Background and aim: Hospital maintenance engineers are heterogeneous group of workers responsible for a wide variety of duties including maintaining equipment, heaters, refrigerators, air-conditioners and ventilation systems, and they are susceptible to adverse health hazards. This study was aimed to characterize and correlate psychological impairment, pain severity and Work-Related Musculoskeletal Disorders (WMSDs) among hospital maintenance engineers in a Nigerian tertiary hospital.
Methods: A total of 111 (76.6% response rate) hospital maintenance engineers responded in this cross-sectional survey. Standardized Nordic Questionnaire, a 100-mm horizontal Visual Analogue Scale for Pain (VAS Pain) and the Depression, Anxiety and Stress Scale (DASS-21) were used to assess WMSDs, pain intensity and psychological impairment (depression, anxiety and stress) respectively. Descriptive statistics of mean and standard deviation and percentages were used to summarize data. Bivariate tests of relationship/association and multivariate regression analyses were employed. Alpha level was set at p < 0.05.
Results: The 12-month and 7-day prevalence of WMSDs were 71.8% and 42.7%. The point prevalence rates of depression, anxiety and stress were 30.1%, 29.1% and 20.4% respectively. The highest 12-month pain severity was recorded in the hip/thigh (54.8 mm) and lower back (49.3 mm) regions while the highest present (7-day) pain severity was in the neck (65.6 mm) and shoulder (64.6 mm) regions. Presence of depressive symptoms increased the odds of having WMSD (Odd ratio (OR) = 1.04; (95% Confidence Interval (CI) = 1.09-1.69; p = 0.019) and specifically, the incidences of shoulder (OR = 1.09; CI = 0.98-1.21; p = 0.049) and upper back (OR = 1.18; CI = 1.03-1.34; p = 0.015) WMSDs. Anxiety and stress symptoms were not associated with presence of any WMSD among the respondents (p > 0.05). Respondents with higher score of depression had significant correlation with higher pain severity in the shoulder (r = 0.21; p = 0.014), lower back (r = 0.25; 0.010), knee (r = 0.25; p = 0.012) and ankle/feet (r = 0.21; p = 0.030) regions in the past year. Similarly, higher score of anxiety and stress symptoms were significantly correlated with higher pain severity in the neck, shoulder, ankle/feet, knee and lower back (r ≥ 0.21; p < 0.05).
Conclusion: There is a high prevalence of WMSDs among hospital maintenance engineers and it is significantly associated with depressive, anxiety and stress symptoms.
Depression, Anxiety, Stress, Engineering staff, Health workers, Nigeria
Work-related musculoskeletal disorders (WMSDs) are impairments of the musculoskeletal system caused or aggravated primarily by work itself or by the environment in which work is performed [1]. They are considered as the most important cause of occupational injury and disability in the world and the main cause of absenteeism at work [2]. According to the National Institute for Occupational Safety and Health (NIOSH), there exist a causal relationship between physical exertion at work and work-related musculoskeletal disorders (WMSDs) [3]. Worldwide, data have shown that WMSDs account for 42%–58% of all work-related illnesses [4,5] and 40% of all work-related health costs [5]. In Nigeria, the prevalence of WMSDs varies among different occupational groups; the prevalence is 91.3% among physiotherapists [6], 78% among nurses [7], and oscillates between 64.4% [8] and 71.9% [9] among Nigerian health workers generally.
Clinical and epidemiological studies indicate that musculoskeletal disorders could be the manifestations of psychological problems [10-12]. Studies have also characterized pattern of WMSDs with the influence of psychological health showing a significant association between WMSDs and psychological health among health workers [11,13,14]. A systematic review has provided evidence that depressive symptoms, for instance, are associated with higher levels of pain intensity, and poor outcome in the management of musculoskeletal disorders [10].
