Background: Intestinal Parasitic Infections (IPIs) are a major public health problem in tropical and subtropical regions. This study aimed to determine the prevalence of intestinal parasites in Yaounde III Subdivision during the COVID-19 pandemic.
Methods: A cross-sectional study was carried out from May to October 2020 during the COVID-19 pandemic. On the two hundred and six (206) stool samples collected from residents of four selected quarters in Yaounde III, Subdivision, macroscopic and microscopic analyses, using the simple floatation technique, were carried out.
Results: Results obtained from this study showed that only one parasite was present in this area (Entamoeba histolytica), with a prevalence of 6%. This prevalence was lower than what was obtained in previous studies, indicating that COVID-19 had a significant impact on the prevalence of IPIs in Yaounde III Subdivision due to the hygiene measures put in place by the Cameroonian Government. Some of the factors that were found to influence the presence of this parasite included: gender, social status, source of water, and family size, and these were significant at α = 0.05.
Conclusion: This study shows that due to the COVID-19 pandemic, some of the hygienic measures put in place by the government were effective to slow down the spread of this virus. Hence, it is important to control and prevent intestinal parasitic infections in and around Yaounde III Subdivision, to eradicate these infections.
Intestinal parasitic infections, COVID-19, Yaounde III subdivision
Intestinal Parasitic Infections (IPIs) are a serious public health problem and among the most common infections worldwide. Intestinal parasites are a diverse group of parasites that include single-celled protozoans and multicellular intestinal worms, responsible for various disorders such as food mal-absorption, chronic anemia, and poor cognitive performance, among others [1,2]. Current estimates show that at least more than one quarter of the world’s population is chronically infected with intestinal parasites and most of these infected people live in developing countries, where climatic conditions, poverty, poor hygienic practices, socio-cultural habits and demographics among other factors, favour their development and spread [3,4]. According to WHO [3], over 2 billion people worldwide are infected by intestinal helminths (mainly Ascaris lumbricoides, Trichuris trichiura, Ancylostoma spp and Schistosoma mansoni ), and protozoans as well (with about 50 million people infected by Entamoeba histolytica and about 2.8 million people infected by Giardia lamblia ), killing over 155,000 thousand per year, with 97% of deaths occurring in developing countries [3,5]. The epidemiology of intestinal parasitic infections shows that these parasites are found in every age group and in both sexes [6,7]. In Cameroon, it is estimated that for the past 15 years, 42% of school children have been infected by Ascaris lumbricoides, 53.4% by Trichuris trichiura and 14.7% by Necator americanus [5]. They have been associated with serious public health issues such as malnutrition, poor school attendance, anemia, growth retardation, morbidity, and mortality. The most common means of infection include the faeco-oral route and consumption of contaminated food and/or water, although some are zoonotic species like Cryptosporidium parvum and Balantidium coli .
Recent studies carried out have been able to establish a link between hygienic practices such as hand washing after visiting the toilets and before a meal, eating of unwashed or poorly cooked vegetables, and drinking water from unsafe sources; all these were greatly reduced during the COVID-19 pandemic [2,6,8]. In rural and semi-rural settings as well as in overcrowded cities, for example, the risk of contamination is higher as there is a considerable lack of sanitation facilities, potable water, adequate health care facilities, and proximity of households to latrines or points of liquid/solid waste and hence to be the source of some health problems such as malaria, dysentery, diarrhoea, typhoid and skin diseases [5,9]. These conditions can be identified in various regions of Cameroon, which over the years have experienced rapid population growth and an increased rate of rural exodus, contributing to the rapid urbanization of its main cities, like Douala and Yaounde, resulting in serious environmental and public health problems originating either from ignorance of hygiene and sanitation practices or poverty or insufficient/inadequate health care facilities [5,9]. In view to reduce the burden of intestinal parasitic infections in Cameroon, various strategies have been put in place to fight against their development and spread like Mass Drug Administration campaigns, but despite all these efforts, the disease burden is still very high [4]. Furthermore, in Yaounde III Subdivision, the climate is a tropical wet and dry type, which is convenient for the growth, development, and survival of intestinal parasites [10]; coupled to all these, self-medication and inadequate deworming also contribute to the presence of these parasites, as most natives will buy drugs from uncertified sources without any medical advice, which in a long run may result in drug resistance [11]. However, recently with the COVID-19 pandemic, strict policies on hygiene and sanitation standards were implemented in the whole world including Yaounde III Subdivision, to avoid or slow down the spread of the disease.
