AIDS (Acquired Immunodeficiency Syndrome) is a condition caused by the Human Immunodeficiency Virus (HIV). HIV is a virus that attacks the immune system and weakens the body's ability to fight off infections and diseases. Approximately 37.6 million people (about twice the population of New York) worldwide are infected with the human immunodeficiency virus (HIV) according to data from the Joint United Nations Program on HIV-AIDS [1].
Malignant neoplasms are one of the leading causes of hospitalization and death in the HIV-infected population. The HIV mortality rate is 3.62 people per 100,000 inhabitants, 6.19 in the case of men and 1.17 for women [2]. The highest are registered in Quintana Roo with 10.25, Colima 9.40 and Campeche with 7.25 deaths per 100,000 inhabitants in each entity [2].
A study carried out by Rivera in Mexico in 2020 found that HIV-associated cancer was more frequent in men, at the colon and rectal level. The most common histological type was squamous cell adenocarcinoma (patients with good adherence to treatment), followed by non-Hodgkin lymphoma and Kaposi's sarcoma (patients with poor adherence or no treatment) [3].
The most frequent neoplasms are gastrointestinal, which are divided into two groups: AIDS-defining neoplasms: Kaposi's Sarcoma and Non-Hodgkin's Lymphoma (which are considered opportunistic tumors) and in second place are non-defining neoplasms: bronchopulmonary, anal, and hepatocellular [4]. Non-Hodgkin Lymphoma (NHL) is a type of cancer that affects the lymphatic system, which is part of the immune system. People living with HIV are at a higher risk of developing NHL due to their weakened immune system. NHL can occur in different parts of the body and can cause symptoms such as swollen lymph nodes, fever, night sweats, and weight loss. Given the enormous number of people infected with HIV that currently exist, it is considered a high-impact and high-cost disease, for which the objective is to minimize the effects of HIV-AIDS infection [5].
The purpose of this study is to present a case of an AIDS patient with Non-Hodgkin Lymphoma with a fatal outcome.
A 49-year-old male resident of Cancun has the following significant history: full immunization, SARS-CoV-2, 2 AstraZeneca doses, previous hospitalizations on two occasions in the last three years for pneumonia, transfusions in March 2022 for anemia, alcoholism for 29 years at a rate of 14 gr/day suspended 8 months ago. HIV positive for 20 years with intermittent adherence to treatment, currently with a third treatment scheme with ritonavir, darunavir, dolutegravir and tenofobir with emtricitabine.
The current condition begins by presenting a productive cough with whitish expectoration, unquantified fever, asthenia, adynamia, weight loss of 10 kg in 3 months, intolerance to the oral route, hair, and fetid evacuations. On physical examination: No neurological compromise, cachectic, pale integuments, tachypnoea, 82% oxygen saturation, globose abdomen, no palpable megalias, matte, decreased peristalsis, extremities with ++ edema, 2-second capillary refill.
Complementary studies: Laboratories: leukocytes 18.7 × 103/ ul, hemoglobin 10.8 g/dl, platelets 357 × 103 ul, lymphocytes 2.8%, lymphocytes 0.52 × 103 ul, CD4 T lymphocytes 8.63%, lymphocyte count 42.86 ul, HIV viral load 57.1 copies/ml.
Abdominal-pelvic tomography: minimal right effusion and ipsilateral basal consolidation area, retentionist stomach, splenomegaly with areas of hypodensity inside, probable cysts, abundant ascites fluid, probable cystic left testicular lesion, and abundant abdominal and inguinal lymph node conglomerates (Figure 1).
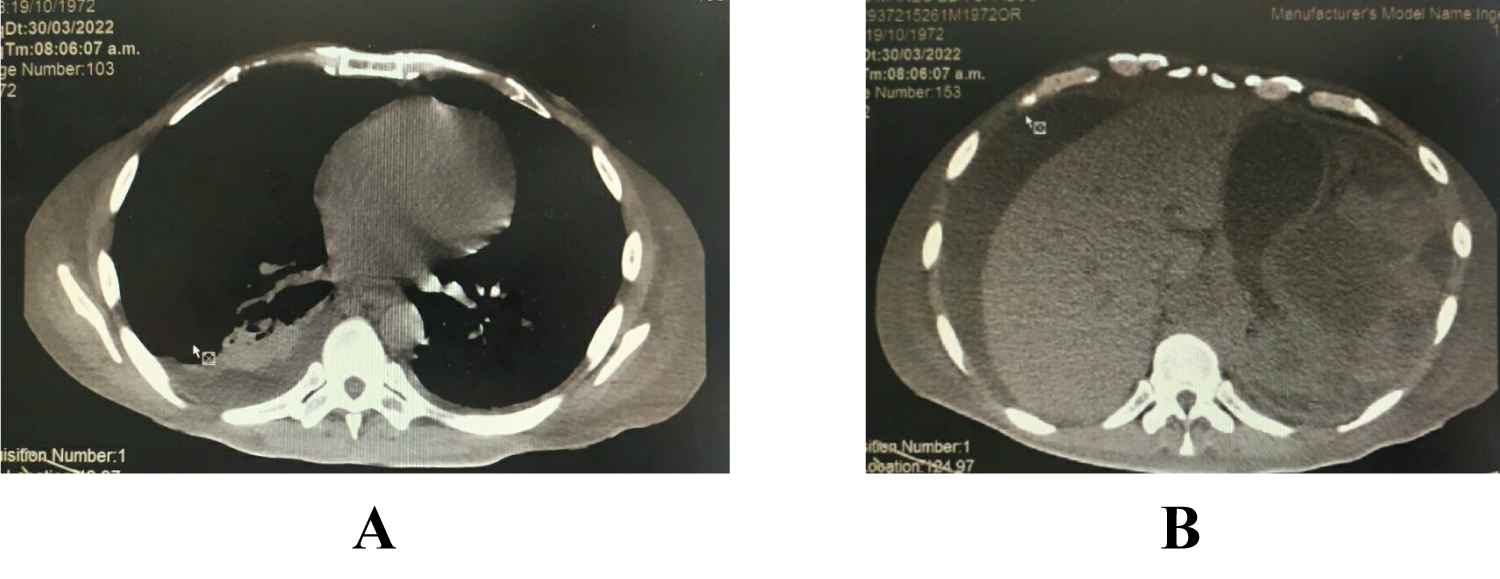 Figure 1: (A) Tomography of the lung with right pleural effusion; (B) Tomography of the abdomen with ascites fluid, splenomegaly.
