Background: With increasing dependence on other people in old age, environmental resources become an important asset for older adults to experience healthy aging. Neighborhood conditions, therefore, are some of the multiple factors that contribute to the mental wellbeing of older adults. This study investigated whether and which neighborhood factors predicted depression and anxiety among American older adults followed up for over five years within the same neighborhood.
Methods: Two waves of publicly available longitudinal data from the National Social Life, Health, and Aging Project (NSHAP) were utilized. A hierarchical multiple regression model analysis was employed to explore the association between neighborhood factors and mental health. The secondary data contained a cohort of 1,731 older adults. Outcome measures were depression using the 11-item CES-Depression Scale and anxiety using the 7-item HADS Anxiety Scale. The predictors were four neighborhood factors: Social cohesion, social ties, neighborhood problems, and perceived neighborhood danger. We also adjusted for demographic and physical health characteristics.
Results: The mean age of the respondents was 71.4 ± 6.5 years and were mostly females (55.5%) and Whites (74.4%). Lower Neighborhood Social Cohesion and a higher Perceived Neighborhood Danger significantly predicted depression. However, the model only explained 2.8% of the variance in Depression. None of the neighborhood factors predicted depression following 5 years after adjusting for demographic and physical health characteristics and baseline depression, but the model significantly improved to 32.5%. Neighborhood problem was the only significant predictor of anxiety after adjusting for other covariates and explained 27.8% of the variance in anxiety.
Conclusion: The study sheds some light on the complexity of the relationship between neighborhood and mental health in older adults. Moreover, our findings suggest that city planners and policymakers can influence healthy aging through the proper mapping of a city and the reduction in disorderliness within communities for older adults. Therefore, future policy development and interventions should target improving both physical and social environments to enhancing the mental wellbeing of older adults.
Environmental correlates, Depression, Anxiety, Neighborhood problems, Older adults
The aging population faces physical and mental health problems in addition to social challenges. Even though most degenerative and inflammatory conditions are expected age-related continuum of diseases associated with the normal aging process [1], mental disorders, unlike these conditions, are not part of the normal aging process [2]. Older adults when compared to their younger counter parts experience lower, but substantial rates of mental health [3]. Despite the lower rate of mental illness, their risk of suicide from a mental illness is higher than the general population [4,5]. Fiske, et al. found that up to 80% of suicides in old age are linked to late-life depression [6].
Because of the high prevalence of mental health disorders, extensive research has investigated the several complex and interrelated factors that contribute to mental health disorders. Neighborhood conditions are some of these factors that contribute to the mental wellbeing of older adults [7,8]. Older adults are particularly at risk of developing poor interaction with their environment due to a decline in mobility and increased dependence [9]. Limitations in mobility in combination with higher cognitive and physical decline were associated with increased dependence on the neighborhood and its resources [10,11]. Since older adults spend a significant amount (about 75%) of their time relating with the neighborhood [12], they are more appreciative to the benefits and vulnerable to the harm of their immediate neighborhood [13].
Undoubtedly, the growing shift in the patterns of family dynamics results in non-readily available kinship ties and support [14]. Consequently, non-familial neighborhood social ties (NST), defined as "the presence of trusting relationships with individuals in one's community," are becoming an increasingly necessary source of social support in old age [15]. NST is a strong positive predictor of good mental health [16,17] and protective against depression and anxiety [18,19]. Importantly, the level of social ties determines the amount of social support received [20]. Therefore, older adults residing in neighborhoods with greater ties among residents may receive greater support than those in neighborhoods with lower social ties. While cross-sectional studies strongly associate lower neighborhood social cohesion (NSC) with higher depression and anxiety severity [21,22], the results of the longitudinal relationship between NSC and mental health factors remain inconclusive [23-26].
In addition to the quality of interpersonal relationships within one's neighborhood, neighborhood problems and perceived danger are also negatively correlated with mental health [27,28]. Neighborhood problems are the physical problems encountered within the neighborhood such as pollution, heavy traffic, noise, and overcrowding [29]. These problems in addition to perceived danger trigger fear and anxiety that may precipitate mental health problems [30]. Older adults living in neighborhoods with greater problems and perceived danger are not able to access necessary social resources which can lead to a decline in their reported well-being [31]. However, an improvement in the perception of the neighborhood in terms of safety may result in improvement in wellbeing.