Alleviating the incidence of WMSDs seems intractable because more focus have been placed on the biomechanical risk factors and physical work stressors (repetitive movements, excessive force and awkward postures) and almost neglecting the psychological risk factors which are one of the main factors for developing WMSDs [12,15-18]. The psychosocial model of managing WMSDs has been proven as a valid means of reducing the incidence of WMSDs indicating that alleviating psychological health disorders among workers may lessen the burden of WMSDs [12,18-20]. Gusti, et al. [12] had indicated that outcome of rehabilitation of musculoskeletal disorders may be unsatisfactory without addressing the effects of psychological health problems. Unfortunately, mental health problems have been observed to be under-reported, under-diagnosed and under-treated in developing countries such as Nigeria [21,22]. Epidemiological data on psychological health of the Nigerian populace have an estimated 20-30% suffering from mental disorders [23] while another study reported that about 38.5% of the Nigerian health workers have one form of psychiatry illness [24].
There are few studies on the influence of psychological risk factors on WMSDs in developing countries such as Nigeria. It has been suggested that studies investigating the relationship between psychological factors and WMSDs should be undertaken in developing countries to deepen the understanding of the phenomenon [18,25-27]. Understanding the contribution of psychological problems in the incidence of WMSDs may help in introducing more efficient workplace interventions such as health, training and safety policies that could minimize these problems. Although health workers are reported to be at a high risk of WMSDs, it is one of the least-studied occupation groups [28] and it appears that most of the studies on WMSDs among health workers are concentrated on the clinicians, whereas non-clinical hospital workers also face work demands, working conditions and activities that made them susceptible to developing WMSDs [29]. For example, engineering staff in Nigerian hospital environment have been reported to render services in uncomfortable positions and regularly employ manual and crude appliances including using of forceful exertion in order to execute their functions [9]. This study was aimed to characterize and correlate psychological impairment, pain severity and Work-Related Musculoskeletal Disorders (WMSDs) among hospital maintenance engineers in a Nigerian tertiary hospital.
In this cross-sectional study, 145 hospital maintenance engineers at the Osun State University Teaching Hospital, Osogbo, Nigeria were invited. However, 111 surveys were returned yielding a 76.6% response rate. Only 103 of the returned questionnaires were found valid to be used in the final analysis. Eligible respondents were those who had been in the employment of the hospital for no less than one year preceding this study. However, workers with apparent physical deformities, positive history of major trauma, degenerative disc diseases, spondylitis, and benign and/or malignant tumor, and those with previous spinal surgery or musculoskeletal injuries were excluded from the study.
Ethical approval for the study was obtained from Research Ethics Committee of the Osun State University Teaching Hospital, Osogbo, Nigeria (Ref: LTH/EC/2021/01/496). The purpose of the study was explained to the respondents and their written informed consent was obtained. A four-section questionnaire was used as the survey instrument. Section A, a self-developed proforma, was used to seek information on the socio-demographic (age, gender, marital status, educational level, alcohol consumption, cigarette smoking and regular habits of physical activity) and work (job tenure, job type, job status, job level, and working posture) characteristics.
The section B, modified standardized Nordic questionnaire, which is a valid instrument in assessing work-related musculoskeletal dysfunction [7,30,31] was employed. This questionnaire consists of questions on symptoms of pain/discomfort in the last 12 months/7 days referring to nine body areas (Neck, shoulders, upper back, lower back, elbows, wrists/hands/thumb, Hips/thighs, knees, ankles/feet) and respondents were required to answer "yes" or "no" to any of the complaints in any body area(s). Section C- 100 mm (10 cm) horizontal visual analogue scale for Pain (VAS Pain), was used to assess pain intensity. The pain VAS is a uni-dimensional pain rating scale that has continuum of value measurement of pain intensity. The simplest form of pain VAS, used in this study, was a straight horizontal fixed line of 100mm measured from left (no pain) to the right (worst pain). The pain VAS score was assessed by measuring (with a metre-rule) in millimeters from the left side of the line to point that the respondent marks [32], with higher score indicates greater pain. Score of 0-4 mm was considered no pain, 5-44 mm mild pain, 45-74 mm moderate pain and 75-100 as severe pain [33]. Since WMSDs are most often expressed in pain by the sufferers, respondents were asked to rate/mark their pain severity in the last 12 months/7 days in the body area(s) of complaint or discomfort by using 100 mm (10 cm) horizontal visual analogue scale for Pain (VAS Pain) placed below each of the body area on Nordic questionnaire. Section D containing Depression, Anxiety and Stress Scales - 21 Items (DASS-21) was used to assess the psychological health (depression, anxiety and stress) of the respondents. The psychometric properties of DASS have been found to be suitable in identifying depression, anxiety and stress in occupational health care setting [34]. DASS-21, which is the short form of DASS-42 with 21 items, is a set of three self-report scales designed to measure the negative emotional states of depression, anxiety and stress. The respondents were asked to score every item on a scale from 0 (did not apply to me at all) to 3 (applied to me very much). The sum scores were computed by adding up the scores on the items per subscale and were doubled to be equivalent to the longer DASS-42 version. Sum scores for each of the subscales range between 0 and 42. DASS score greater than 9, 7 and 14 were considered as positive caseness of depression, anxiety and stress respectively. DASS score of 10-13, 14-20, 21-27 and ≥ 28 were classified as mild, moderate, severe and extremely severe depression while score of 8-9, 10-14, 15-19 and ≥ 20 were classified as mild, moderate, severe and extremely severe anxiety. Also, DASS score of 15-18, 19-25, 26-33 and ≥ 34 were considered as mild, moderate, severe and extremely severe stress [35,36].
