Background: HIV/AIDS continues to be a major global public health issue, having claimed. The rapidly expanding access to antiretroviral therapy (ART) is increasing survival of global HIV epidemic dramatic ways and AIDS-related mortality rates are declining fastly.
Objectives: The aim of this study was to determine survival status and predictors' of mortality among ART patients attending Hawassa Comprehensive Specialized Hospital 2020.
Methods: A five years retrospective cohort study was conducted involving all patients seen were reviewed between from January 2015-December 2019. The data was analyzed using SPSS version 25.0. Kaplan-Meier Log-rank model was used to estimate the survival time of ART patients based on explanatory variables. Bivariate and multivariate Cox proportional hazards regression models was performed to identify the independent predictors for mortality.
Result: Overall survival probability of ART patients was 74%. The death incidence rate of 0.135 per 100 person- years with medial survival of 34 month. WHO clinical stage III and IV (HR = 3; 95% CI =, 0.9-9.5, p = 0.04); age > = 60 (HR = 1.6; 95% CI = 0.3-2, p = 0.04); Functional status bed ridden (HR = 3.1; 95% CI = 1.2-9.4, p = 0.04); hemoglobin level (HR = 2.38; 95% CI = 0.91-6.28) were independent predictors of mortality among RVI patients.
Conclusion: Survival rate of ART patients in this study was low as compared to other studies conducted in the developed world. Strengthening ART care centers, improving community awareness on PLWHA, timely diagnosis and early initiation for treatment may be necessary to increase patient survival.
Antiretroviral therapy, Human Immunodeficiency virus, Mortality, Survival, Ethiopia
HIV/AIDS continues to be a major global public health issue, having claimed almost 33 million lives so far. In spite of that, with increasing access to effective HIV prevention, diagnosis, treatment and care, including for opportunistic infections, HIV infection has become a manageable chronic health condition, enabling people living with HIV to lead long and healthy lives. There were an estimated 38.0 million people living with HIV at the end of 2019 [1,2]. The main population groups and their sexual partners accounted for over 60% of all new HIV infections globally among the age group 15-49 years (an estimated 62%) in 2019.
In eastern European and central Asia, Asia and the Pacific, western and central Europe and north America and Middle East and north Africa, these groups accounted for over 95% of new HIV infections in each of these regions and Over two thirds of all people living with HIV live in the WHO African Region (25.7 million) [1,3,4]. Ethiopia is one of the hardest hit sub-Saharan African countries by the HIV pandemic. An estimated 738,976 Ethiopians are currently living with HIV [5]. According to the Ethiopian Demographic and Health Survey 2016 (EDHS 2016), the national HIV prevalence is 0.9%.; the urban prevalence was 2.9%, which is seven times higher than that of the rural (0.4%).
The 2016 EDHS also show that the HIV prevalence varies from region to region ranging from less than 0.1% in Ethiopia Somali to 4.8% in Gambella. Furthermore, the 2018 spectrum HIV estimate indicate that the 2017 HIV prevalence in regions ranges from 0.16% to 4.34% [6,7]. The 2016 World Health Organization guidelines recommending early ART initiation to all PLHIV irrespective of CD4 cell count were based on a growing body of evidence showing the increased risk of AIDS or death associated with delaying treatment [8].
The rapidly expanding access to antiretroviral therapy (ART) is increasing survival of global HIV epidemic dramatic ways and AIDS-related mortality rates are declining fastly. So far, the rising up of usage of ART has decreased an estimated of 6.6 million HIV/AIDS related deaths worldwide predominantly in underdeveloped and developing countries [3,9]. As a result of concerted international efforts to respond to HIV, coverage of services has been steadily increasing. In 2019, 68% of adults living with HIV globally were receiving lifelong antiretroviral therapy (ART). At the end of 2019, 25.4 million people were accessing antiretroviral therapy. Antiretroviral therapy (ART) reduces HIV replication and the infection of new cells, and it improves the immune system function. Therefore, ARV therapy positively influences the quality of life and the survival of seropositive HIV carriers [1,10]. Antiretroviral treatment began in 2003 and free ART was launched in Ethiopia in 2005. An estimated 738,976 Ethiopians are currently living with HIV and all of them require antiretroviral treatment (ART) however only 426,000 are currently taking ARV [5,11].
