S. aureus meningitis usually occurs in the postoperative neurosurgical. There are few cases from the community. We report the case of an 83-year-old woman undergoing alternative therapy for rheumatoid arthritis with bee stings on her knee. She was hospitalized with an allergic reaction after the fourth session. She remained in the hospital for 4 days and was discharged in good general condition. Ten days after discharge, the patient returned to the unit with complaints of headache and fever for 7 days. On admission, she was found to have altered mental status, dysarthria, and meningeal rigidity. A diagnosis of S. aureus bacterial meningitis was made. Treatment with ceftriaxone and oxacillin was administered, and the patient had a favorable outcome. In our report, we describe a case of bacterial meningitis possibly associated with bee stings, because there is a causal relationship between alternative therapy with bee stings and the occurrence of meningitis, and the S. aureus isolated here had a susceptibility profile compatible with community germs. This study is relevant because there are no reports in the literature describing bacterial meningitis due to S. aureus as a result of patient exposure to bee stings.
Staphylococcus aureus, Meningitis, Bee sting, Insects, Bacterial infection
S. aureus meningitis is commonly encountered in postoperative neurosurgical cases, with few reports from the community without a history of surgical intervention. We describe a case of bacterial meningitis which we hypothesize was caused by exposure to bee stings.
A retired 83-year-old Brazilian woman from a rural area of São Paulo with a history of rheumatoid arthritis and systemic arterial hypertension was admitted to the hospital with sudden onset of urticaria and dyspnea after the fourth session of consensual exposure to bee stings on her right knee for the treatment of arthritis. She had undergone the procedure once a week for the past 3 weeks (Figure 1).
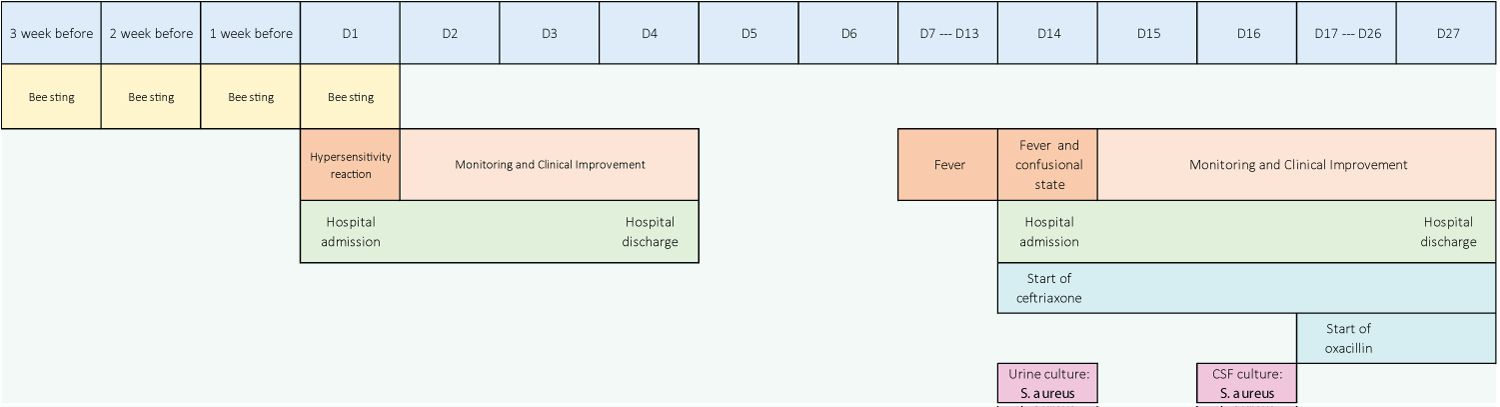 Figure 1: The clinical course and relevant events.
View Figure 1
Figure 1: The clinical course and relevant events.
View Figure 1
At the time of admission, a diagnosis of severe hypersensitivity reaction was considered. Therapeutic measures were taken, and the patient was admitted to the intensive care unit. She remained hospitalized for 4 days and was discharged in good general condition.