This study aimed to determine the prevalence of Intestinal Parasitic Infections (IPIs) in Yaounde III Subdivision during the COVID-19 pandemic, to determine if the hygienic measures put in place by the government could have an impact on the spread of intestinal parasites.
A cross-sectional study was carried out in the periphery of Yaounde III Subdivision as seen in Figure 1. Yaounde is located in the Centre Region of Cameroon, in the Mfoundi Division, at an altitude of 760 mm and has a surface area of 183 km 2 [12]. The population of Yaounde is over 2.8 million according to the last census carried out in 2005, where there are about 453,000 inhabitants in Yaounde III subdivision.
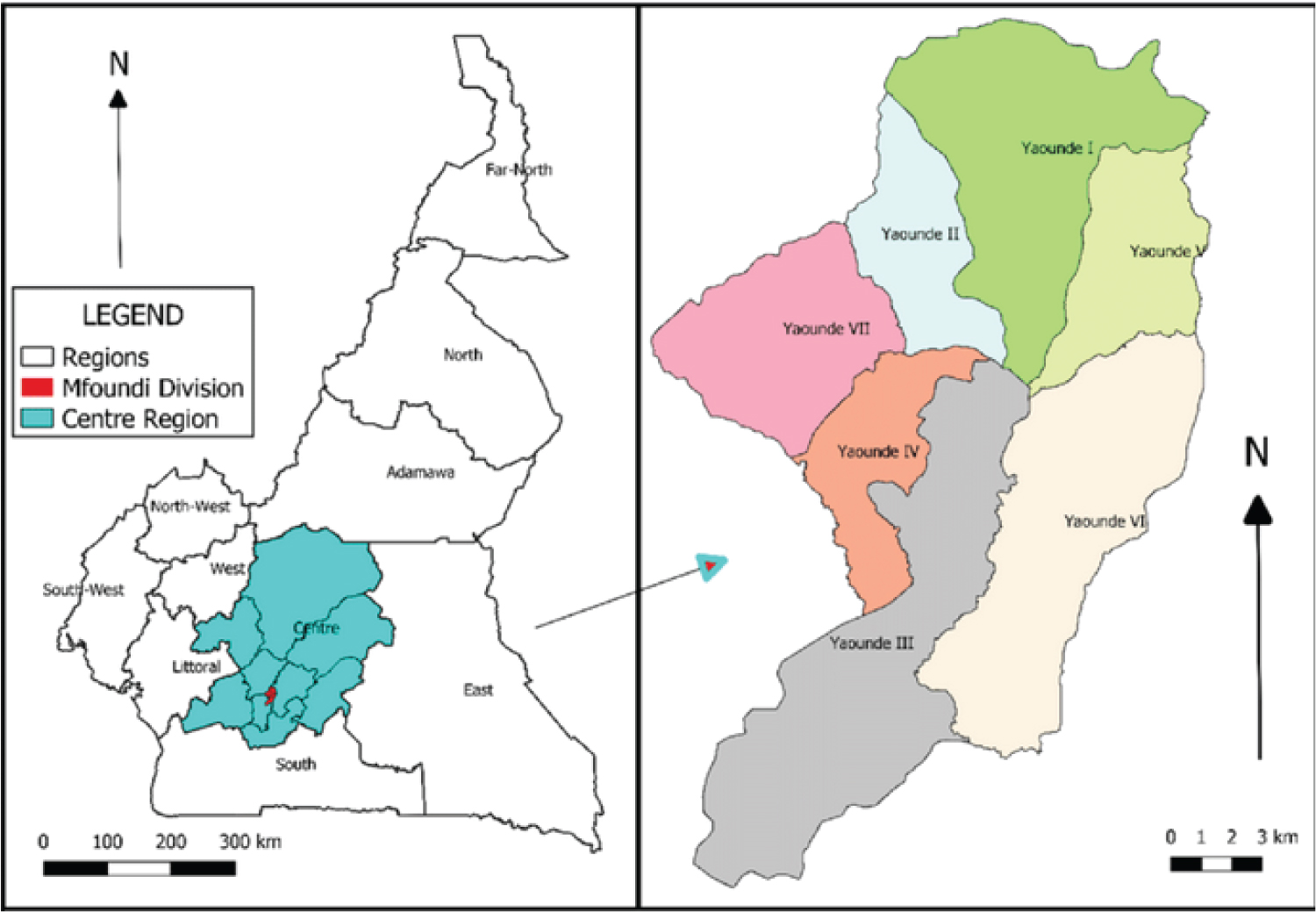 Figure 1: Yaounde III Subdivision.
View Figure 1
Figure 1: Yaounde III Subdivision.
View Figure 1
The sample size was determined using Lorenz’s formula [13] as shown below:
Where:
n = sample size
Z = 1.96% at 95% Confidence Interval
P = Estimated proportion of students being infected (in this case P = 0.5)
q = 1-P (that is the estimated proportion of students not infected (in this case q = 0.5)
e = desired level of precision
We randomly sampled four quarters and had a total of 206 participants, with 88 females and 118 females. Only individuals who gave their free and voluntary consent and provided stool specimens were included in the study and those who failed to provide the specimen were removed from the study.