Despite the culminating evidence on the association between neighborhood factors and mental health, most studies were conducted among adults and not the older adult population. With an increasing emphasis on the significance of aging-in-place among older adults, there is a need for studies that explore the impact that neighborhood social environment have on their mental health. Moreover, there is a need for a current national study to show the longitudinal association between neighborhood correlates and mental health in the literature of the aging population. As a result, implementing a longitudinal study design to examine the impact of neighborhood environment and mental health will give better insight into their relationships and add to the body of literature on the subject matter. This quantitative study was designed to investigate whether and which neighborhood factors predicted depression and anxiety among American older adults followed up for over five years within the same neighborhood.
Two waves of publicly available longitudinal data from the National Social Life, Health and Aging Project (NSHAP) which was accessed online from the Interuniversity Consortium for Political and Social Research [32] were utilized. The NSHAP is a nationwide survey that covers aspects of health and social connectedness of older adults across all ethnicities and gender in the United States. The first (Wave 1) interview period was between 2005 and 2006 while subsequent Waves were conducted five years apart. Face-to-face interviews using structured questionnaires were conducted, and bio-measures were taken at the respondent's home.
A national area probability sampling method was used to select community-residing adults based on the Health and Retirement Study's (HRS) national household screening method.
The HRS used a multi-stage area probability sample method with four selection stages. The HRS includes the selection of U.S. Metropolitan Statistical Areas (MSAs) and non-MSA Counties, i.e., include both urban and rural areas. A more detailed sampling method was described elsewhere [32,33]. A total of 3005 respondents were interviewed during the Wave 1 period. During the Wave 2 period, about 3400 interviews were completed where as a total of 4,777 respondents