Bechet's, Mycoplasma pneumoniae
A 20-year-old female with recurrent childhood ear infections, and reported history of recurrent oral, genital ulcerations and UTIs, presented as transfer from outside hospital with concern for Behcet syndrome. The patient initially had a 3-4-month history of fever, oral and genital ulcerations and worsening respiratory symptoms. She was initially treated at urgent care with antivirals and nitrofurantoin. She was later admitted to an outside hospital with worsening of aforementioned symptoms and respiratory failure, briefly in ICU for worsening respiratory status. She was treated with Zosyn and fluconazole with some improvement.
On transfer to UNM, patient was febrile at 101F. She had rash over neck (Figure 1A), mucositis of lips and buccal mucosa (Figure 1B) as well as conjunctivitis (Figure 1C) described by patient as "bloody tears". Infectious workup was positive for mycoplasma IgM; chlamydia serologies negative; autoimmune panel negative. CT chest showed multifocal bronchiolitis/bronchopneumonia. The shave biopsy of lip was suggestive of nonspecific ulceration. Patient was seen by Ob/Gyn but there was no evidence of vulvar or vaginal lesions on colposcopy exam at that time and no area amendable to biopsy. Ophthalmology found no concerning evidence of retinal vasculitis, nor was there evidence of anterior/posterior uveitis. She did have severe bilateral conjunctival injection, which could be concerning for early scleritis/episcleritis.
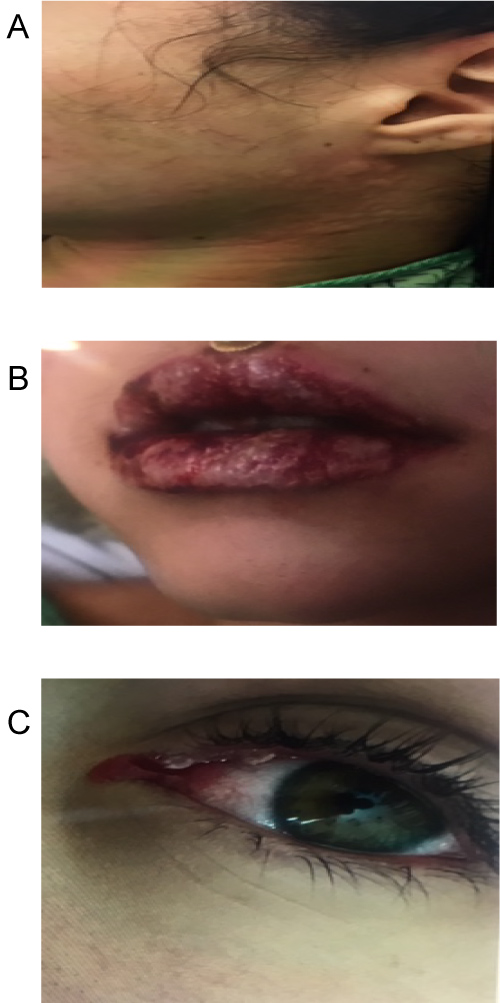 Figure 1: Patient with MIRM. A) Rash over neck; B) Mucositis of lips and buccal mucosa; C) Conjunctivitis.
View Figure 1
Figure 1: Patient with MIRM. A) Rash over neck; B) Mucositis of lips and buccal mucosa; C) Conjunctivitis.
View Figure 1
A diagnosis of mycoplasma-induced rash and mucositis (MIRM) was made. She was discharged with 3-day course of Azithromycin and prednisolone 50 mg once daily for 3 days with taper for 3 weeks with almost complete resolution.
MIRM is a relative new entity [1,2]. It affects mostly children, mostly males and rarely adults. Patients typically present with 2 to 3 affected mucosal sites with almost universal oral involvement and sparse skin involvement [3]. Histopathology features are in line with SJS/TEN [4]. Treatment is with antibiotics targeting mycobacterium pneumoniae and systemic/oral steroids depending on mucosal involvement [5]. Patients usually have favorable outcome with little chances of recurrence.