Distribution of questionnaires and specimen containers occurred between May and October; our highest number of participants came from the first quarter visited Pharmacam. Those who gave their consent, an informed consent form, a questionnaire sheet carrying an identification code, and a specimen container, carrying the same identification code as on the questionnaire were given to each participant, aged between 2 and 90-years-old who accepted or were allowed to participate. On the day of collection, each specimen was first macroscopically observed. We then preserved each specimen with 10% and placed them in cartoons to ease transportation to the health center where we proceeded with microscopic examination [5,7,14].
The prevalence of infections according to socio-demographic factors [3,5] such as age and sex was evaluated, where;
The association between the level of infection and encountered risk factors were also determined [1,3].
Data obtained from the questionnaires were entered in EPI info software, version 72.2.6, where descriptive analysis of the sample (distribution of the population according to age and sex), as well as bivariate analysis were done, at a level of significance of α = 0.05; the results obtained here were then transferred to Excel 2007, where graphs and tables could be constructed.
The distribution of participants according to gender. It follows from the analysis of this figure that 118 participants were females (57%) and 88 were males (43%).
It follows from the analysis of Figure 2 that the study population included participants aged from 2-75 years-old, with a mean age 20.7 ± 16.3 years; the highest number of participants belonged to the age group of 10-19 years-old.