were interviewed for Wave 3. The Wave 1 interviews did not include the neighborhood correlates of interest to this study. Therefore, only the core datasets from both Waves 2 and 3 were used and only respondents that participated in both waves were used for this analysis. Wave 2 (Time 1 or T1) and Wave 3 (Time 2 or T2) data were merged after data cleaning into a horizontal format using the participant's assigned identification numbers. Following merging, we obtained a cohort of 2210 older adults from both Waves 2 and 3. However, we excluded all the participants who have lived within their neighborhood for less than 5 years at T2 using a variable assessing the length of residence within the neighborhood. This exclusion was done to ensure that people were already living within their neighborhood at T1, thus accounting for neighborhood factors at T1. Our final sample size was 1731 cohort of older adults as depicted in Figure 1.
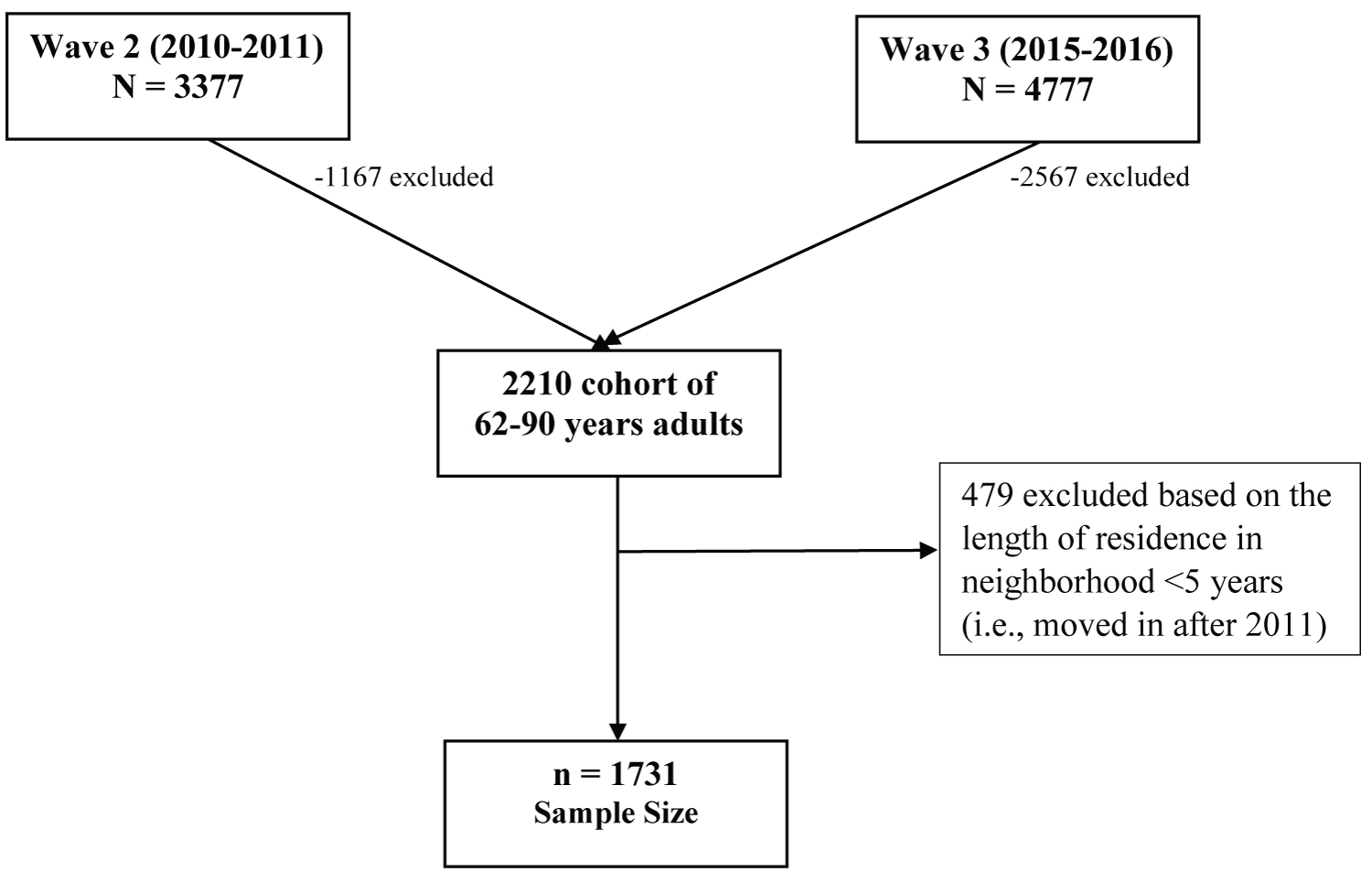 Figure 1: Flow chart for selection criteria and sample size. View Figure 1
Figure 1: Flow chart for selection criteria and sample size. View Figure 1
Outcome variables were two mental health constructs, depression and anxiety at T2 (Wave 3). Previously validated 11-item Center for Epidemiologic Studies Depression Scale (CES-D) and the 7-item Hospital Anxiety and Depression Scale (HADS) were used for depression and anxiety, respectively. These constructs' items were discussed extensively by Payne, et al. who reported internal consistencies of 0.78 and 0.73 for the CES-D and HADS scales, respectively [34]. The reliability scores for these scales for both Waves of data are reported in Table 1.
Table 1: Summary of variables. View Table 1
Predictors of mental health used in this study were four previously validated multi-item psychometric scales of neighborhood factors: Neighborhood social cohesion, social ties, and neighborhood probelms, rated from 1 to 5 as described in Table 1. Other covariates were demographic factors, self-rated physical health, and comorbidity index (CCI) described in Table 1 and below. The modified CCI [36] was used to calculate the comorbidity index (CCI) to control for other mortality risk factors and medical conditions that may affect health and cognition.