Data obtained was summarized in mean, standard deviation, frequency and percentage. Logistic regression analysis expressed in Odd ratios (ORs) and 95% Confidence Interval (95% CI) was used in determining the relative risk of psychological factors causing WMSD in any of the nine body parts while Chi-square was used to evaluate the association between the prevalence of WMSD and selected socio-demographic variables. Respondents with WMSD in four or more body parts were classified as having multiple WMSD according to Parkes, et al. [29]. Upper body WMSD was defined as having WMSDs in neck, shoulder and upper back together and as upper extremity WMSD if found in elbow and hand/wrist together. Lower extremity WMSD was defined as having WMSDs in the knee and ankle/feet together [29]. Logistic regression was also used to determine the predictors of WMSDs and factors responsible for consultation with health care professional for the symptoms of WMSDs.
Spearman's correlation was used to determine the relationships among pain and WMSDs, and psychological factors. Alpha level was set at p < 0.05. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp. was used for the analysis.
The mean age of the respondents was 45 ± 7.70 years. Most of the respondents in this study were men (67%), 97.1% were married, 55.3% had tertiary education, 33% had consumed alcohol and 57.3% of them reported to regularly engage in physical activity. 42.7% of the respondents had worked in their current job between 6-10 years. 60.2% of the respondents had their work schedule described as being strenuous. 48.5% of the respondents assumed body posture of standing and bending while working (Table 1). Table 2 shows the results on prevalence and level of depressive, anxiety and stress symptoms of the respondents. The prevalence of depression, anxiety and stress were 30.1%, 29.1% and 20.4% respectively. Most of the respondents had moderate depression (16.5%) and anxiety (17.5%) while mild caseness of stress (10.7%) was mostly prevalent among these staffs.
Table 1: General characteristics of the respondents (N = 103). View Table 1
Table 2: Prevalence and level of depression, anxiety and stress symptoms among the respondents (N = 103). View Table 2
The 12-month and 7-day prevalence of WMSDs were 71.8% and 42.7%. The three most affected body parts in the past year were lower back (46.6%), shoulder (30.1%) and knee (25.2%) while lower back (28.2%), ankle/feet (10.7%) and shoulder and knee (9.7%) were mostly affected in the past week. Hip/thigh (54.8 mm), lower back (49.3 mm) and upper back (49.0 mm) were the 3 anatomic sites with highest pain severity in the past year and neck (65.6 mm), shoulder (64.6 mm) and wrist/hand (60.4 mm) in the past week (Table 3). Table 3 also shows the 12-month and 7-day prevalence rates for the multiple, upper body, upper and lower extremities WMSDs. Also, Figure 1 illustrates the frequency of the number of sites wherein the respondents experienced WMSDs in the past year. About a quarter of the respondents (24.3%) had WMSDs in four or more parts of the body in the past year. From Table 3, annual prevalence of WMSDs in upper body and lower extremity was 8% respectively, which is relatively low compared to the annual prevalence of WMSDs affecting the lower back (46.6%). Only 39.2% of those who reported WMSDs sought interventions from healthcare professionals (HCP). Logistic regression analysis results indicate that respondents with WMSD affecting the lower back were more likely to consult HCP than for any other WMSD (OR = 3.70; CI = 0.92-14.23; p = 0.049). Presence of other WMSDs and psychological impairments were not associated with consultation to HCP (p > 0.05). Furthermore, WMSDs affected work (34.4%) and leisure (29.7%) of the respondents (Table 4a and Table 4b).