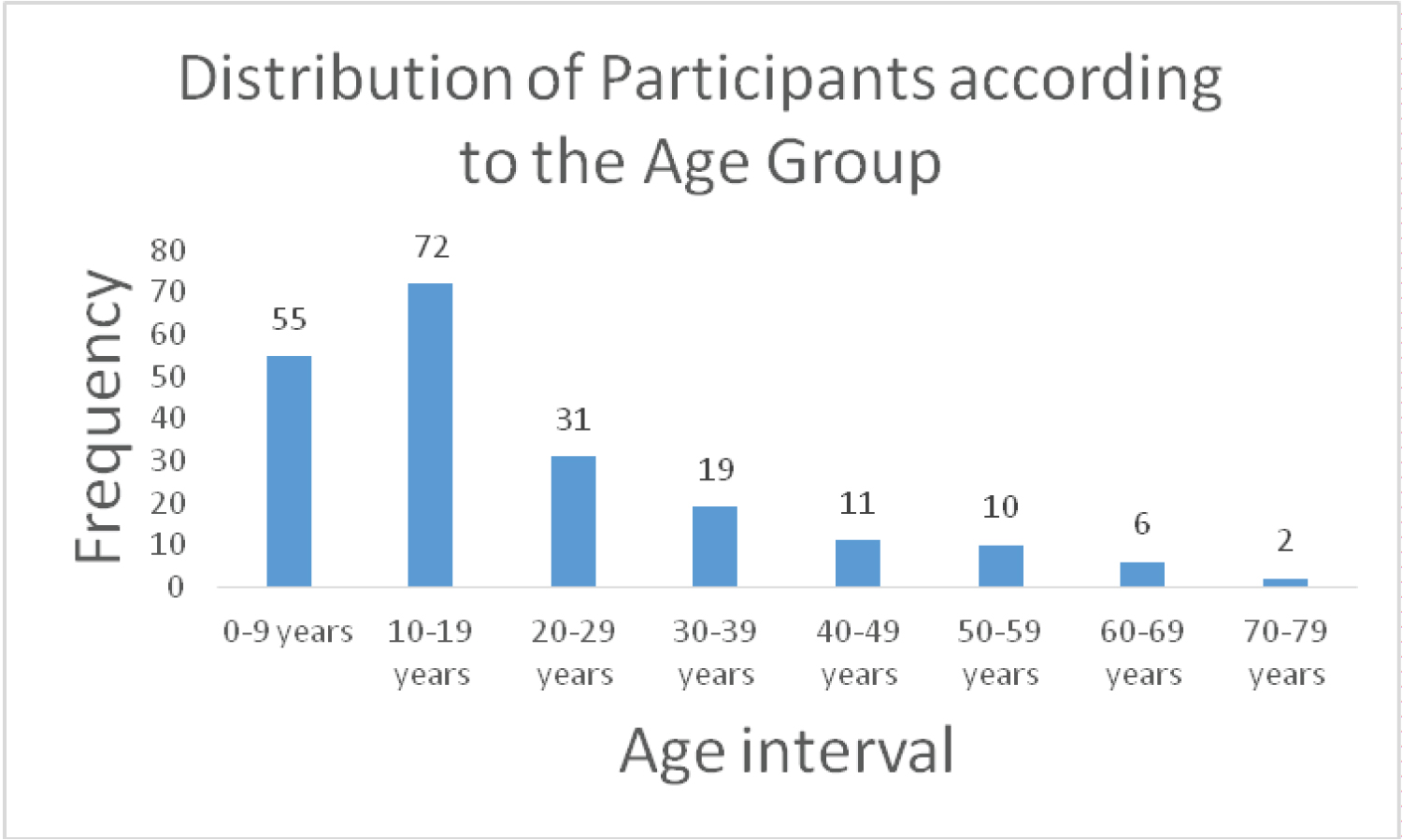 Figure 2: Distribution of participants according to the age group.
View Figure 2
Figure 2: Distribution of participants according to the age group.
View Figure 2
It appears from Figure 3 that four quarters were sampled, and the highest frequency of participants was identified as coming from Pharmacam, with a total of 82 participants out of 206 participants.