A very few studies which are conducted in Ethiopia and other countries on mortality of HIV adults shows that a timely initiation of ART among HIV/AIDS adults has decreased the mortality of the HIV patients and has a positive impact on the survival of those particular study groups. And CD4 count, WHO clinical stage, baseline hemoglobin, cotrimoxazole prophylaxis therapy (CPT) , Older age, male sex and HAART use as a predicting factors [2,8,11]. But there are no possible studies conducted at the study are area on the survival and predicting factors. The aim of this study was to determine predicting factors associated with survival of HIV/AIDS patients at Hawassa comprehensive specialized hospital.
The study was conducted in Hawassa University Specialized Hospital providing ART and IPT service in Hawassa City Administration. It is located 273 km south of Addis Ababa. The hospital gives services for approximately two million people and a teaching Hospital with basic facilities for HIV care and treatment and with established clinical set up and highly trained medical personnel. The hospital has started pre-ART and ART services since July 2006.
Institutional based retrospective study was conducted between January 2015 to December 2019 in Hawassa comprehensive specialized hospital to assess survival in PLWHA and who are on ART.
Source population: Person living with HIV/AIDS, age ≥ 15 years and started ART treatment in Hawassa comprehensive specialized hospital.
Study population: Those patients fulfilling the following criteria
Inclusion criteria
• HIV positive adults aged 15 yrs or older who started ART
• HIV patients with complete intake form, registers and follow up form
Exclusion criteria
• Diagnosis is made outside of health institution
• Women who were pregnant at the time of ART initiation and lactating mother
The sample size was determined using double population proportion formula by considering CD4, functional status and WHO stage as the major predictor variables [12]. Moreover, CD4 is considered as independent predictor since it gives the maximum sample size. Sample size was calculated by using open Epi info version 7 statistical packages.
P1: is percent of completed with the outcome
P2: is percent of non-completers. with the outcome
Z α/2: is taking CI 95%: 80% power
r: is the ratio of non-completers to completers 1:1
Sample size calculation was done by considering determinant factors.
|
S.N |
Variables |
CI |
Assumptions |
Total sample size |
References |
|
1. |
CD4 |
95% |
P1 = 54% P2 = 7.5% |
483 |
[13] |
|
2. |
WHO stage |
95% |
P1 = 65% P2 = 34% |
92 |
[14] |
|
3. |
Bedridden |
95% |
P1 = 66% P2 = 33% |
88 |
[14] |
|
P1: is percent of completed with the outcome |
Zα/2: is taking CI 95% |
r is the ratio of non-completers to completers 1:1
✓ Then the largest sample size (n = 483).
Study participant were selected by using systematic random sampling method using commands in Excel all 464 records of patients receiving ART in Hawassa comprehensive specialized hospital were listed in an excel spreadsheet, and a randomly selected 483 patients were studied.
The main outcome measure was time to event in month. The time of survival was calculated in months by using the time between the dates of ART treatment initiation and the date of the event or censoring. The independent determinant variables were Socio demographic characteristics and Base line clinical data's. The ART patients were followed to the date of death, lost to follow up, transferred out or to the end of the study. Patients were considered as censored if they were lost to follow up or transferred out.
A data collection form was developed from ART entry and follow up from being used in the ART clinic. The data was collected by reviewing pre-ART register, laboratory request and follow up form. The most recent laboratory results before starting ART was used as a base line value. Data quality was controlled by designing the proper data collection materials and through continuous supervision. All completed data collection form was examined for completeness.
The cleaned and coded data were entered into Epidata version 4.6.2. An analysis was done based on 5-year cohort follow up. Finally, data was exported to SPSS version 25.0 for analysis. Descriptive statistics of numeric variables were presented in medians with interquartile range (IQR), categorical variables are presented using frequency and percentages. TB-free survival time was estimated by applying the Kaplan-Meier Log-rank model to estimate the Occurrence time of TB based on explanatory variables. Bivariate and multivariable Cox proportional hazards regression models were performed to the independent determinants.
Lost to follow up: if a patient discontinued ART for at one to three month as recorded by ART physician
Event: - PLWHIV on ART, who died during the study period
Survival: lack of experience of death
Ethics approval and consent to participate
Ethical clearance was obtained from research and ethics committee (REC) of School of Nursing and Midwifery, College of Health Sciences, Addis Ababa University. Permission letter to access patients' data was obtained from the hospital outpatient authorities. As we are reporting a retrospective study of medical records, all data were fully anonym zed before we accessed them and the ethics committee waived the requirement for informed consent.