IBM SPSS statistical software v27.0 was used for all the data analytic procedures. Frequencies and percentages were used to describe categorical variables while means and standard deviations were used to describe continuous variables at both times. Next, chi-square and independent T-tests were used to compare differences between dichotomous and continuous variables at T1 and T2, respectively. We used a Hierarchical Multiple Regression to examine the relationship between neighborhood factors at T1 and depression as well as anxiety at T2. We had three models in total for each of the outcome variables. Model 1 contained the interaction between the neighborhood factors at T1 and outcome variables. Since depression and anxiety at T1 may act as a confounding factor, we controlled for depression and anxiety at T1 in model 2, for the depression and anxiety outcome variables, respectively. We finally introduced the demographic factors, physical health, and CCI as covariates in the third model.
Additionally, assumptions of normality of residuals and assumptions of no multicollinearity were checked before progressing with the multiple regressions. The assumption of normally distributed residuals was tested with QQ-plots and descriptive statistics while the assumption of multicollinearity was tested by calculating the variance inflation factor [37]. The quality of the multiple regressions was interpreted using the overall model effect size, R2 the statistical significance of the overall model, and the statistical significance of the individual regression coefficients. R2 is the variance explained effect sizes. We observed the changes in regression statistics in the relationship between neighborhood factors and depression as well as anxiety in the second and third models. All tests were two-sided and p-values less than 0.05 were considered to be statistically significant.
This nationally representative sample consists of older adults with a mean of 71.6 ± 6.6 years, who are mostly females (55.5%) and also in a marital relationship (71.9%). About 59% of them had at least some college education. The majority of the respondents were White non-Hispanic older adults. About a quarter of them earn above $50,000 but less than $100,000 annually at T1 and there was a statistically significant increase in income at T2. When asked about their physical health at T1, only 19.2% reported fair or poor health status and there was a significant report of poorer health at T2. The mean comorbidity index decreased significantly from 1.76 to 1.60 within the five years. Contrastingly depression increased significantly whereas anxiety scores remained the same after five years of living in the neighborhood. There was no statistically significant difference in the participants' reports of social cohesion and perceived danger within their neighborhood. However, problems within the neighborhood, as well as social ties, decreased significantly within the five-year period.
A normally distributed sample has a skewness of zero and deviation from normality occurs when skewness is > 1.98 (West, Finch, & Curran, 1996). Table 2 showed that the skewness of our outcome variable is within the normal range. Similarly, the VIF indicate no severe multicollinearity for any of the outcome variables.
Table 2: Selected descriptive statistics for residuals and VIF of outcome variables. View Table 2
All three models were statistically significant. The first model examining the relationships between the neighborhood factors and depression had a low variance explained, R2 = 2.8%. The variance explained by the predictors increased significantly by 25.6% after controlling for depression at T1 (Model 2). In model 3, adjusting for socio-demographic factors made the model better as R2 increased further by 4% (overall model = 32.5% of variance explained). In the first model in Table 3, PND was the strongest predictor of depression with β coefficient of 13.9%. That is, higher perceived danger within the neighborhood predicts a higher rate of depression. Conversely, NSC was significantly related to depression in the negative direction while the two remaining neighborhood factors did not predict depression after five years in this model. After controlling for depression at T2 in the second model, PND was the only significant predictor of depression, β = 0.055, p < 0.05. In this model, depression at T1 was the strongest predictor of depression at T2, β = 0.216, p < 0.001. In the third step, with the entry of demographic factors, CCI, and physical health in the equation, none of the neighborhood factors emerged as a significant predictor of depression. In this model, age, gender, ethnicity, marital status, physical health, and CCI significantly predicted depression, but depression at T1 remained the strongest predictor. A better self-report of physical health is associated with a lower risk of depression, β = -0.129, p < 0.05. In contrast, a unit increase in CCI score potentially increases the risk of depressive symptomology by 7.3%.
