acyclovir 1000 mg per day during 20 days was started 7 days after admission. Functional rehabilitation was associated during hospitalization stay and after one month. During hospitalized period of 40-day, the patient developed a systemic infection with Escherichia coli on admission day 15 and depressive symptoms on admission day 33 with sadness of mood, suicidal thoughts, anorexia and insomnia. This depression was moderated with a MADRS score rated 20/60. At discharge, the patient presented with apyrexia, spastic paraparesis rated 4/5 and disappearance of depressive symptoms. Complete recovery occurred in 4 weeks of treatment.
 Figure 1: Macula scarred lesions hyperpigmented on the trunk (A, B), on the face (C) and on the leg (D).
View Figure 1
Figure 1: Macula scarred lesions hyperpigmented on the trunk (A, B), on the face (C) and on the leg (D).
View Figure 1
 Figure 2: Cervical MRI showing extensive intramedullary T2 hypersignal of C6 to C7 without enhancement on T1 after gadolinium injection and Fat saturation. The remainder of T2 hypersignals is related to a truncation artifact.
View Figure 2
Figure 2: Cervical MRI showing extensive intramedullary T2 hypersignal of C6 to C7 without enhancement on T1 after gadolinium injection and Fat saturation. The remainder of T2 hypersignals is related to a truncation artifact.
View Figure 2
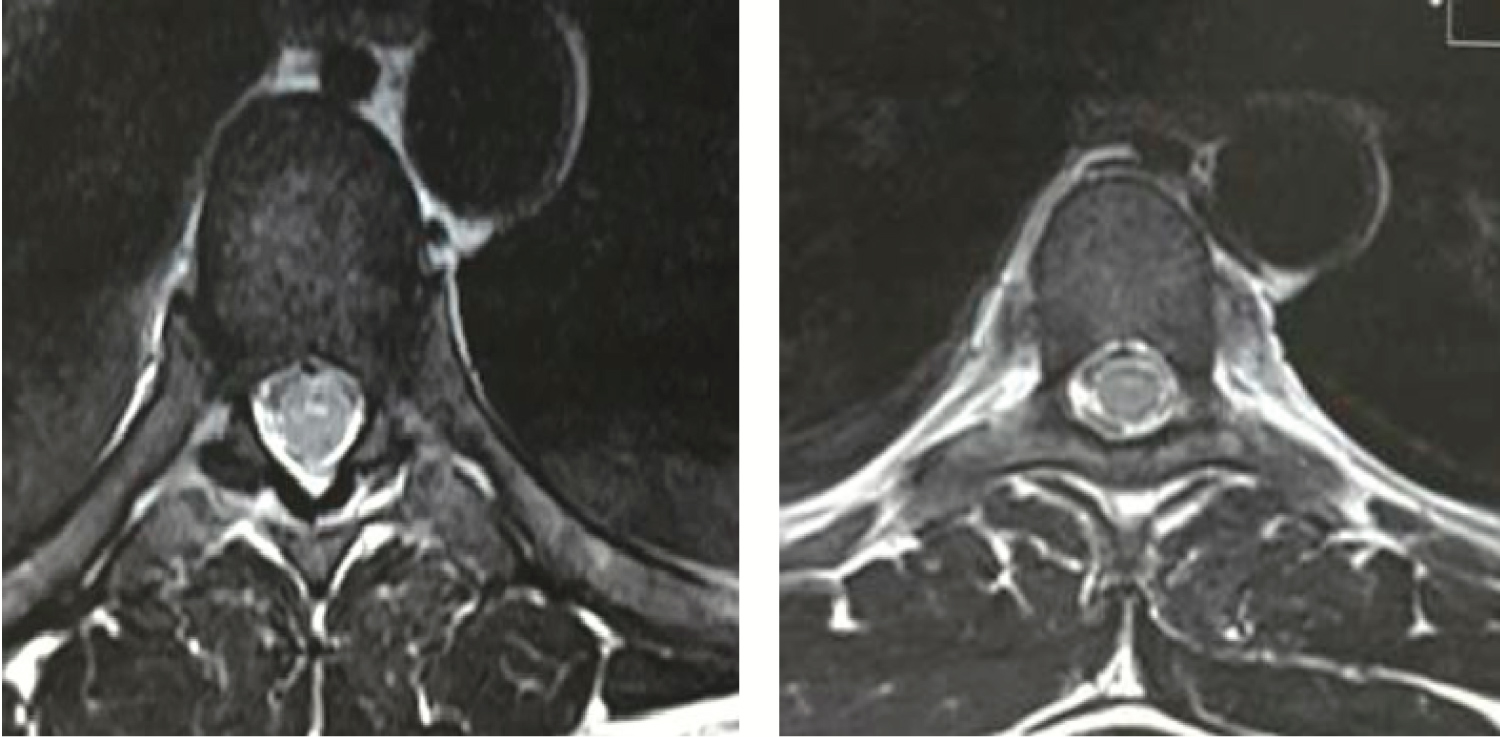 Figure 3: Cervical MRI T1 gado showing normal aspect of the spine (axial coupes).