A total of 483 participants were surveyed, of whom 262 (54.2%) were male. The mean age of respondents was 32.8 ± 12.8 years (Mean ± SD), with a range from 18 to 68 years. More than half 271 (56.1%) of the respondents were married. In regards to participant's education, 271 (56.1%) of the respondents were secondary and above education while the rest 212 (43.9%) was lower than primary. Only 26 (25.50%) of population attended higher education. Almost half 247 (51.1%) of the respondents have history of substance use.
By occupation, 123 (25.5%) of respondents were government employed. Most of the participants were, from Urban area, and only 186 (38.5%) were from the rural area. Regarding religion majority was Orthodox religion follower 225 (46.6%) (Table 1).
Table 1: Socio-demographic characteristics of HIV patients who were enrolled for ART care at Hawassa University Comprehensive specialized Hospital Sidama, Ethiopia, from January 2015 to December 2020 (n = 483). View Table 1
More than half 356 (73.7%) of study participants were WHO clinical Stage I/II and medium of current CD4 count = 456 cells/μL. Seventy six (76.2%) of respondents were in CPT prophylaxis and (93.8%) were IPT completed. Three hundred six (69.7%) of respondents functional status was working and more than half of respondents BMI were less than 18 kg/m2 (Table 2).
Table 2: Clinical characteristics of HIV patients who were enrolled for IPT care at Hawassa University Comprehensive specialized Hospital, Sidamma, Ethiopia from January 2015 to December 2020 (n = 483). View Table 2
During the follow up time, 26 (5.4%) patients were deceased and death incidence rate of 0.135 per 100 person-years. The survival probability at eleventh month of ART initiation was 99.8%. This proportion reduces to 99.6, at the 14th months and preceded with 99.4%, 97.9%, 91.6%, and 76.4% at 2nd, third, fourth and the end of follow-up period, respectively (Figure 1). Base line WHO clinical stages (Log rank, p p ≤ 0.01), functional status (Log rank, p ≤ 0.001), age (Log rank, p ≤ 0.001 base line hemoglobin (Log rank, p ≤ 0.001), and CD4 count (Log rank, p p ≤ 0.01) were variables that showed the significant association with the survival of patients on ART with in Log rank test (Figure 2 and Table 3).
