To assess the diagnostic accuracy of geriatrician-performed point-of-care ultrasound (PoCUS) on suspicion of deep venous thrombosis (DVT) in geriatric inpatients by comparing findings to a radiologist/specialist performed ultrasound as reference.
This study was conducted as a single-center feasibility study. Patients with suspicion of deep venous thrombosis defined as Well's score of 0-1 with a concomitant elevated D-dimer or a Well's score ≥ 2 regardless of D-dimer were eligible for inclusion. In addition, the following inclusion criteria were met: 1) ≥ 65 years, and 2) presence of ≥ 2 diseases. No current DVT diagnosis or targeted treatment against DVT. Patients first underwent ultrasound examination by a geriatrician and subsequently by a blinded radiologist.
A total of 29 (19 women) patients were included. The prevalence of DVT was 3.4%. Analysis of the diagnostic accuracy revealed a sensitivity of 100 (2.5-100), and a specificity of 96.4 (81.7-99.9). Positive predictive value was 50.0 (12.8-87.3) and negative predictive value of 100 (100-100), with an overall diagnostic accuracy of 96.5 (82.2-99.9). χ2-test revealed a non-significant difference in Geriatrician-performed PoCUS and Radiologist-performed ultrasound.
Our results suggest a promising diagnostic accuracy of Geriatrician-performed PoCUSfor the examination of deep venous thrombosis which should be further assessed by adequately powered studies. PoCUS, as a tool for clinical examination, could be a great fit for examining geriatric inpatients bedside in a patient-centered and safe environment.
Point-of-care ultrasound, Ultrasound, Deep venous thrombosis, Geriatric
• Point-of-care ultrasound is a safe and patient-centered clinical tool for examining geriatric inpatients
• Point-of-care ultrasound show a high diagnostic accuracy when examining geriatric patients for the presence of DVT
• Point-of-care ultrasound offers shielding of frail patients from unnecessary exposure of stressors, thus a great fit for clinical examination of geriatric inpatients
Deep venous thrombosis (DVT) is a common condition in patients ≥ 80 years of age, with an estimated prevalence of 1/100 in Denmark [1]. Several studies have estimated a prevalence lower extremity DVT of 15% in geriatric patients aged > 70 years admitted to the emergency department [2,3]. Typical symptoms encompass swollen/painful leg(s), tenderness along the deep veins, superficial venous configuration, and pitting edema [4]. For assessment of pre-test probability, clinical scores such as Well's score (Table 1) in addition to measurement of D-dimer are commonly utilized as recommended by The European Society of Cardiology [5,6].
Table 1: Wells score. View Table 1
The primary and chief life-threatening complication of DVT is pulmonary embolism (PE), which occurs when a DVT dislodges from its site of origin and travels to the pulmonary vasculature, obstructing blood flow. Multiple studies have reported a presence of residual deep venous thrombotic material in approximately 50% of patients with PE [7-9]. In these cases, an undetected residual DVT may aggravate an already potentially life-threatening condition by dislodging and migrating to the already embolized pulmonary vessels, further adding to the occlusion [10]. Aside from complications like PE, nearly half of patients with DVT develop post-thrombotic syndrome (PTS). This condition arises due to venous valvular incompetence and venous hypertension as a result of thrombotic obstruction, manifesting as symptoms such as swelling, cramping, itching, and pain [11].
Point-of-care ultrasound (PoCUS) is a safe, non-invasive, and patient-centered bedside method for assessing and diagnosing various conditions including DVT [12,13]. With an evidence-based education and continuous supervised training, PoCUS has been shown to enhance clinical decision-making [14,15]. This makes it ideal for examining geriatric patients suspected of critical illness, which are among the most frequent users of the healthcare system in the western world [16,17]. As disease presentation is often atypical in the geriatric patient, the clinician must be able to interpret clinical information while considering that these patients are hallmarked by: 1) Vague symptoms, 2) A decreased ability to explain symptoms, 3) A decreasing cognition, and 4) A decreasing physical function [18].
These circumstances often complicate assessment of pre-test probability of present DVT. As such, ultrasound investigations performed by the geriatrician could save both time for the clinician and of even greater importance alleviate the need for transporting a potentially frail geriatric patient to another ward, thereby avoiding the unnecessary exposure of potential stressor, hence lowering the risk of delirium.