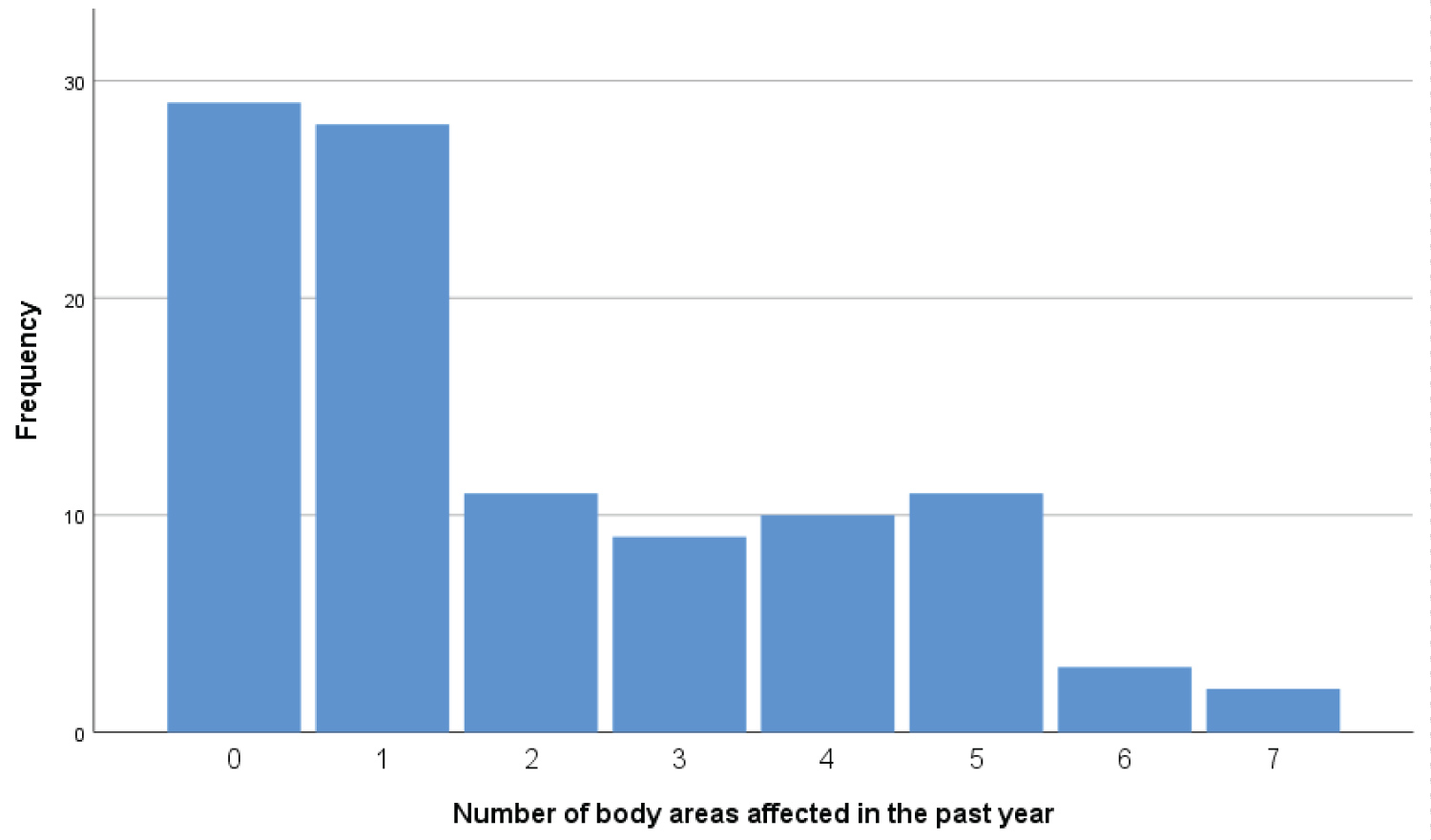 Figure 1: Bar chat of number of areas affected in the past year.
