Background and aims: Chronic rhinosinusitis (CRS) is a well-known heterogeneous disorder due to its potentially infectious status along with long-term inflammation of the nose, paranasal sinuses, and lining of the nasal passages, which lasts for 12 consecutive weeks or longer. Although the definite pathophysiological mechanism is not clear, recent studies have postulated bacterial infections with biofilm or fungal colonization as the pathophysiological mechanisms. Coronary heart disease (CHD) is a critical public health problem across developed countries worldwide. A newly published study has shown that patients with CRS were at a higher risk of acute myocardial infarction in a 6-year follow-up.
Methods: We conducted a population-based retrospective cohort study using data extracted from the Longitudinal Health Insurance Database of Taiwan from 2000 to 2010 (follow-up 2011). The database with a sample of 1 million cohorts was randomly selected from 23 million individuals. The study population comprised individuals who were first diagnosed with chronic sinusitis (International Classification of Diseases, Ninth Revision, Clinical Modification 473) since 2000, which was defined as the index day. Patients with ischemic heart disease were excluded from this study. In addition, the matched system was adjusted for age, sex, and the index year. In total, data on 13644 patients with CRS from 2000 to 2010 were extracted for the study cohort. The comparison groups were selected by matching patients with CRS in terms of age, sex, and the index year.
Results: The age of most patients with CRS was < 49 years. The comorbidities associated were diabetes mellitus (DM), hypertension (HTN), hyperlipidemia, asthma, chronic obstructive pulmonary disease (COPD), alcohol-related illness, and tobacco dependency. The cumulative incidence of CHD was significantly different between the patients with and without CRS. In addition, after adjusting for age, sex, and comorbidities such as DM, HTN, hyperlipidemia, asthma, stroke, COPD, alcohol-related illness, and tobacco dependency, the hazard ratio of CHD for individuals with CRS was 1.21 (95% confidence interval = 1.11-1.33) compared with individuals without CRS.
Conclusion: The findings of this study offer some points regarding the positive relationships between CRS and CHD.
Chronic rhinosinusitis, Coronary heart disease
Chronic rhinosinusitis (CRS) is a well-known heterogeneous disorder due to its potentially infectious status along with long-term inflammation of the paranasal sinuses and the lining of the nasal passages, which lasts for 12 consecutive weeks or longer [1-4]. Although the definite pathophysiological mechanism is not clear, recent studies have postulated bacterial infections with biofilm [3-6] or fungal colonization [3,7-9] as the pathophysiological mechanisms. Progressive inflammation and the biofilm can stimulate neutrophils, mononuclear cells, and type 2 T helper cells to release cytokines into the bloodstream and may cause acute myocardial infarction (AMI) and apoplexy [8]. Complications of CRS not only contribute to systemic disease but also decrease the quality of life and economically impact life [10,11]. Coronary heart disease (CHD) is a crucial public health problem across developed countries worldwide [12]. A recent study has shown that patients with CRS were at a higher risk of AMI occurrence in the 6-year follow-up [13]. However, whether the incidence of cardiovascular complications increased in untreated CRS remains unclear. This study aimed to answer this question using a population-based retrospective cohort study using the Taiwan Longitudinal Health Insurance Database (LHID).
Data for this retrospective cohort study were derived from the 2000-2011 LHID 2000 (LHID2000) established and managed by the Taiwan National Health Insurance (NHI) program for research purposes. Since March 1, 1995, the NHI program has provided approximately 99% of the 23.74 million residents with comprehensive and universal health care in Taiwan. The LHID2000 includes longitudinal data on medical claims for 1 million individuals randomly sampled from the NHI program. The details of the LHID2000 and NHI program have been described previously [14,15]. Disease status in the Taiwan NHI program was established using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM).