Table 3: Hierarchical multiple regression for the neighborhood paredictors of depression. View Table 3
In the hierarchical regression analysis for the neighborhood predictors of anxiety, all of the three models were statistically significant (Table 4). The first model explained only 3.7% of the variability in the outcome, anxiety at T2. Two neighborhood factors, NSC and neighborhood problems were significant negative predictors of anxiety. PND, on the other hand, was the strongest and positive predictor of anxiety, β = 0.154, p < 0.01. This indicates that a higher perception of danger within the neighborhood increases the risk of depression. With the addition of anxiety at T1, model 2, only PND and neighborhood problems emerged as significant neighborhood predictors of anxiety. Both predictors had equal β weights (0.048) but in opposite direction, such that a higher PND and lower NP predicts higher levels of anxiety among older adults. Additionally, anxiety at T1 strongly predicted anxiety at T2, indicating that the presence of anxiety at any point in time is the strongest risk factor for future anxiety symptomology. In this second model, we observed a significant rise in the variance explained by 23% (R2 = 0.267). Finally, adjusting for demographic factors, CCI, and physical health resulted in a significant and better model fit, F (13, 1710) = 50.76, p < 0.05, R2 = 0.278. However, NP was the only significant neighborhood predictor of anxiety, in the negative direction, β = -0.050, p < 0.05. As expected, anxiety symptoms at T1 also strongly predict anxiety at T2. Among the covariates adjusted for, only gender, ethnicity, and physical health were statistically significantly related to anxiety.
Table 4: Hierarchical multiple regression for the neighborhood predictors of anxiety. View Table 4
This study sought to investigate whether and which neighborhood factors predicted the mental health of older adults in America residence for five years within their community. Understanding the different neighborhood factors the mental health of older adults is crucial for healthy aging. Several measures of assessing the neighborhood context and the mental health status of older adults were included in the NSHAP study. According to previous research with the same NSHAP study data [35], four neighborhood correlates were conceptualized with high internal consistencies. The four correlates were NSC, social ties, neighborhood problems, and PND. Cross-sectional studies have highlighted how these neighborhood factors impact anxiety and depression, but only a few longitudinal studies have examined this relationship.
Based on previous studies, we expected that older adults with better social cohesion or social ties will be less anxious and depressed [38]. Conversely, those with more problems or perceived danger within their neighborhood will have poorer mental health outcomes [27]. Our results, however, suggest that PND and social cohesion were the only predictors of depression in the direction also indicated by previous studies [27,38]. Due to the longitudinal nature of this study, adjusting for baseline depression resulted in PND being the only significant predictor of depression, while social cohesion no longer predicted depression. Previous cross-sectional research also reported a significant relationship between social cohesion and depression [21]. Whereas longitudinal studies have mixed reports. For example, Fujiwara and Kawachi in their three-year longitudinal study reported a higher level of depression with lower levels of social cohesion after adjusting for baseline depression [24]. On the other hand, Mair, et al. found no association between social cohesion and depression in their 4-5 years follow-up study [26].
According to Lorenc, et al. and Doran and Burgess, the perception of danger within one's immediate community fosters fear and mistrust that produces increased levels of psychological distress such as depression and anxiety [37,39]. It is noteworthy that despite the statistically significant relationship between depression and PND, as well as NSC, before adjusting for baseline depression, the predictors explained only 2.8% of the variance in depression. That is, other factors beyond the neighborhood social environment may have a stronger influence on depression. In our study, some of these factors included age, gender, ethnicity, marital status, comorbidities, and physical health status.
The addition of baseline depression and other sociodemographic and physical health characteristics and the subsequent increase in the R2 to 32.6% supported this observation. In fact, none of the neighborhood factors were significant predictors of depression after adjusting for these covariates. In contrast to cross-sectional study findings, some longitudinal study designs also did not report a significant relationship between neighborhood factors and depression after three to five years of follow-up [26,40,41]. The findings in these longitudinal studies were similar to those observed in this study. However, a longitudinal study examined this relationship and reported that social cohesion reduced the negative change in mental health caused by living in a deprived neighborhood after seven years [25]. Interestingly, another ten-year follow-up study also observed a significant increase in common mental disorders such as depression in adults living in more deprived neighborhoods [22]. Clearly, the studies with longer follow-up periods reported a significant relationship between neighborhood factors and mental health, whereas those with follow-up within five years or less reported no significant relationship. We can, therefore, assume that a significant change in mental health may only occur after prolonged interaction with one's neighborhood.