View Figure 1
Figure 1: Bar chat of number of areas affected in the past year.
View Figure 1
Table 3: Prevalence and severity of Work-related musculoskeletal disorders/pain in the past year and past week (N = 103). View Table 3
Table 4a: Factors associated with consultation to healthcare professionals due to work-related musculoskeletal disorders. View Table 4a
Table 4b: Factors associated with consultation to healthcare professionals due to work-related musculoskeletal disorders. View Table 4b
The results of logistic regression shows that reporting positive for depressive symptoms was associated with annual prevalence of WMSDs (OR = 1.04; CI = 1.09-1.69; p = 0.019) and specifically, the WMSD affecting the shoulder (OR = 1.09; CI = 0.98-1.21; p = 0.049) and upper back (OR = 1.18; CI = 1.03-1.34; p = 0.015). Anxiety and stress symptoms were not associated with incidence of any WMSD (p > 0.05) (Table 5).
Table 5: Associations of depressive, anxiety and stress symptoms with the annual prevalence of work-related musculoskeletal disorders. View Table 5
Prevalence of WMSDs affecting the shoulder was associated with male gender (p = 0.022), higher level of education (p = 0.046) and being locum staff (p = 0.027), while prevalence of WMSDs affecting the lower back was associated with lack of engagement in regular physical activity (p = 0.036), bending (p = 0.025) and standing and bending (p = 0.022) working posture. Prevalence of WMSDs affecting the hip/thigh was associated with lack of engagement in regular physical activity (p = 0.003), and being of junior cadre position (p = 0.025). Prevalence of WMSDs affecting the knee was associated with strenuous job (p = 0.041), lack of engagement in regular physical activity (p = 0.030), being in junior cadre (p = 0.037), smoking (p = 0.016), and alcohol intake (p = 0.003). Furthermore, prevalence of WMSDs affecting the ankle or feet was associated with doing strenuous job (p = 0.043) and being in junior cadre (p = 0.047 (Table 6).
Table 6: Associations of work and personal characteristics with the annual prevalence of work-related musculoskeletal disorders. View Table 6
The extent to which depressive, anxiety and stress symptoms correlates with the reported pain in the 12-month and 7-day in all of the body anatomical sites was determined using the Spearman's rho correlation analysis (Table 7). Staff with positive caseness of depressive symptoms had significant but weak correlation with pain severity in the shoulder (r = 0.21; p = 0.014), lower back (r = 0.25; 0.010), knee (r = 0.25; p = 0.012), ankle/feet (r = 0.030), and multiple (r = 0.26; p = 0.007) 12-month WMSDs. Similarly, having anxiety problem led to significant but weak positive correlation with pain severity in the neck (r = 0.21; p = 0.036), shoulder (r = 0.22; p = 0.029), and in ankle/feet (r = 0.23; p = 0.020) regions. Shoulder pain severity among respondents with 7-day WMSDs was significantly associated with presence of anxiety symptoms (r = 0.21; p = 0.036). Also, psychological stress symptoms were significantly correlated with pain severity in the shoulder (r = 0.25; p = 0.010), lower back (r = 0.25; 0.011), knee (r = 0.28; p = 0.004), ankle/feet (r = 0.27; p = 0.006), and multiple (r = 0.24; p = 0.015) WMSDs (Table 7).
Table 7: Correlation between pain severity resulting from work-related musculoskeletal disorders and psychological impairment. View Table 7
This study was aimed to characterize and correlate psychological impairment, pain severity and Work-Related Musculoskeletal Disorder (WMSDs) among hospital maintenance engineers in a Nigerian tertiary hospital. The 12-month and 7-day prevalence of WMSDs were 71.8% and 42.7%. There is dearth of data on the prevalence of WMSDs among hospital engineering staff with which this study can be compared. However, the prevalence rates observed in this study were comparable to the findings reported among health workers in Nigeria [8,9,37,38] and globally [39-41]. A previous study among oil and gas engineering staff in the United Kingdom reported a prevalence of 80% and 37% for annual and weekly rates of WMSDs [29].