Ten days after discharge, the patient returned to the unit with complaints of headache, low back pain, dysuria, and fever of 38.8 °C for 7 days. Upon admission, she was found to have altered consciousness, dysarthria, and meningeal rigidity. A diagnosis of bacterial meningitis was made. Cephtriaxone was initiated, followed by further investigation with cranial computed tomography (CT) and laboratory tests.
Investigations on the first day of hospitalization revealed the following: Hemoglobin 14.3 g/dL, leukocytes 33,310 cells/mm 3 (82% segmented), platelets 282,000 cells/mm 3 ; C-reactive protein 427.60 mg/L; blood cultures negative, and urine culture positive for S. aureus (sensitive to oxacillin). CT revealed no intracranial abnormalities.
Cerebrospinal fluid (CSF) investigations on the third day of hospitalization revealed the following: leukocytes 75 cells/mm 3 (neutrophils 85%, lymphocytes 12%, monocytes 2%, and macrophages 1%) and red blood cells 1 cell/mm 3 ; protein 535 mg/dL; glucose 25 mg/dL (no paired serum glucose); and positive culture for oxacillin-sensitive S. aureus (Figure 2).
 Figure 2: Cerebrospinal fluid appearance.
View Figure 2
Figure 2: Cerebrospinal fluid appearance.
View Figure 2
After identification of S. aureus in the CSF, intravenous oxacillin 2g every 4 hours was started, and intravenous ceftriaxone 2g 12/12 hours was maintained. No echocardiography was performed for further investigation of endocarditis. The patient had a favorable outcome throughout hospitalization, with a good clinical response and progressive neurological improvement. Treatment was terminated after 11 days with oxacillin and 14 days with ceftriaxone.
After discharge, the patient had no further S. aureus -related hospitalizations or complications.
There are a few reports in the literature regarding bacterial infections associated with bee stings. The few cases described are mostly skin and soft tissue infections [1-4]; however, there are cases that suggest an association between stinging and the occurrence of endophthalmitis [5], empyema [6], and splenic abscesses [7].
Various pathogens have been described as being associated with invasive infections following insect stings or bites, including Streptococcus pyogenes [1,2], Streptococcus group A, Staphylococcus aureus [3], Mycobacterium chelonae [4], Pseudomonas aeruginosa , Aeromonas veronii [5], Enterococcus faecium [7], and Vibrio vulnificus [8]. Kontoyiannis, et al. have also described fungal infections associated with insect bites [9].
Skin and soft tissue infections are among the most common complications of insect bites or stings [10]. In a study on S. aureus infections conducted in a remote geographical region, 14.8% of patients reported an insect bite as the causative event [11]. Segarra-Newnham, et al. have described community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) in patients with insect and spider bites [12].
In our report, we describe a case of bacterial meningitis possibly associated with bee stings, since there is a causal relationship between alternative therapy with bee stings and the occurrence of meningitis, and the S. aureus isolated in this case presented a susceptibility profile compatible with community germs. Cases of S. aureus meningitis commonly present with postoperative meningitis or are acquired from the community due to hematogenous spread by different risk factors, such as intravenous drug use [13].
Different studies have indicated a higher mortality in S. aureus meningitis cases in the community than in postoperative ones [13-15]. The overall mortality from S. aureus meningitis in different case series is 23% [14], 27% [15], 36.4% [13], 56% [16], and 67% [17]. In our case, we managed one patient who had a favorable outcome after treatment.
The importance of bees as carriers of pathogenic bacteria that can be inoculated through bee stings is unclear. We demonstrate in this report a possible association between S. aureus meningitis and bee stings, considering that such an event could be a "gateway" for staphylococcal infection and subsequent hematogenous dissemination. This could account for the central nervous system infection seen in our patient.
This study is relevant because of the absence of any reports in the literature describing bacterial meningitis due to S. aureus as a result of exposure of patients to insect stings or bites.