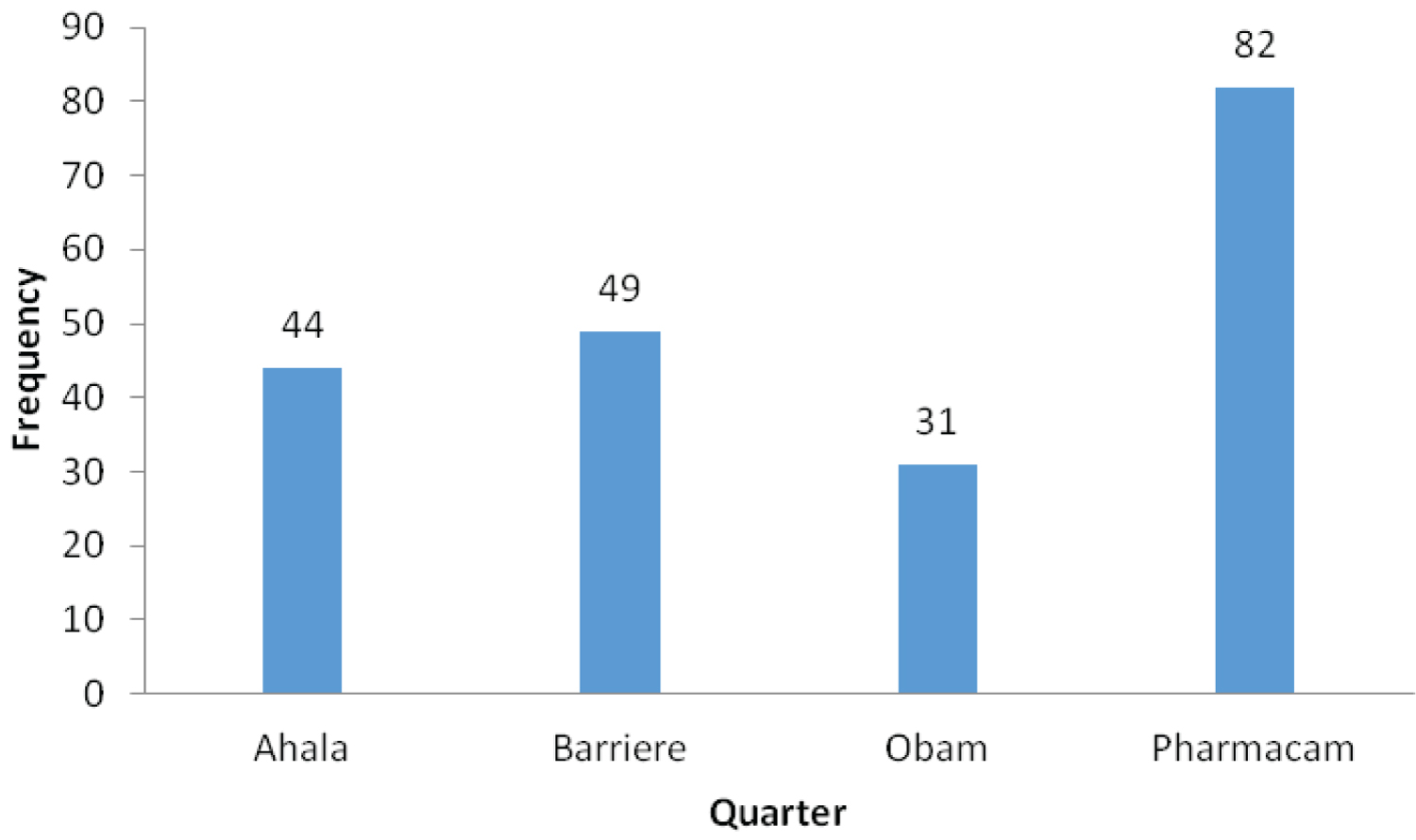 Figure 3: Distribution of participants according to the quarter.
View Figure 3
Figure 3: Distribution of participants according to the quarter.
View Figure 3
Table 1 shows the profile of the studied population according to socio-demographic factors. We can notice that a good majority of those who participated were individuals of secondary education (44.97%), followed by those of the nursery schools with 34.92%. As for the profession, we had our highest number of samples from students (66.32%), and the least from retired individuals (1.58%). We also noticed a divergence in the size of the families we visited as some were large, others medium, and some small.
Table 1: Profile of studied population according to socio-demographic factors. View Table 1
Table 2 shows the frequency of infected participants according to Socio-Demographic Characteristics. It appears from this table that both sexes were infected, with 8 female (66.67%) and 4 male cases (33.33%), hence females were more infected than males. Unfortunately, there is insufficient evidence to say that the prevalence of parasitic infections in this study area is gender related (p = 0.45 > 0.05).