This retrospective cohort study included two cohorts: A CRS cohort and a non-CRS cohort. Participants in the CRS cohort were diagnosed with CRS between January 1, 2000 and December 31, 2010 (ICD-9-CM code 473). The index date for the CRS cohort was set as the day the diagnosis of CRS was established. Patients with a history of CHD (ICD-9-CM codes 410-414), those who underwent percutaneous transluminal coronary angioplasty (PTCA) (ICD-9-CM procedure codes 36.0, 36.01, 36.02, 36.05, 36.06, 36.09, and 36.2), those who underwent coronary angiography only without PTCA (ICD-9-CM procedure codes 37.21, 37.22, 37.23, and 37.29) before the index date, and those aged < 20 years were excluded from the study. The non-CRS cohort participants were selected from individuals without a diagnosis of CRS and those who did not have a history of CHD, PTCA, or coronary angiography only without PTCA before participating in the study. For the CRS cohort, the non-CRS cohort was established by 4-fold age- and sex-frequency matching, and the index date assigned was the same as that of the corresponding CRS cases.
The follow-up for the CRS and non-CRS cohorts started at the index date and terminated when the participants withdrew from the NHI program; died; until events such as CHD, PTCA, and coronary angiography only without PTCA occurred; or the end of December 31, 2011. The following baseline comorbidities were included: diabetes mellitus (ICD-9-CM code 250), hypertension (ICD-9-CM codes 401-405), hyperlipidemia (ICD-9-CM code 272), asthma (ICD-9-CM code 493), stroke (ICD-9-CM codes 430-438), chronic obstructive pulmonary disease (COPD) (ICD-9-CM codes 491, 492, and 496), alcohol-related illness (ICD-9-CM codes 291, 303, 305, 571.0, 571.1, 571.2, 571.3, 790.3, A215, and V11.3), and tobacco dependency (ICD-9-CM code 305.1).
Pearson's chi-square test was used for categorical variables, such as sex, age group (≤ 49 years, 50-64 years, and ≥ 65 years), and comorbidities, between the CRS and non-CRS cohorts. Continuous variables were analyzed using Student's t-test. The cumulative incidence of CHD between the CRS and non-CRS cohorts was assessed using the Kaplan-Meier method, and the differences were tested using a log-rank test. The overall sex-, age-, and comorbidity-specific incidence density rates (per 100 person-years) were calculated for each cohort. Univariable and multivariable Cox proportional hazard regression models were used to assess the risk of CHD development associated with CRS compared with that of the non-CRS cohort. The relative hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated using Cox models. For the multivariable model, the effects of age, sex, and the comorbidities of diabetes mellitus, hypertension, hyperlipidemia, asthma, stroke, COPD, alcohol-related illness, and tobacco dependency were controlled. Further analysis was performed to investigate whether surgery for CRS influenced the risk of CHD. All analyses were performed using the SAS software for Windows (version 9.4; SAS Institute, Inc., Cary, NC, USA). Statistical significance was set at P < 0.05.
This study surveyed 13644 patients with CRS and 54576 comparisons without CRS (Table 1). In this study population, 50.1% were females, and 70.7% of the study participants were aged ≤ 49 years. The proportions of baseline comorbidities, except for stroke, were significantly different between the CRS and non-CRS cohorts. Kaplan–Meier analysis results showed that the cumulative incidence curves of CHD were significantly higher in the CRS cohort than in the non-CRS cohort (log-rank test, P < 0.001; Figure 1). During the mean follow-up period of 6.83 years for the CRS cohort and 6.78 years for the non-CRS cohort, the overall incidence density rate of CHD was significantly higher in the CRS cohort than in the non-CRS cohort (1.26 vs. 0.90 per 100 person-years) with an adjusted HR (aHR) of 1.30 (95% CI = 1.22-1.39) after adjusting for age, sex, and comorbidities (Table 2). The aHR for CHD was higher in women (aHR = 1.38, 95% CI = 1.25-1.52) and men (aHR = 1.23, 95% CI = 1.12-1.35) in the CRS cohort than in the non-CRS cohort. The incidence of CHD increased with age in both cohorts. The age-specific relative risk of CHD in the CRS cohort compared with the non-CRS cohort was higher for all age groups. Compared with the non-CRS cohort, the patients in the CRS cohort exhibited a higher risk of developing CHD (patients without comorbidities, aHR = 1.34, 95% CI = 1.20-1.49 and patients with comorbidities, aHR = 1.17, 95% CI = 1.08-1.28).