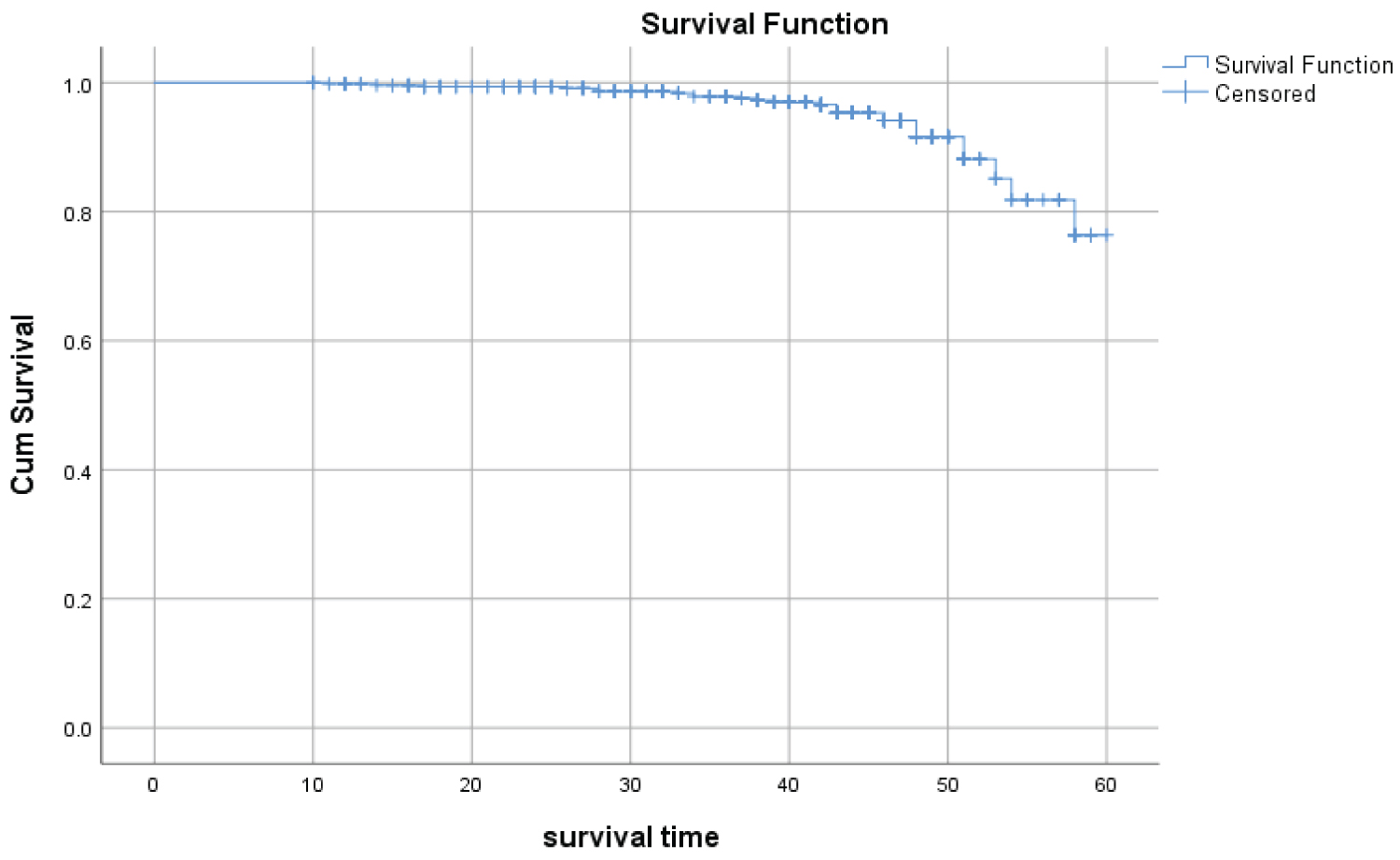 Figure 1: Shows overall survival probability of patients on ART starting from initiation of ART until the end of the study period among PLWHA, Hawassa town, Southern Ethiopia, November 2020.
View Figure 1
Figure 1: Shows overall survival probability of patients on ART starting from initiation of ART until the end of the study period among PLWHA, Hawassa town, Southern Ethiopia, November 2020.
View Figure 1
 Figure 2: Kaplan-Meier survival curves shows for comparison of A) TB/HIV co infection, (Log rank test; p ≤ 0.01); B) Functional status, (Log rank test; p ≤ 0.01); C) CD4 Cell count status, (Log rank test, p ≤ 0.01); D) Hemoglobin count, (Log rank test; p ≤ 0.01) and E) Age of the patients, (Log rank test; p ≤ 0.01) at base line among PLWHA, Hawassa town, Southern Ethiopia, November 2020.
View Figure 2
Figure 2: Kaplan-Meier survival curves shows for comparison of A) TB/HIV co infection, (Log rank test; p ≤ 0.01); B) Functional status, (Log rank test; p ≤ 0.01); C) CD4 Cell count status, (Log rank test, p ≤ 0.01); D) Hemoglobin count, (Log rank test; p ≤ 0.01) and E) Age of the patients, (Log rank test; p ≤ 0.01) at base line among PLWHA, Hawassa town, Southern Ethiopia, November 2020.
View Figure 2
Table 3: Baseline characteristics and probability of ART survival during 5-year of follow-up (Kaplan-Meier method) of HIV patients receiving ART, Hawassa University Comprehensive specialized Hospital, Sidama, Ethiopia from January 2015 to December 2019 (n = 483). View Table 3
To identify the independent predictors of survival after initiation of ART, Bivariate and multivariate Cox regression models were used. Bivariate Cox regression model, base line WHO clinical stage, CD4, age, hemoglobin, and functional status and HIV/TB co-infection showed significant association with early mortality after initiation of ART (Table 2). After multivariate analysis, four baseline factors could be independently identified: WHO clinical stage III and IV (HR = 3; 95% CI =, 0.9-9.5, p = 0.04); age > = 60 (HR = 1.6; 95% CI = 0.3-2, p = 0.04); Functional status bed ridden (HR = 3.1; 95% CI = 1.2-9.4, p = 0.04); hemoglobin level (HR = 2.38; 95% CI = 0.91-6.28) (Table 4).