In recent years, several studies have emerged which evaluates PoCUS protocols, performed by surgeons who underwent a training course in US technics, physics, anatomy and hands-on training under supervision, in comparison with radiologist performed ultrasound. These studies showed an accuracy of 94% in detecting gallstones, an accuracy of 93.3% in detecting acute cholecystitis, and an accuracy of 77.3% in detecting appendicitis [19,20]. However, to our knowledge, no study has evaluated the diagnostic accuracy of geriatrician-performed PoCUS in regards to lower extremity DVT occurrence, in comparison with radiologist-performed ultrasound.
To assess the clinical utility of geriatrician performed deep venous ultrasound, this study aims to approximate the diagnostic accuracy of geriatrician-performed PoCUS on suspicion of deep venous thrombosis in geriatric inpatients by comparing findings to a radiologist/specialist performed ultrasound as reference test.
The study was a quality assurance project, which entails that no personal data were collected that could identify participating patients. The authors made inquiries to the local ethics committee and no formal approval from the committee was required (ID: S-20212000-18 Acadre 21/209). All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions.
Informed consent was obtained from all patients for being included in the study.
This study was carried out as a single center feasibility study at Svendborg Hospital, Region of Southern Denmark, Denmark. The hospital is the second largest referral center, covering the southern part of the region of Funen, with an annual emergency census of approximately 1400 geriatric patients. Following initial diagnostic and clinical work-up in the emergency department, geriatric patients are referred to the department of geriatrics for further treatment.
Geriatric patients with clinical suspicion of DVT in lower extremities, exhibiting either a Well's score of 0-1 with a concomitant elevated D-dimer or a Well's score ≥ 2 regardless of D-dimer were eligible for inclusion if they fulfilled the following inclusion criteria:
1) Geriatric patients referred to the department of geriatrics defined as: 1) aged ≥ 65 years, and 2) presence of ≥ 2 diseases (multimorbidity).
2) One of the following symptoms: Uni- and/or bilateral swollen leg, pain, increased venous prominence, and/or edema.
3) No recent prior DVT diagnostics (6 months) upon hospital admission.
4) No current DVT diagnosis or targeted treatment against DVT.
Further, in accordance with Danish legislation, patients suffering from cognitive impairment were also not eligible.
Patients meeting the inclusion criteria would undergo extended compression ultrasound (ECUS) by one of two geriatricians certified in PoCUS by an educated instructor with several years of teaching and experience in PoCUS-research. Subsequently, the patients were referred to the department of radiology, where they were subject to a complete duplex ultrasound scan (CDUS) performed by a physician employed in the ultrasound section as a reference standard. The investigating physicians at the department of radiology were blinded to geriatrician findings and were only provided information regarding which extremity to scan. In case of DVT found by ECUS, patients would immediately receive treatment according to hospital guidelines (e.g., either treatment with Dalteparin (low molecular weight heparin) or direct oral anticoagulants).
According to a recent report published in Circulation, a journal under the American Heart Association (AHA), for PoCUS examination for DVT, the extended compression ultrasound (ECUS) scan is favored over the frequently used 2-point compression ultrasound (2-CUS) scan [12].
With the patient in the supine position, the examined leg slightly rotated externally, and with a gentle flexion of the knee, ECUS was performed by compressing the deep veins, starting with the common femoral vein (Figure 1), and compressing for every centimeter, continuing just proximal to the division of the popliteal vein (Figure 2). The linear transducer (3-12 MHZ linear transducer, GE Venue) was used for the examination and was placed transversely, perpendicular throughout the examination [12].