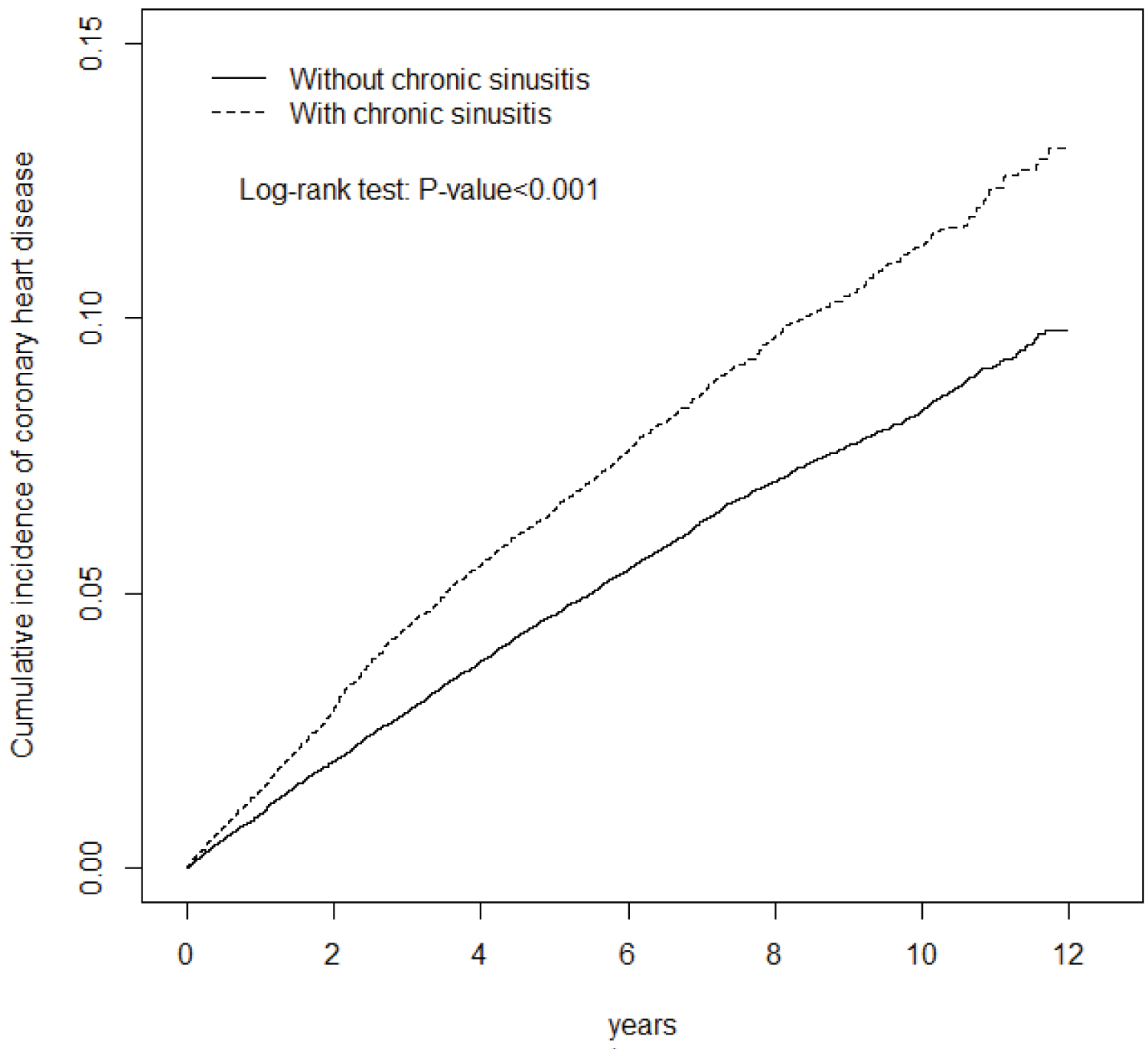 Figure 1: Cumulative incidence of coronary heart disease compared between patients with and without chronic rhinosinusitis using the Kaplan-Meier method.