View Figure 3
Figure 3: Cervical MRI T1 gado showing normal aspect of the spine (axial coupes).
View Figure 3
This study reports a case of acute transverse myelitis caused by VZV infection in an adult immunocompetent patient. Several cases of VZV myelitis in adult patients have been described in the literature [11,14-21]. Some of these cases concerned immunocompetent patients aged 20 to 79 years [14-19]. In our case, our patient had no defect, the biological balance was normal (blood sugar, hepatic, HIV serology, CD4). Typical presentation of VZV-induced Acute Transverse Myelitis consists of rapidly progressive motor, sensory and autonomic dysfunctions that are usually preceded by a dermatomal rash involving the same spinal level [22]. This typical description was found in our patient. The delay between chicken pox and acute transverse myelitis onset is variable, 15 days with our patient. For Alungal, et al. myelitis can occur with the rash or may be delayed for up to 2 weeks [18]. The diagnosis of myelitis is based on spinal MRI which was normal in our patient. This case is found in the literature or up to 40% of cases have no findings on MRI [23]. Polymerase chain reaction is now the standard methodof diagnosis for many viral CNS infections [24,25]. In the case of VZV myelitis, the diagnosis is based on the detection of VZV DNA PCR or the production of VZV IgG in the CSF [14-16,18]. However, in some cases, PCR for VZV DNA and anti-body, viral isolation, and viral culture can be all negative [26]. This confirmation was not necessary in our context because our immunocompetent patient presented a rash typical of chickenpox and had no history of vaccination with VZV. Indeed, diagnostic confirmation was rare in an African context due to the under-equipment of laboratories. For example, in a study from Guinea, authors had found that the 2 cases of VZV myelopathy were diagnosed by blood serology and PCR in blood sample [13]. VZV vaccination is not integrated into the national vaccination program of Burkina Faso. The standard treatment regimen for varicella zoster myelitis is not yet established. However, several authors suggest that treatment with high dose acyclovir and steroid is effective [14,27,28]. According to VZV myelitis treatment, early antiviral agents are important to prevent post-herpetic neuralgia [29]. The recommended dose for immunocompetent adult varicella or herpes zoster is 1000 mg 3 times daily for 7 days a total dose of 21 g [30]. In our case, the patient received a daily dose of 1000 mg for 20 days, which is equivalent to the total recommended dose. Corticosteroid therapy was combined as a 120 mg/day bolus for 3 days followed by oral corticosteroid therapy. In some studies, patients were treated with only intravenous acyclovir for 21 days without steroids [17,19]. However, the use of acyclovir was not consistent in all series. Thus, Yýlmaz, et al. were not using acyclovir to treat the 2 cases of VZV myelitis; corticosteroid therapy was used in one case [14]. Plasmapheresis can be used during 5 days to improve in case [15]. The prognosis is generally thought to be quite favorable, with complete recovery occurring in about 55-75% of cases [6,31]. Complete recovery occurred in 4 weeks of treatment. In the study of Yýlmaz, et al. the two patients had fully recovered at 1 year of follow up [14]. The early recovery in our case could be explained by the use of recommended dose of acyclovir.
Transverse VZV myelitis in an adult immunocompetent patient following cutaneous rash is extremely rare in our context. Clinical outcome was favorable after recommended dose of acyclovir, corticotherapy and rehabilitation.
This study was approved by the local ethical Committee of Yalgado Ouedraogo University Teaching hospital. All the patients gave their written consent to participate to this study.
The patients give his consent to the publication.
All the data and materials were available with the corresponding authors.
The authors do not report any conflict of interest.
No funding.