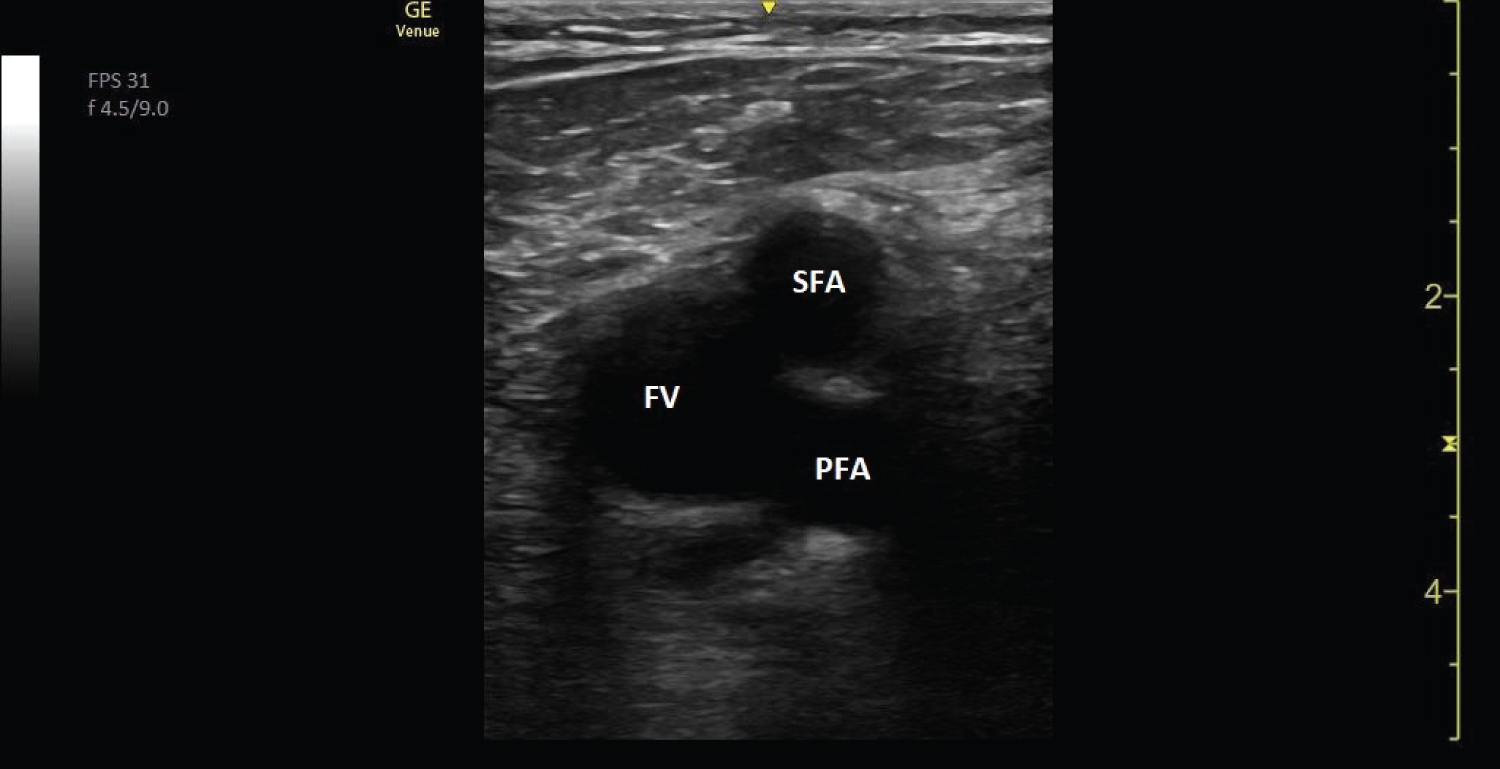 Figure 1: Ultrasound image showing the left femoral vein (FV) and the superficial (SFA) and profound (PFA) femoral artery.
View Figure 1
Figure 1: Ultrasound image showing the left femoral vein (FV) and the superficial (SFA) and profound (PFA) femoral artery.
View Figure 1
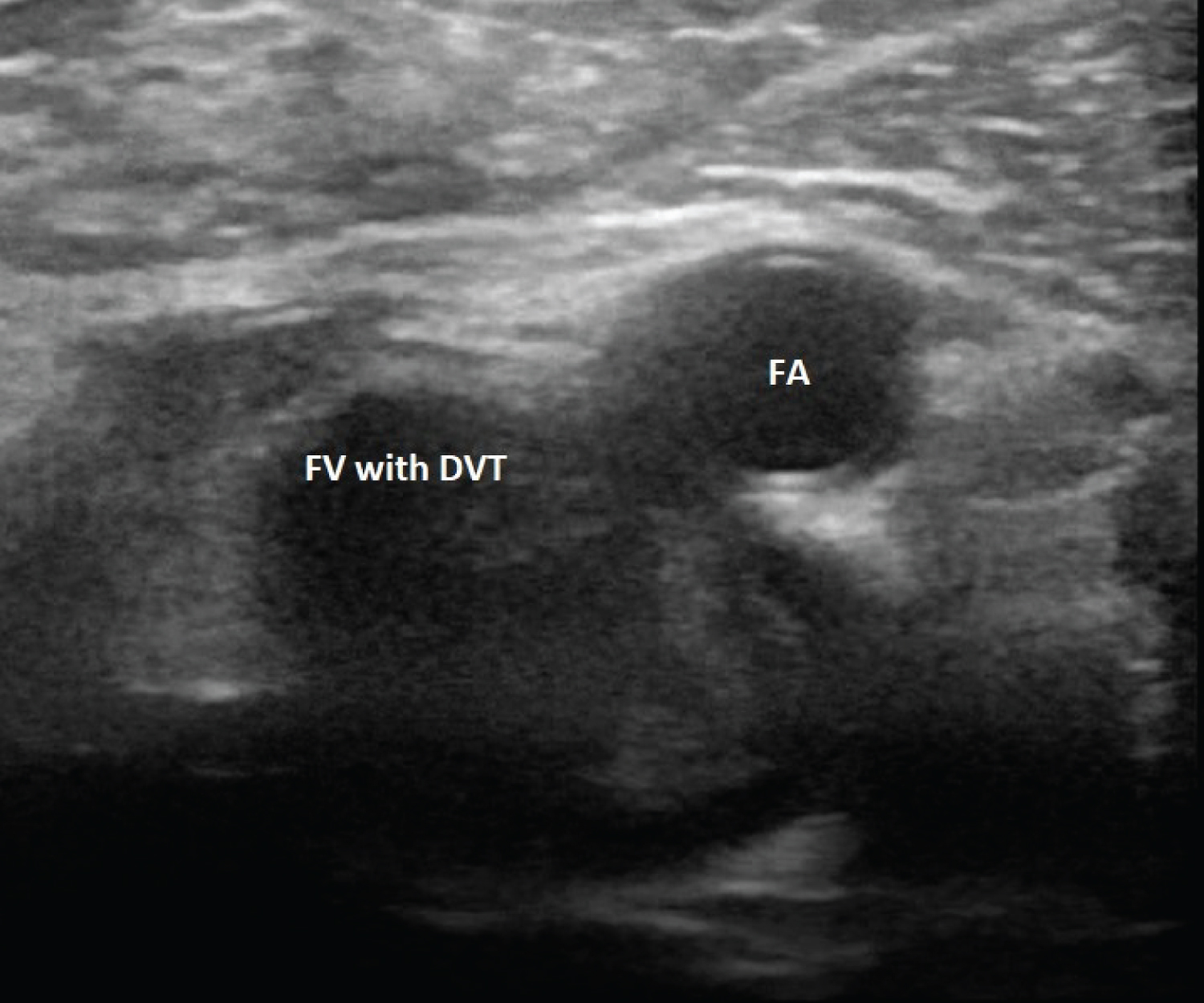 Figure 2: Ultrasound image showing the left femoral vein (FV) containing thrombosis and the femoral artery (FA).
View Figure 2
Figure 2: Ultrasound image showing the left femoral vein (FV) containing thrombosis and the femoral artery (FA).
View Figure 2
The deep veins were examined from the groin and as far down the lower extremity as possible by using the linear transducer. The patient was first positioned in the supine position with a slight external rotation of the hip. First, the common femoral vein both above and below the inguinal ligament and the sapheno-femoral junction was examined. For examination of the popliteal vein and the crural veins the patient was placed in the lateral decubitus position, or prone with a pillow under their ankles. Hereby, exposing the popliteal vein to examination of the posterior tibial and peroneal veins as far distally as possible were examined. If it was possible to identify the anterior tibial veins these were examined as well. During the whole examination compression and color Doppler were applied along the veins to evaluate the presence of DVT.
Because the ECUS protocol does not include the crural part of the lower extremity, the department of radiology noted if the patients had DVT according to the area included by the ECUS and/or DVT in the region not included by the ECUS.
In case of divergence in DVT-diagnosis, defined as the presence of DVT in a patient by geriatrician-performed ECUS but absence of DVT in the same patient by CDUS, patients were offered a new scan 5-7 days after their latest scan, to evaluate if a DVT was present. As the department of radiology was the reference standard, patients would not receive treatment prior to the additional CDUS.
The prevalence of DVT among geriatric patients varies immensely, in general and according to the clinical setting. For example, as a part of a focused examination during admission to the emergency department [3], or as a coincidently finding at a geriatric department. Thus, a valid expected prevalence of DVT among geriatric inpatients as usage for power-calculation was challenging to estimate. There for it was decided to include all inpatients suspected for DVT over the course of a year.