Work-related musculoskeletal disorders affecting the lower back was the most prevalent in both annual and weekly periods among hospital maintenance engineers in this study. Similar pattern of WMSDs have been reported among health workers [7,37-39,41-43] and engineering staffs [29,44]. The engineering staff in this study were involved in manual tasks and always assumed standing and bending postures while carrying out their duties. Bending has been reported as a major factor responsible for developing or aggravating low-back pain [45-47]. In addition, poor work environment and apparent lack of ergonomic standards in the Nigerian work environment may be responsible for the high prevalence of WMSDs among engineering staff in Nigerian health care settings. Ogunlana, et al. [9] reported that Nigerian health professionals work in environment that lack required ergonomic standards leading to debilitating effects on their wellbeing.
A significant number of engineering staff in this study reported more than one form of annual WMSDs. About 25% of the engineering staff had WMSDs in four or more anatomic sites (out of the total of nine body sites assessed). Having multiple WMSDs has been reported as a common phenomenon among engineering staff in the study by Parkes, et al. [29] among oil and gas workers in the UK. The most plausible reason for this phenomenon is that these categories of staff are involved in multi-tasking services that require more manual, physical environment stressors and manipulation of most body parts while carrying out the works [48].
In agreement with several previous studies [7-9,29,37,49,50], the findings of this study revealed that presence of ergonomic hazard increases the likelihood of developing WMSDs, and possibly increases the numbers of WMSDs an individual worker suffers from. Furthermore, some lifestyle choices including alcohol intake, cigarette smoking and not engaging in regular physical activity are found to be associated with reported work-related pain. Negative lifestyle factors like cigarette smoking and alcohol intake were reported to have significant association with developing musculoskeletal pain among the nurses [51,52], factory workers [53], software engineers [54], and bank employees [55]. Nicotine is a major risk factor for developing chronic pain [56]. Also, Micheletti, et al. [57] found that engaging in physical activity during leisure period was associated with lower risk of having musculoskeletal pain among the general working population in Denmark.
About 30% of the staff assessed had positive caseness of depression. The results of this study showed that presence of depressive symptoms increased the odds of having WMSDs. Depression and other related mental health problems have been implicated in the incidence of musculoskeletal dysfunction [13,14,58-60]. Conversely, anxiety and stress were not associated with any musculoskeletal complaint among the engineering staff. In this study, depressive symptoms were associated with only shoulder and upper back musculoskeletal pain and not to any site in the extremities. It has been previously reported that psychological impairment is common in individuals with incidence of musculoskeletal disorders in the upper body (neck, shoulder and upper back) than in the upper or lower extremities (i.e. arms, elbows, wrists, and hips, knees, ankles) [29,61-63]. Yadzi, et al. [11] have reported that musculoskeletal disorder in the neck and shoulder had direct association with psychological problems which was similar to the findings of this study.
The findings of this study showed that the staff' musculoskeletal pain severity is associated with presence of symptoms of depression, anxiety and stress. The results showed that increase in the scores of these psychological problems is associated with increase in the pain scores. Moreover, staff with higher pain intensity in the neck, shoulder, lower back, knee, ankle/feet, and as a result of multiple WMSDs were either significantly depressed, anxious or stressed. Depression and anxiety are associated with higher pain severity in individuals with musculoskeletal pain [59,64] and the more the psychological illness, the worse the physical pain [65]. Vargas-Prada and Coggon [10] submits that depressive symptoms are associated with higher levels of musculoskeletal pain intensity, and poor outcome in the management of musculoskeletal disorders and Yadzi, et al. [11] reported that psychological problems are higher in people with higher latent class of musculoskeletal pain. Psychological health problems were found to be significantly higher in workers with musculoskeletal pain than those without [66] while presence of depression and anxiety symptoms were identified as major risk factors to developing neck pain among general population [61] and were also involved in the presence of musculoskeletal pain in military personnel [67]. The results of a systematic review has also revealed that presence of knee pain is associated with anxiety and depression [68], and evidence has shown from randomized clinical trials that patients treated with antidepressant drugs had their musculoskeletal pain subsided [11]. Also, staff with multiple sites of WMSDs (4 or more WMSDs) in this study had a higher depression and stress symptoms which were significantly correlated with higher pain severity than those without multiple WMSDs. Patients with higher frequency or number of physical symptoms have been reported to be more likely to have psychological problems than those with nil or few numbers of physical problems [65].