View Figure 1
Figure 1: Cumulative incidence of coronary heart disease compared between patients with and without chronic rhinosinusitis using the Kaplan-Meier method.
View Figure 1
Table 1: Basic demographics. View Table 1
Table 2: Comparison of the incidence and hazard ratio of coronary heart disease stratified by sex, age, and comorbidities between patients with and without CRS. View Table 2
Compared with the patients without CRS, the risk of CHD was 1.16-fold (95% CI = 1.00-1.35) higher in the patients belonging to the CRS cohort who underwent surgery and 1.33-fold (95% CI = 1.24-1.43) higher in the patients who did not undergo surgery (Table 3). The risk of CHD between the patients with CRS who did and did not undergo surgery showed no significant difference (aHR = 0.88, 95% CI = 0.75-1.04).
Table 3: The incidence and hazard ratio of coronary heart disease among patients with CRS who did and did not undergo surgery compared with patients without CRS. View Table 3
Owing to the increasing trend of CRS in recent years, many studies have shown that this chronic inflammatory condition also has significant effects on other systems of the body; however, the detailed mechanism is unclear. Therefore, this study used the NHI system database for sampling to explore the association between CRS and CHD. From January 1, 2000 to December 31, 2010, 13644 patients diagnosed with CRS were included in this study. Most of the participants were middle-aged individuals, and 70.7% of the participants were younger than 49 years. This may be due to the nature of diseases, which are more likely to occur earlier in human life. In our statistical analysis, it was also found that women were more likely to have CRS than men, (aHR, 1.38 vs. 1.23, respectively) which was consistent with the results of previous studies [16,17]. Although men are more likely to smoke than women, women are more likely to have access to medical care or be more alert than men and, therefore, more likely to be diagnosed with the disease [18]. As shown in Table 2, after controlling for the variables of the comorbidity, the risk of CHD in the CRS cohort was 1.34 times higher than that in the non-CRS cohort after adjustment.
While investigating patients with CRS who did or did not undergo sinus surgery, it was found that there was no significant difference in the occurrence of CHD in the patients who did or did not undergo sinus surgery, which was inconsistent with our initial hypothesis. We assumed that CRS is associated with cardiovascular disease because of long-term inflammation. If this is the cause, then the source of chronic inflammation will be eliminated after sinus surgery; therefore, the incidence of CHD should be almost the same as that in the normal population. However, our study found that this was not the case. One possible reason may be the endogenous allergic disease of the patient. In the rhinosinusitis classification, the CRS group with nasal polyps accounted for more than half of the patients. The pathophysiology of this group is highly complex, and patients often have coexisting airway diseases, such as allergies and asthma, in addition to CRS. Although we lowered the level of sinus inflammation by surgery, the accompanying allergy may still cause chronic inflammation in the human body. Another reason is that, in patients with CRS, the pro-inflammatory substances and cytokines produced during chronic inflammation may have already resulted in adverse effects on the cardiovascular system. In addition, among patients with CRS, those who ultimately underwent sinus surgery may have had more severe disease and thus more severe inflammatory reactions than those who did not undergo sinus surgery. Although we did not observe a statistically significant difference, the HR demonstrated a higher risk of CHD in patients with CRS who did not undergo sinus surgery than in patients with CRS who underwent sinus surgery.
CRS is a threatening disease that affects the patient's quality of life and exerts an economic burden on the government. Although it is well known that long-term inflammatory conditions lead to the activation of immune cells and the release of cytokines, the exact mechanism is not fully understood. Our study showed that CRS was significantly associated with CHD. Our study also found that women with CRS are more likely to develop CHD than men, and aggressive surgical treatment seems to be protective; although, there was no statistically significant difference in the incidence of CHD. Patients with CRS may be more alert to their cardiovascular conditions.
None declared.
None declared.