All statistical analyses were performed in GraphPad Prism 9.0.0. (GraphPad Software, San Diego, California USA). Diagnostic accuracy of geriatrician performed ultrasound was assessed through calculation of sensitivity and specificity, positive and negative predictive values as well as accuracy. 95% confidence intervals were calculated as Clopper-Pearson intervals [21]. Normality was assessed using the Shapiro-Wilk test [22]. Normally distributed data are presented as mean ± SD. Non-normally distributed data are presented as median with interquartile range (IQR). χ2-test was performed to assess differences in diagnosing DVT and non-DVT patients between Geriatrician-performed PoCUS and Radiologist-performed ultrasound. A P-value below 0.05 was considered statistically significant.
A total of 29 patients (19 women) were included in the study. Demographic baseline characteristics are listed in Table 2. Median age was 85.3 years and body composition measures revealed mean BMI of 29.2 ± 6.4 kg/m^2. Median Charlson Comorbidity Index (CCI)-score of 4 (IQR: 2-5.5). Median Well's score was1 (IQR: 0-2) with a median D-dimer of 2.0 mg/L (IQR: 1.1-5.0). A median of 4 admission days (IQR: 2-6) went by before patients received their initial ultrasound scan. Five patients were admitted with erysipelas, six patients were admitted with other infections (pneumonia, urinary tract infections unspecified bacterial infection), four patients with unspecified oedema, two patients were admitted with traumatic muscle ischemia after falling. Other diagnoses upon admission are listed in Table 2.
Table 2: Baseline characteristics. View Table 2
The prevalence of DVT was 3.4% (1/29). Analysis of diagnostic accuracy regarding Geriatrician-performed PoCUS, as listed in Table 3, revealed a sensitivity of 100 (2.5-100), and a specificity of 96.4 (81.7-99.9). Positive predictive value was 50.0 (12.8-87.3) and negative predictive value was100 (100-100), yielding an overall diagnostic accuracy of 96.5 (82.2-99.9). Geriatrician-performed PoCUS revealed 1 true positive, 1 false positive, 0 false negatives and 27 true negatives patients. A χ2-test was performed to examine differences in DVT and non-DVT patients when patients underwent Geriatrician-performed PoCUS and Radiologist-performed ultrasound. χ2-test revealed a p-value of 0.5532, thereby showing a non-significant difference.
Table 3: Diagnostic accuracy. View Table 3
To our knowledge this is the first study comparing Geriatrician-performed PoCUS with ultrasound performed by radiologists. Our results showed a non-significant difference between Geriatrician-performed PoCUS and Radiologist-performed ultrasound in diagnosing patients with or without DVT. Furthermore, a specificity of 96.4% and a promising diagnostic accuracy of Geriatrician-performed PoCUS of 96.5%. These findings suggest that geriatrician-performed PoCUS, as a tool for clinical examination, could be a great fit for examining geriatric inpatients bedside in a patient-centered and safe environment. Because PoCUS allows for a patient-centered approach and potentially could be performed by the same physician who initially sees the patient, it is not only a patient-friendly method but also a time saving method that shields the potentially frail patient from unnecessary exposure of stressors.
However, this study has some limitation which should be considered when interpreting the results. First, the prevalence of DVT was lower than previously reported [3]. Several factors could have contributed to this. One factor is the high presence of atrial fibrillation (AFLI) among the studied population (data not shown) and the corresponding treatment with direct oral anticoagulants (DOAC) such as Rivaroxaban and Apixaban. These medications are also the recommended treatment for DVT [23], and although the indication for treatment was not DVT but thromboprophylaxis in AFLI, there is a great probability that it did affect the results. However, the prevalence of DVT among geriatric patients might still be high despite prophylactic treatment with anticoagulants [3]. Second, in the hospital where the study was performed, geriatric patients are not directly admitted to the department of geriatrics but admitted to the department of emergency medicine and after initial diagnosis then referred to the department of geriatrics. This could influence the overall prevalence of DVT among geriatric patients since potential patients with DVT would not be seen by a geriatrician but rather referred to the outpatient clinic of cardiology for further diagnosis and treatment. Third, the median Well's score among the studied population was 1 (IQR: 0-2), hence the risk of DVT low, and therefore the portion of patents with a low risk of DVT high, and thereby a potential confounder.
As such, further large-scale studies are warranted to confirm the promising use of geriatrician-performed PoCUS for the detection of DVT. The limited but promising diagnostic accuracy of 96.5% in this study could be an impetus for a movement in geriatric medicine for enhancing the use of PoCUS among geriatricians, given sufficient supervision and after undergoing a certified education program.
The authors would like to acknowledge Open Patient data Explorative Network (OPEN) at Odense University Hospital, for their support during this project.
None declared.
This project did not receive funding of any kind.
All authors participated equally in the conduct of this study.