It has been previously suggested that musculoskeletal disorders associated with psychological problems induce increased muscle tension or physiological changes that lead to pain [29,69]. Also, psychological stress is a precursor to physiological strain and muscle tension which may result into adverse effect on the immune system response [70]. Increased levels of psychological stress may induce individuals to undertake tasks differently in such a way that it generates abnormal biomechanical loading [71]. It is therefore plausible to infer that incidence and higher intensity of musculoskeletal pain are directly related to psychological problems since individuals with mental health problems are more prone to inflammation compared to those without psychological issues [11] and undertake tasks in a posture inimical to normal biomechanical functioning.
Explaining the relationship between musculoskeletal disorders or pain and mental health problems, some researchers have implicated the involvement of neurotransmitters [10,65] and cytokine receptors [72] in this. Depression is explained to be associated with dysfunction in inflammatory cytokine synthesis due to stress, and negatively affect autonomic cardiac functioning [73,74] thereby disrupting hypothalamic-pituitary-adrenal control [75]. Besides, it appears there is a shared neurologic pathway between pain and depression [76] because physical pain, which is regulated in the brain by serotonin and norepinephrine, also connect with mood and emotion through these neurotransmitters. This dysfunction or dysregulation in neurotransmission which apparently connect pain and depression may further explain why musculoskeletal pain is reduced in patients taking antidepressant medications that inhibit norepinephrine and serotonin reuptake [77]. Therefore, if this shared pathway is affected by any psychological illness, it may aggravate or perpetuate musculoskeletal pain or disorder.
Only 39.2% of those who reported WMSDs in this study sought help for their discomfort from any healthcare professionals despite that they were working in the hospital setting. There seems a poor healthcare seeking behavior among these health sector workers. A Nigerian study indicates that over 70% of health workers practiced self-medication with many of them expressed fear what the outcome of medical consultations will be and therefore abstain from seeking consultation for their health challenges [78]. In this study, psychological health problems were not associated with the healthcare seeking attitude of the staff, however, staff with lower back work-related musculoskeletal pain consulted a healthcare professional than for any other WMSD. Low-back pain, and even in just four weeks of onset, has been reported to be bad enough to limit activities of daily living or adversely affect work routine and leisure compared to other musculoskeletal pain [29,79,80] making the sufferers to seek for help. In this study, work (34.4%) and leisure (29.7%) were reportedly affected among the staff by symptoms of WMSDs which lower back is the most prevalent.
This study has some potential limitations. The data were collected from engineering staff of only one hospital. Although, the hospital is a large tertiary health facility. Also, the cross-sectional nature of the study makes it difficult to recall bias especially as it relates to remembering whether their musculoskeletal disorders were as a result of work or not, as well as the ability to rate severity of musculoskeletal pain. Furthermore, as this is a cross-sectional study, the significant association between psychological health and WMSDs observed in this study cannot be taken for a cause-effect relationship.
There is a high prevalence of WMSDs among hospital maintenance engineers and it is significantly associated with depressive, anxiety and stress symptoms. Therefore, it is imperative for the policy makers and clinicians to consider the broad implication of psychological health on WMSDs when formulating remediation programmes.
We appreciate all the staff in the Department of Works, Osun State University Teaching Hospital, Osogbo, Nigeria.
The study was self-funded by the authors.
No conflict of interest to declare.
Conception and design: ABA; Acquisition, analysis and interpretation of data: ABA, CEM, OAS, BYA, IAA, TAO; Drafting, critical revision and final approval of the manuscript: ABA, CEM, OAS, BYA, IAA, TAO, FF, HM, MIO.