View Figure 1
Figure 1: (A) Tomography of the lung with right pleural effusion; (B) Tomography of the abdomen with ascites fluid, splenomegaly.
View Figure 1
Endoscopy: Probable ulcerated activity, penetrated the duodenum with intestinal occlusion. Duodenal biopsy with atypical lymphocytic proliferation. The diagnosis of stage 3 AIDS was integrated, due to probable non-Hodgkin lymphoma, bacterial pneumonia. Treatment of pathology, pneumonia, with antibiotics with cephalosporins, is scheduled for gastrostomy and the biopsy result is awaited to request evaluation by medical oncology, however, he presents a torpid evolution and dies before receiving histopathology results.
The human immunodeficiency virus is not an oncogenic virus; however, segments in its genome seem to be involved in the growth of Kaposi's sarcoma cells. Its presence conditions a stimulus in B lymphocytes, altering antitumor activity, indirectly facilitating oncogenic viruses [5]. There are several factors that increase the risk of developing NHL in people living with HIV. One of the main factors is the degree of immune suppression. The lower the CD4 cell count (a type of immune cell), the higher the risk of NHL. People living with HIV who have not started antiretroviral therapy (ART) or have a low CD4 cell count are at a higher risk of developing NHL. Other factors that increase the risk of NHL in people living with HIV include co-infection with other viruses such as hepatitis B and C, Epstein-Barr virus (EBV), and human herpesvirus 8 (HHV-8). Lifestyle factors such as smoking and alcohol use may also increase the risk of NHL in people living with HIV.
It has been found that there are factors associated with an unfavorable prognosis such as age over 35 years at the time of diagnosis, intravenous drug use, advanced stages, CD4 count less than 100 uL [6].
In Mexico, the mortality rate from malignant tumors for the year 2019 is 70 deaths per 100,000 inhabitants. In Quintana Roo, rates of 50.93 to 62.44 are registered. There are currently no records of the percentage of non-Hodgkin lymphoma in the Mexican population [6].
The association of HIV and cancer is more frequent. The predominant ones in one stage of AIDS include Kaposi's disease and non-Hodgkin's lymphoma [7]. In this case, although the immunohistochemical study is not reported, due to the symptoms presented by the patient, the first pathological report, and the statistics make us suspect the presence of non-Hodgkin lymphoma.
There are currently no standard diagnostic tests for the diagnosis of HIV-associated cancer. Monitoring of HIV patients is performed by measuring CD4 lymphocyte levels and viral load. A lower level of CD4 lymphocytes than 200 ul cells has been associated with the presence of AIDS-defining neoplasms [8,9].
The patient reported adequate adherence to current antiretroviral treatment but had periods of absence from treatment. His CD4 count at the time of the symptoms of the current condition was less than 100 ul, predisposing to decreased immunity, which in turn favors the appearance of so-called opportunistic neoplasms [4,10].
The treatment of neoplasms is based on the origin of the neoplasm itself, the appropriate use of antiretrovirals and the prophylaxis and treatment of opportunistic diseases. Treatment for NHL in people living with HIV involves a combination of chemotherapy and ART. The chemotherapy drugs used to treat NHL can cause side effects such as nausea, vomiting, and hair loss. However, with proper medical care and treatment, people living with HIV can live long and healthy lives with NHL.
It should be noted that the clinical presentation of non-Hodgkin lymphoma is atypical, it does not have specific symptoms, often due to the appearance of masses, depending on the location and the symptoms it produces. In this case, it generated data of intestinal obstruction, which was the reason for performing an endoscopy.
The patient was in the AIDS stage due to the presence of neoplasia and according to the CD4 count, the diagnostic protocol was started, with a torpid evolution without being able to offer further treatment for the neoplasia.
Until now, little is known about the prognosis and influencing factors before and after cancer diagnosis in patients with HIV, which makes diagnostic methods difficult [9]. AIDS and Non-Hodgkin Lymphoma are two conditions that are closely linked. People living with HIV are at a higher risk of developing NHL due to their weakened immune system. The risk of developing NHL increases with the degree of immune suppression and other factors such as co-infection with other viruses and lifestyle factors [1,11-29].
The high mortality of patients with HIV, the atypical presentation of neoplasms in them and late diagnosis guide us to the importance of prioritizing preventive measures for the general population against HIV, secondary prevention in patients with HIV for adequate adherence. to antiretroviral treatment and decreased exposure to oncogenic agents.
The authors declare no conflict of interest in this review.
The authors received no funding for this case presentation.