Table 4: Cox regression analysis of the determinants of the incidence of TB among adults, who completed IPT care at Hawassa university comprehensive specialized hospital in Sidamma Regional State, January 2015 to December 2019 (n = 483) View Table 4
In this historical cohort study, we found that the independent significant predictors of lesser survival in patients living with HIV/AIDS after initiation of ART were, Hemoglobin Functional status, advanced WHO staging (III and IV) and CD4 cell count < = 200 (Cells/μL). In univariate analysis, patient survival under ART was significantly associated with clinical AIDS stage at start, baseline CD4 count, hemoglobin, age, HIV/TB co-infection and functional status. In multivariate analysis, only hemoglobin < 11 g/dl (Anemia), WHO clinical stage and functional status remained significantly associated with survival.
In our study, there were 26 (5.4%) deaths in 19194 PYO, yielding an incidence rate of 0.135 per 100 person-years. The estimated survival probability of the cohort at 1, 2, 3, 4, and 5 years were 99.8%, 99.4%, 97.9%, 91.6% and 76.4%, respectively. This result shows that there was a better survival of ART patients in relation to other findings in Africa. The same research conducted in a Malawi shows, the probability of being alive on ART at 6, 12 and 18 months was 89.8%, 83.4% and 78.8% respectively [7]. On the other side, the mortality rate was comparable to most studies, especially, in the 1st six months [15-17]. We might explain this by the fact that most of the patients in this study were on advanced status of the disease which is 57 (82.6%) had CD4 < 200 Cells/μL and 107 (84.3%) were in WHO stage III & IV).
Our study results confirm that, the relationship between WHO staging (III and IV) and mortality after controlling for confounding, which is in agreement with studies done in north and west Ethiopia which shows similar result of high mortality among advanced WHO clinical stage and respectively [2,8,10]. Another study which was conducted at south Ethiopia and Debremarkos referral hospitals indicates that individuals with WHO stage II and IV at baseline had an increased rate of risk of death compared to these with a WHO stage I and II and being ambulatory and bedridden. A Five-Year Retrospective Cohort Study in Kagera Region of Tanzania also has the same result of the above [18].
Study conducted in Far-North Province, Cameroon showed that patients with low hemoglobin at diagnosis had almost twice as significantly as higher risk of mortality compared to patients with high number of hemoglobin 2.38 (0.91-6.28) (0.0478) [19]. Our study result also shows similar progression this may be due to hematologic problem with patients progressed to AIDS at a faster rate and patients whose hemoglobin number < 11 g/dl (Anemia) were in high mortality in response to viral killing. A study done in south Africa implicated that a less number of hemoglobin in HIV/AIDS patients was one of the main indicators of increased mortality which is a hemoglobin concentration ≤ 8 g/dl [20], this result has is similar to this present study. Similarly, a meta- analysis study which is conducted in Adults Initiating Antiretroviral Therapy (ART) in Low- and Middle-Income Countries shows also being anemic was another determining factor for mortality of HIV/AIDS patients which was also supported by a thesis done in France at University of Bordeaux [21,22].
In this research survival status of the patients was determined by the functional status of the patients. Bed ridden and ambulatory status of the patients were seen the main determinant factor. This is similar to the research conducted in Somali region with the result of a bedridden functional status. Other studies which are conducted in African also shows that one of survival status determinant of ART patients was functional status of the patients especially bedridden and ambulatory status [10,23-27]. The same kind study done in far east and India explains that functional status of ART patients was major determinant factor of mortality and survival of the patient during the study period [28,29].
We are very grateful to the Hawassa University collage of Health sciences, Hawassa University Comprehensive specialized Hospital. We would also like to thank the staff of the ART clinic of Hawassa University Hawassa comprehensive specialized Hospital, the study participants, and the data collectors. A preprint has previously been published (1).
Not applicable.
For those who are interested the datasets analyzed during the current study are available from the corresponding author on reasonable request.
The authors declare that they have no competing interests.
Ethical clearance was obtained from research and ethics committee (REC) of School of Nursing and Midwifery, College of Health Sciences, Addis Ababa University. Permission letter to access patients' data was obtained from the hospital outpatient authorities of Hawassa university specialized hospital. As we are reporting a retrospective study of medical records, all data were fully anonym zed before we accessed them and the ethics committee waived the requirement for informed consent.
The research was funded by Addis Ababa University. The University does not have any role in the design of the study and data collection, analysis, and interpretation of data and in writing the manuscript should be declared.
BB, AF, conceived, designed and developed the data collection instruments. BB and AF performed the statistical analysis and wrote all versions of the manuscript. All authors critically revised and approved the final manuscript.
The authors declare that they have no competing interests.