Table 2: Frequency of infected participants according to socio-demographic characteristics. View Table 2
This goes in line with the results of Lucia, et al. [5] obtained in Lolodorf in the South region of Cameroon [5], as well as the results obtained by Signaboubo, et al. [4]. The age group 20-40 years recorded the highest level of infection (50%), this is contrary to the results obtained by Signaboubo, et al. [4].
The prevalence of IPIs was high in some quarters and null in others, with Pharmacam recording the highest number of cases (83.33%) and the association between the quarter and prevalence of infection came out to be statistically significant (p = 0.01 < 0.05). This corroborates the results obtained by Fusi-Ngwa, et al. [7], concerning the distribution of infection within quarters.
The low class was more infected (58.33%) than middle and high class individuals (41.67%). This goes in line with what Fusi-Ngwa, et al. [7]. Furthermore, the majority of cases were reported among students (50.00%) followed by private workers and self-employed individuals, but no case was recorded among retired individuals. These results are in line with those obtained by Payne, et al. [3], working in Babadjou in the West region of Cameroon.
A great majority of those infected (83.33%) took worm medicine at least once last year and did not take them again. This gives us an indication on the act of auto-medication and deworming which is not very efficient or not active at all since we still had cases of infection. Nevertheless, these results are in line with those obtained by Sylla, et al. [11], and those obtained by Fusi-Ngwa, et al. [7].
Out of 12 infected, 8 (66.67%) answered that they usually eat outside, indicating that the chances of getting contaminated when eating regularly outside are high; we also noticed an association between this behaviour and the prevalence of infection (OR = 1.43) although not statistically significant (p = 0.57 > 0.05) Almost similar results were obtained in Lolodorf [5]. The prevalence of infection was higher among secondary level individuals (66.67%), followed by those of primary and higher levels (16.67% each) and null for illiterates; this goes in line with previous results [4]. The fact that secondary level individuals, who constituted the greatest majority of our sample, were the most affected could be linked to the habit most students have of eating outside on their way to school or in their school canteens; hence further research should be done to prove this association.
During our survey, we noticed that the majority of the houses had traditional toilets (96 out of 185) and others had modern toilets (89 out of 185). There was an association between the toilet type and prevalence of infection as 75% of those infected had traditional toilets and 25% of those infected had modern toilets. These results corroborate with those obtained by Fusi-Ngwa, et al. [7].
Finally, we found out that many residents of Yaounde III Subdivision bought drugs from a safe source, that is pharmacies (125 out of 186), some from street vendors (39 out of 186) and others from local or traditional sources (22 out of 186). The association between the source of drugs and the prevalence could not be established, and hence could not be considered as significant statistically (p = 0.89) (Appendix).
This research reveals that out of the different protozoan and helminthic parasites existing, only one protozoan was identified, which was Entamoeba species , with a prevalence of 5.83%. This result might have been affected by the presence of the Coronavirus (COVID-19) pandemic, which has forced people to be constantly respecting hygiene and sanitation rules to avoid being infected by the virus, in Yaounde III Subdivision especially, where the pandemic was more severe.
Data and material are available to other researchers upon request.
The authors declared that they have no competing interest.
No funding.
The authors are sincerely grateful to the Senior Divisional Officer of Yaounde III Subdivision, Mr. BIWELE Serge Hervé and to the Director of the Ahala Health Centre.
DDSI, KPV, YC, and NACN contributed to the design of the study, data collection, led the analysis and drafting of the manuscript. All authors read and approved the final manuscript.
Ethical clearance was obtained from the National Committee on Research Ethics for Human Health. This work was carried out in accordance with the Declaration of Helsinki. All ethical rules involving research with disadvantaged groups such as prisoners have been respected. Patients were free to attend the study without any outside constraints.
Not applicable.