In our study, baseline depression was the strongest determinant of depression following five-year, followed by self-rated physical health. Previous research findings support an age-associated rise in negative affect or increased depression in older adults [42], which may explain why baseline depressive symptoms strongly influence depression in later years. Furthermore, the effect of physical health on the relationship between neighborhood factors and depression cannot be overemphasized because older adults rely on the relationships in their neighborhood which may be adversely affected by poor physical health which may subsequently result in higher mental disorders. Previous research also indicates that physical health has a strong impact on mental health and vice versa and this effect are especially more prominent with advanced age [43]. Besides, an older adult's physical health determines their ability to interact with their neighborhood. Therefore, older adults who rely on their neighborhood for various resources may report higher mental disorders particularly when they have poor physical functioning.
Consistent with other studies, lower NSC and a higher PND were associated with higher anxiety symptoms among older adults [21,22]. Surprisingly, however, higher neighborhood problems predicted lower anxiety levels in our study. We expected that physical problems encountered within the neighborhood such as pollution, heavy traffic, noise, or overcrowding to cause a higher level of anxiety within the neighborhood [29,30]. The contrasting relationship observed in our study could be due to the significant decrease in the neighborhood problem scores from baseline to T2 (Table 5). Since the older adults reported the neighborhood that they live in to have fewer problems after five years, it is understandable why their levels of anxiety may decrease as well. After controlling for baseline anxiety levels, only PND and NP were significantly associated with anxiety. In this case, a higher PND and lower NP predicts higher anxiety symptomology.
Table 5: Characteristics of the participants. View Table 5
In our third model, we controlled for demographic and physical characteristics and baseline anxiety levels (Table 3). In this model, only NP emerged as the only significant predictor of anxiety, however, still in the negative direction. This finding still contradicts evidence from previous research that established how built environment or the amount of physical disorder in a neighborhood negatively impacts people's ability to focus or sleep thereby causing substantial anxiety. Despite the negative impact of neighborhood problems on the development of stress and anxiety, Pudrovska, et al. highlighted how mastery of the said problems within the neighborhood may moderate these relationships [44]. The extent to which the respondents perceived the events or problems within their neighborhood that is their control, also called mastery, could also explain why their rating of neighborhood problems was lower after five years.
Similar to depression, baseline anxiety level was the strongest predictor of anxiety levels after five years after controlling for other factors as seen in Table 4. This is despite the non-significant change in anxiety levels within five years (Table 5). Sami and Nilforooshan also reported baseline anxiety to be a considerable prognostic factor for future anxiety in a six-year follow-up study [45]. Additionally, we found that physical health influenced anxiety levels, such that a unit increase in physical health rating in the positive direction lowers the risk of anxiety symptoms by 7.9%. Older adults without functional limitations can explore the resources within their immediate community leading to lower rates of psychosocial problems.
This study has some limitations. First, secondary data was used which constrained the variables of interest. For instance, we were unable to account for the social and regional characteristics of the respondents which may contribute to the covariates explaining most of the variance in anxiety and depression in our study. Second, longitudinal studies require more than two data points for best practices to assert causality. However, this study utilized only two waves of data with two-time points. Therefore, despite the associations claimed in this study, causal inference cannot be established. Third, considering the significant association between baseline depression/anxiety and anxiety and depression at T2, we were unable to ascertain if the participants have received a clinical diagnosis of these mental disorders or on medical treatment for them.
From this study, we conclude that after adjusting for other covariates, neighborhood factors do not predict the development of depression among older adults in America who have lived in their present communities for at least five years. However, neighborhood problems significantly influence anxiety among this population even after adjusting for other covariates. We also established the significant impact of physical health on mental health among community-dwelling older adults. Our findings suggest that city planners and policymakers can influence healthy aging through the proper mapping of a city and the reduction in disorderliness within communities for older adults. Therefore, future policy development and interventions should target improving both physical and social environments to enhancing the mental wellbeing of older adults.
The authors declare that they have no competing interests.
No funding was received for this study.
All the authors contributed equally in the preparation of this study.